Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Xinbo58.com2
Effect of sertraline on the recovery rate of cardiac autonomic function in depressed patients after acute myocardial infarction Allan McFarlane, MD,a Markad V. Kamath, PhD,b Ernest L. Fallen, MD,b Victoria Malcolm, RN,b Finu Cherian,a and Geoff Norman, PhDc Hamilton, Ontario, Canada Background Brain serotonin is known to possess sympathoinhibitory properties. The aim of this clinical physiologic study was to determine whether sertraline, a selective serotonin reuptake inhibitor, facilitates the rate of recovery of cardiac autonomic function after an acute myocardial infarction (MI) in patients with depression. Methods and Results Thirty-eight post–MI depressed patients were randomized to receive either sertraline 50 mg per day or placebo for 6 months. Depression was defined as a score >15 on the standardized Inventory to Diagnose Depression questionnaire taken at prehospital discharge and again within 2 weeks of the acute infarct. Eleven stable post- MI nondepressed patients served as a nonrandomized reference group during follow-up. Twenty-seven patients completed the randomization. All 3 groups were followed up closely in a multidisciplinary post-MI clinic where they underwent serial testing for both time and frequency domain heart rate variability (HRV) indices at baseline (1-2 weeks after MI) and at 6, 10, 14, 18, and 22 weeks. The rate of recovery of HRV was determined by use of a growth curve model based on repeated-measures analysis of variance. There was a linear rate of increase in the SD of 24-hour N-N intervals (SDNN) in the sertraline-treated group that paralleled that of the nondepressed reference group. This contrasted with a modest but sig- nificant decline in SDNN in the placebo group from 2 to 22 weeks (t = 2.10, P < .05). However, the short-term power spec- tral indices, while trending toward a more rapid rate of recovery in the treated group, did not reach statistical significance compared with the placebo group. Conclusion In depressed patients who have survived the acute phase of an MI sertraline facilitates the rate of recovery of SDNN, a recognized predictor of clinical outcome. (Am Heart J 2001;142:617-23.)
Major and minor depressive disorders are common,
depressant treatment has been fully elucidated.
with lifetime prevalence rates of 5% and 13%, respec-
Although depressed patients may be vulnerable by
tively.1 It is now recognized that depressed patients hav-
virtue of occasional noncompliance in following pre-
ing an acute myocardial infarction (MI) are particularly
scribed treatment, it is highly unlikely that this factor
predisposed to major adverse outcome within the first
alone could explain the magnitude of the interaction.
year of the acute event.2,3 In a recent study Frasure-
From a neurochemical perspective, depressed
Smith et al reported an 18% and 27% incidence of major
patients often have a chronically heightened sympa-
and minor depression, respectively, in patients recover-
thetic state.5 This has been attributed to putative mech-
ing from an acute MI.4 Moreover, the hazards ratio for
anism such as β-adrenoreceptor down-regulation and
death within 6 months of the acute event was 5-fold
abnormal 5-hydroxytryptamine (5-HT) receptor activity
among a depressed compared with a nondepressed
in the brain.5,6 It is now known that brain serotonin, a
cohort. Although this association is a matter of growing
neurotransmitter with central sympathoinhibitory prop-
concern, neither the mechanisms nor the effect of anti-
erties, is reduced in depression and could result in over-expression of sympathetic neural discharge.7
Heart rate variability (HRV) offers a unique noninva-
From the Departments of aPsychiatry, bMedicine, and cClinical Epidemiology andBiostatistics, McMaster University Faculty of Health Sciences, Hamilton, Ontario,
sive window through which to visualize the effects of
centrally mediated changes in autonomic modulation of
Supported by a peer-reviewed grant from the Heart and Stroke Foundation of
cardiac function.8 It follows that by use of this technol-
ogy it is possible to assess changes in cardiac sympatho-
Submitted September 15, 2000; accepted April 26, 2001. Reprint requests: Allan McFarlane, MD, McMaster University Medical Centre,
modulation over time, using serial changes in HRV. Room 3G 16, 1200 Main St W, Hamilton, ON L8N 3Z5, Canada.
Interestingly, it is known that reduced HRV, one of the
consequences of sympathoexcitation, is, as in depres-
sion, an independent predictor of mortality within the
first year of an acute MI.9 Moreover, several studies have
618 McFarlane et al
demonstrated a shift in sympathovagal balance toward a
All 3 groups had baseline measurements of HRV 2 weeks
heightened sympathetic state in patients with depres-
after MI before sertraline or placebo was initiated. These
sion.10-12 Our working model presumes that linkages
included short-term supine and standing power spectral
exist between the stress of an acute MI, either onset or
indices of HRV under controlled laboratory conditions as well
exacerbation of depression, cardiac autonomic imbal-
as time domain statistics derived from 24-hour ambulatoryelectrocardiogram (ECG) Holter recordings. All 3 groups were
ance, and adverse clinical outcomes. Several studies have
then followed up by one nurse practitioner (V. M.) in a special
demonstrated a gradual recovery of cardiac autonomic
post-MI clinic (PMIC) at McMaster University Medical Centre
function within 2 to 12 months after an acute MI.13,14
for 6 months. The PMIC is a multidisciplinary clinic with uni-
Given that most serious outcome events occur within
form standards of follow-up care for those discharged from
the first 6 months of hospital discharge, it is reasonable
our CCU, providing access to exercise rehabilitation, nutri-
to assume that any intervention that rapidly returns auto-
tional counseling, smoking cessation programs, and support-
nomic balance in patients with persistent depressive
ive psychotherapy. Hence all 3 groups received the same
symptoms could stabilize the heart, thereby rendering it
level of care throughout in the same clinic with the same
less vulnerable to malignant ventricular arrhythmias. In
caretaker(s). Each patient underwent identical 24-hour Holter
this randomized, placebo-controlled clinical physiologic
and laboratory testing at 2, 6, 10, 14, 18, and 22 weeks afterMI. IDD testing was repeated at 6, 10, 18, and 22 weeks. The
study, we set out to determine the effect of sertraline, a
research protocol was approved by the Institutional Review
selective serotonin reuptake inhibitor (SSRI), on the rate
Board of the Faculty of Health Sciences of McMaster Univer-
of recovery of heart rate variability in depressed patients
sity. All patients gave written informed consent.
The IDD is a self-completion instrument developed by Zim-
merman et al.15 It covers all Diagnostic Statistical Manual’s crite-
Between September 1996 and March 1999, 238 patients
ria for major depressive disorder. It uses thresholds to determine
admitted with an acute MI to our coronary care unit (CCU)
the presence or absence of symptoms, each item being graded
completed a standardized questionnaire designed to assess
for severity as well as duration. The IDD is highly reliable with a
depression. Eighty-six percent or 36% scored above a predeter-
sensitivity of 81% to detect major depressive disorder. It corre-
mined threshold that satisfied criteria for inclusion of both
lates well with the Beck Depression Inventory (0.87), the Hamil-
minor and major depression. Of these, 38 (44%) agreed to
ton Rating Scale (0.80), and the Depression Interview Schedule
enter a double-blind, randomized, placebo-controlled trial of
(κ 0.9). The IDD is especially useful in measuring severity of
sertraline 50 mg per day for 6 months. Eleven dropped out
depressive symptoms with changes over time.16
after randomization within the first 2 months (6 in the sertra-line group and 5 in the placebo group), 3 because of drug side
effects, 7 because of noncompliance, and 1 because of fre-
For the time domain analysis, each 24-hour Holter tape was
quent ventricular ectopy. Of the 27 patients who completed
first annotated with an Oxford Medilog Excel scanner. A beat-
the study, the average age was 62 ± 11 (SD) years and 16% or
to-beat recognition software algorithm was assigned a configu-
59% were male. Eleven age-matched nondepressed post-MI
ration class to each QRS complex. The normal sinus-conducted
patients (9 male, age 62 ± 12 years) served as a nonrandomized
N-N interbeat intervals were then downloaded for offline com-
reference group to ascertain the “normal” rate of recovery of
putational analysis. This included the average heart rate, the SD
cardiac autonomic function in an otherwise nondepressed
of all 24-hour N-N intervals (SDNN), and the root mean square
cohort. Excluded were patients whose predischarge 24-hour
of the SD of successive N-N intervals (rMSSD). The power
Holter recordings showed either atrial fibrillation or ventricular
spectrum of HRV was computed by autoregressive modeling.
ectopic beats greater than 100 per hour. Also excluded were
This test was performed under carefully controlled laboratory
patients with overt congestive heart failure, any life-threaten-
conditions with a customized acquisition analog-to-digital sys-
ing comorbid condition, an inability to complete the question-
tem. A full description of our method can be found in a previ-
naire, and those already on antidepressant medications.
ous report.17 In brief, the filtered ECG signal (2.2 minutes)was digitized with a 12-bit analog-to-digital converter at a sam-
pling rate of 1 kHz. The instantaneous heart rate series was
The design was a double-blind, randomized, placebo-con-
resampled by linear interpolation to obtain an equally sampled
trolled trial with stratification before randomization for those
signal spaced 0.5 seconds apart. The power spectrum was
on β-blocker therapy. Patients meeting the inclusion criteria for
then computed from the HRV data of 256 samples. An autore-
randomization had to score >15 on the Inventory to Diagnose
gressive model of order number 14 was fitted to the HRV sig-
Depression (IDD) questionnaire (vide infra) at least twice, once
nal. Both the peak amplitude and the normalized area power
just before hospital discharge and again 2 weeks later. This was
contained in the low-frequency (LF) (0.05-0.15 Hz) and the
to ensure stability in their mood alteration. The 38 patients
high-frequency (HF) (0.15-0.40 Hz) bands were derived.
were then randomized to receive either sertraline 50 mg a day
Because of anticipated low energies in signals from patients
or a matched placebo tablet. There was, in addition, a third
with poor left ventricular (LV) function, all patients were stud-
group, a nondepressed nonrandomized reference group (n =
ied in both the supine (20-30 minutes) and standing (10 min-
11) whose IDD score had to be less than 15.
utes) positions to maximize the signal-to-noise ratio in the LF
American Heart JournalVolume 142, Number 4
McFarlane et al 619 Table I. Baseline demographics and clinical data Sertraline Placebo P Parameter
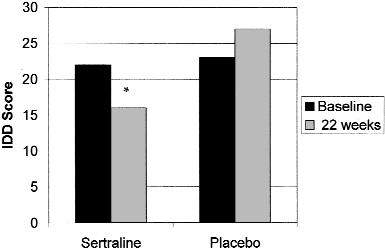
IDD scores for sertraline-treated and placebo groups at base-
line and at 22 weeks after MI. Asterisk, Significant drop in
All values are expressed as mean with SD in parentheses. NS, Not significant at P =.05.
active treatment and placebo groups, respectively. There were no significant group differences for risk fac-tors, cardiac medications, revascularization procedures,
band as well as to assess, indirectly, a measure of baroreceptor
thrombolysis, or history of previous MI. The IDD scores
(range 16-43) averaged 21 ± 6.7 and 23 ± 6.4 for thesertraline and placebo group, respectively. It was only
in the sertraline-treated group that a significant
The primary outcome measurements were the time-depen-
decrease in IDD scores (21 to 16, P < .05) was seen at
dent changes in both time and frequency domain parameters
of HRV. To estimate the rate of recovery of autonomic func-
Similarly, there were no significant baseline differences
tion, we used a growth curve model based on a repeated-mea-
in any of the HRV measurements between the study
sures analysis of variance (ANOVA).18 With this method the
groups (Table II). There appeared to be a more robust
data are fitted to a linear equation containing a polynomial
HRV in the nondepressed reference group whose
function of time, dummy variable for the sertraline versusplacebo group, and interactions. The functional form was
reduced LF/HF ratio, slower heart rate, and higher rMSSDsuggest a comparatively higher vagal state. These baseline
Y = b0 + b1 (X) + b2 t + b3 (t × X),
differences, however, did not reach statistical signifi-
where X is a dummy variable equal to 0 for the placebo group
cance. On the other hand, there was a distinct difference
and 1 for the sertraline group and t is elapsed time from initia-
between the depressed patients and their nondepressed
tion of treatment. Initial analysis also included quadratic and
counterparts with respect to the ability to mount a
cubic terms (and interactions), but these were not significant
baroreceptor-mediated response to orthostatic stress (Fig-
and were omitted from the reported analysis. Finally, a test of
ure 2). Although only 1 nondepressed patient failed to
significance was conducted by dividing each coefficient by its
increase his LF power on standing erect, >50% (16/27) of
SE. The analyses were conducted by use of a standard statisti-
the depressed group actually exhibited an abnormal
cal package (BMDPV, Los Angeles, Calif). All data are expressed
decrease in LF power with orthostasis (P < .05).
as mean ± SEM. Baseline differences were analyzed by 1-way
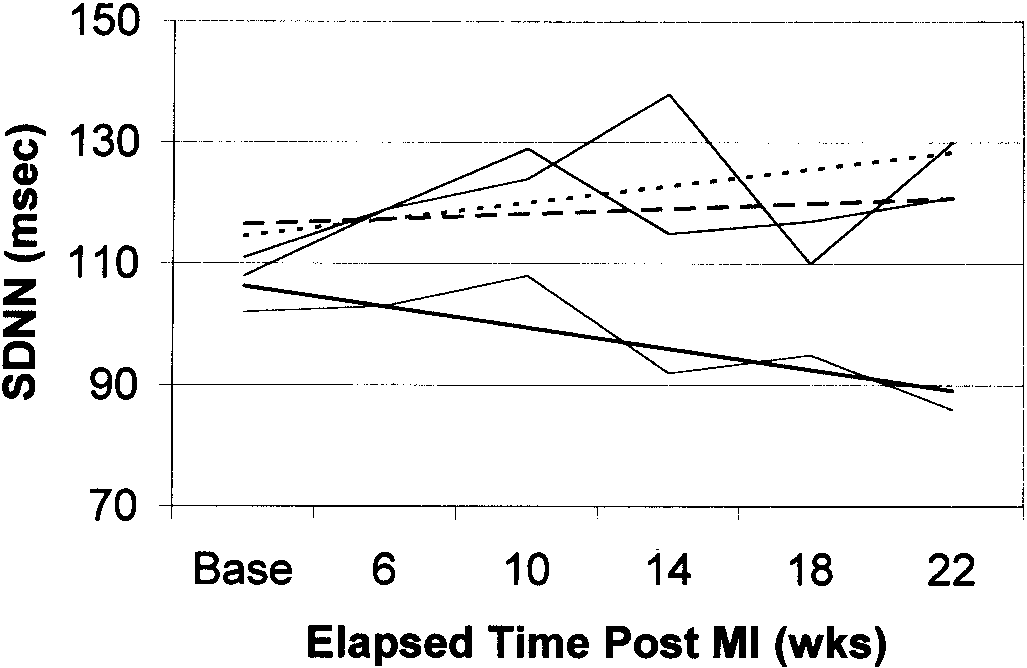
The most striking finding was an increase in SDNN in
ANOVA and comparisons of the direction of orthostatic changesin LF power between the depressed and nondepressed refer-
the sertraline-treated group in contrast to the steady
ence group were computed using χ2 analysis. A value of P < .05
decline in SDNN in the placebo group (Figure 3 and
Table III). During the 22 weeks after the acute infarction,the average SDNN for the sertraline group increased amodest 5% from 110.6 ± 10.1 milliseconds to 115.4 ±
11.0 seconds. Conversely, the depressed patients treated
Baseline demographic and clinical characteristics
with placebo showed a 9% decrease in SDNN. This dif-
were similar between the sertraline and placebo groups
ference in the trends of the sertraline versus placebo
(Table I). Both groups had well-preserved LV function
groups was confirmed by growth curve analysis where
with ejection fractions averaging 53% and 58% for the
the test of the group × time interaction was significant
620 McFarlane et al Table II. HRV data at baseline Parameter Sertraline (n = 12) Placebo (n = 15) Reference (n = 11) P value
Values are expressed as mean with SEM in parentheses. NS, Not significant at P = .05; nu, normalized units.
Comparison of the orthostatic responses of the LF power
Growth curve plots of the rate of recovery of SDNN (in mil-
between the depressed (n = 27) and nondepressed (n = 11)
liseconds) conform to a linear model represented by the sertra-
groups at baseline. Solid bars, Depressed group; open bars,
line (dashed line), placebo (solid line), and nondepressed (dot-
nondepressed group. Positive and negative refer to directional
ted line) groups. Base on the abscissa refers to baseline (2
changes (increases or decreases respectively) of the LF power
weeks after acute MI). The differences in rate of recovery
from supine to standing states. There were significantly more
between the sertraline-treated and placebo group are statisti-
abnormal responses (ie, a fall in LF power on standing) in the
cally significant (t = 2.10, P < .05).
depressed group (χ2 P < .05).
either of the depressed groups throughout the follow-up period (Table III).
(t = 2.10, P < .05). In all instances the same individual
At the end of 6 months there was a 26% reduction in
patients contributed to the mean values at every time
IDD scores in the sertraline group (22.25 ± 2.0 to 16.5
period. During this same interval, it can be seen that the
± 1.5, P < .05) compared with no change in the
nondepressed group showed a 28% increase in SDNN
placebo group (23 ± 2.1 to 27 ± 8). However, there
from 108 ± 8.6 to 138 ± 12 milliseconds.
was no significant correlation between the baseline
Although no significant group differences were seen
IDD scores and any of the HRV measurements. Neither
in time trends for any of the remaining HRV parame-
was there a correlation between changes in IDD scores
ters (Table III) there were nevertheless 2 interesting
over time and time-dependent changes in any HRV
observations. First, in all 3 groups both time and fre-
index. Although it was not the purpose of the study to
quency domain HRV indices were not static but dis-
measure clinical outcomes, the sample size being too
played linear trends over time, indicating a progressive
small, we note there were no deaths in any of the
recovery toward normalization of autonomic balance.
groups during 6 months of follow-up, and the number
Second, although sertraline did not appear to influence
of patients requiring readmission for either unstable
the rate of recovery of either the LF/HF ratio or the
angina or reinfarction was too small to draw any statisti-
resting supine LF power in the depressed groups,
cal inferences. Of note, sertraline was well tolerated
there was a persistent and significant reduction in LF
with no adverse reactions or clinical symptoms among
power indices in the nondepressed compared with
American Heart JournalVolume 142, Number 4
McFarlane et al 621 Table III. Time course of HRV data Weeks after MI Parameter Baseline P value NS, Nonsignificant between groups and with respect to rate of recovery. *Statistically significant with respect to rate of recovery between sertraline and placebo groups. †Significance only between nondepressed and both depressed groups. Discussion
been shown that stimulation of central 5-HT1A recep-
This study shows that, in depressed patients after
tors can also lead to sympathoexcitation.23
acute MI, sertraline facilitates the rate of recovery of
Autonomic regulation of cardiac function is usually
SDNN, a potent predictor of cardiac mortality. For the
expressed by noninvasive measurements of HRV. Both
sertraline-treated group the trend toward restoring
time and frequency domain indices of HRV are power-
autonomic balance paralleled that of the nondepressed
ful independent predictors of mortality within the first
group. These rates of recovery were not dissimilar from
year after MI.9,24 A relationship between depression
those reported by Bigger et al13 and Lombardi et al.14
and HRV has also been well documented. Carney et al25
Conversely, the depressed group on placebo demon-
reported that HRV, expressed as SDNN, was signifi-
strated a modest but persistent decline in SDNN
cantly lower in patients with coronary disease with
throughout the 6 months of follow-up.
depression compared with nondepressed patients even
Much has been written about the worrisome impact
after correction for known covariates. Rechlin et al,10
of depression on adverse outcomes after MI.20 Post hoc
using both time and frequency domain measures in
analysis of data from several large clinical trials shows a
patients with major depression, reported significantly
strong correlation between psychosocial factors and
lower values of SDNN and HF (vagal) power with little
cardiac outcome events including sudden death.19,20
or no differences seen in a control group with reactive
These and other studies support previous claims that
depression confers a mortality risk as high as 4- to 6-
Given these observations, one could make a case that
fold within a year or so of an acute MI.21,22 Depression
because antidepressants significantly improve HRV
therefore emerges as a potent risk factor even after cor-
parameters they should, at least theoretically, improve
rection for known covariates such as LV dysfunction,
clinical outcomes. Much depends on the cardiovascular
previous MI, and ventricular arrhythmias.
effects of antidepressants generally and their influence
A causal link is harder to unravel. In terms of physio-
specifically on cardiac autonomic regulation. In con-
logic mechanisms, it is now accepted that depression is
trast to tricyclic antidepressants, which can cause
associated with a heightened sympathetic state.5 This
tachyarrhythmias, the SSRIs are well tolerated and pos-
may be related to down-regulation of central postsynap-
sess no anticholinergic effects and no effect on periph-
tic β-adrenoreceptors or changes in activity of sero-
eral autonomic tone such as postural hypotension, and
tonin 5-HR2 receptors in the brain.6,23 With depression,
they are not proarrhythmic. Balogh et al26 studied the
chronic depletion of neurotransmitters such as sero-
effects of antidepressants on SDNN and rMSSD in 17
tonin in central synaptic clefts could lead to interrup-
patients with a major depressive disorder over 4 to 8
tion of inhibitory inputs to central sympathetic centers,
weeks. Although they reported changes in SDNN that
thereby increasing sympathetic neural discharge. It has
correlated positively with improvement in depression
622 McFarlane et al
scores, especially with nontricyclics, the predrug HRV
that sertraline had no effect on the chronotropic
indices did not predict drug response nor was there
response to exercise in patients on β-blocker therapy.
any correlation between HRV and depression scores,
One of the major problems with drawing comparisons
findings similar to our treatment group. Kharykin et al27
between studies that use different methods is the lack
compared the effect of both doxepine and fluoxetine
of a common gold standard, a problem particularly per-
on 24-hour HRV measurements over 6 weeks. Using the
tinent to both HRV measurements and instruments for
Hamilton Depression Rating Scale they found that
diagnosing depression. In this respect, measures of
among the 10 of 14 patients responding to treatment
HRV parameters in this report assiduously followed the
there was a 17% increase in SDNN, whereas an actual
guidelines recommended in the task force report of
decrease in SDNN was seen in the nonresponders.
Although their population was noncardiac, our study
In conclusion, our study shows that sertraline, a cen-
showed similar findings in post-MI patients insofar as a
tral serotonin reuptake inhibitor, facilitates the rate of
significant increase in SDNN was observed in the sertra-
recovery of HRV, an expression of cardiac autonomic
line treatment in post-MI patients whereas an actual
function, in depressed patients after an MI. The clinical
decrease in SDNN occurred over time in the placebo
relevance of these findings deserves comment. There is
group. In an interesting study of patients with panic
often a tendency to ascribe a critical physiologic role to
disorder, Tucker et al28 observed a positive effect of flu-
potent prognostic variables such as HRV as if iatrogenic
oxetine on baroreceptor responsiveness as determined
modification of the variable would necessarily have an
by the LF power response to orthostasis. We saw a
impact on prognosis. This may or may not be the case
trend toward an increase in the orthostatic effect on LF
because the variable may simply be a surrogate or
power over time, but the differences between the ser-
epiphenomenon rather than a direct precipitant of out-
traline-treated and placebo groups did not reach statisti-
come events. Given this caution, the results reported
cal significance. Of interest, however, was the distinct
here nonetheless help advance the notion that SSRIs
impairment of the orthostatic (baroreceptor) response
may play an important therapeutic role for susceptible
in both depressed groups before randomization. These
depressed patients recovering from an acute MI.
findings lend credence to the notion that early treat-
Accordingly, they are worthy of being tested in larger
ment of depression significantly improves HRV parame-
ters, a known risk factor for adverse post-MI outcomes.
Potential limitations of this study deserve comment. References
First, the autonomic changes seen with sertraline were
1. Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12 month
not evident for all HRV parameters. For instance, there
prevalence of DSM III-R psychiatric disorders in the United States.
were only modest changes in rMSSD for any group. It
should be noted, however, that rMSSD is a differencing
2. Cleophus JM. Depression and myocardial infarction: implications
method that primarily characterizes vagally mediated
for medical prognosis and options for treatment. Drugs Aging
responses. It is of interest, therefore, that both de-
pressed cohorts exhibited lower rMSSD values com-
3. Musselman DL, Evans DL, Nemeroff MD. The relationship of depres-
pared with the nondepressed group consistently
sion to cardiovascular disease. Arch Gen Psychiatry 1998;55:580-
throughout the follow-up period. Although the power
spectral measurements were performed under labora-
4. Frasure-Smith N, Lesperance F, Talajic M. Depression following
myocardial infarction: impact on 6 month survival. JAMA 1993;55:
tory-controlled conditions to ensure stationarity, it is
important to be aware they are known to have less
5. Carney RM. Depression and the heart. JAMA 1996;276:1122-7.
intraindividual reproducibility over time compared
6. Bennett JP. Drugs for affective (mood) disorders. In: Brody TM,
with the more robust SDNN.29 The LF power for
Larser J, Minneman KP, et al, editors. Human pharmacology. St
instance, whether normalized or no, represents a small
Louis: Mosby–Year Book; 1994. p. 333-43.
portion (about 4%) of the total power contained in the
7. Meltzer H, Lowy MT. The serotonin hypothesis of depression. In:
daily 24-hour signal. And yet this index, primarily of
Meltzer HY, editor. Psychopharmacology: the third generation of
sympathetic origin, did decrease over time for both
progress. New York: Raven Press; 1987. p. 513-26.
depressed groups and paralleled the LF changes seen in
8. Kamath MV, Fallen EL. Power spectral analysis of heart rate vari-
the nondepressed group. More than 60% of the patients
ability: a non-invasive signature of cardiac autonomic function. CritRev Biomed Eng 1993;21:245-311.
were on β-blockers. It is well known that these agents
9. Kleiger RE, Miller JP, Bigger JT, et al. Decreased heart rate variabil-
can attenuate the power contained in the LF band30,31
ity and its association with mortality after myocardial infarction. Am
and thus may have influenced the modest changes seen
in the power spectral indices. For this reason we took
10. Rechlin T, Weis M, Spitzer A, et al. Are affective disorders associ-
care to stratify all patients on β-blockers before random-
ated with alterations in heart rate variability? J Affect Disord 1994;
ization. Apropos any possible interaction between SSRI
agents and β-blockers, Ziegler and Wilner32 showed
11. Carney RM, Rich MW, Tevelde A, et al. The relationship between
American Heart JournalVolume 142, Number 4
McFarlane et al 623
heart rate, heart rate variability and depression in patients with
HT activates 5-HT1A receptors to cause sympathoexcitation. Br J
coronary artery disease. J Psychosom Med 1988;32:159-64.
12. Yeragani VK, Pohl R, Balon R, et al. Heart rate variability in patients
24. Farrell TG, Bashir Y, Cripps T, et al. Risk stratification for arrhythmic
with major depression. Psychiatry Res 1992;37:35-46.
events in postinfarction patients based on heart rate variability. J
13. Bigger JT, Fleiss JL, Rolnitzky et al. Time course of recovery of heart
period variability after myocardial infarction. J Am Coll Cardiol
25. Carney RM, Saunders RD, Freedland KE, et al. Association of
depression with reduced heart rate variability in coronary artery
14. Lombardi F, Sandrone G, Pernpruner S, et al. Heart rate variability
disease. Am J Cardiol 1995;76:562-4.
as an index of sympathovagal interaction after acute myocardial
26. Balogh S, Fitzpatrick DS, Shelton BGS, et al. Increases in heart rate
infarction. Am J Cardiol 1987;60:1239-45.
variability with successful treatment in patients with major depres-
15. Zimmerman M, Coryell W, Corenthal C, et al. A self-report scale to
sive disorder. Psychopharm Bull 1993;29:201-6.
diagnose major depressive disorder. Arch Gen Psychiatr 1986;73:
27. Kharykin Y, Dorian P, Baker B, et al. Autonomic correlates of antide-
pressant treatment using heart rate variability analysis. Can J Psychi-
16. Zimmerman M, Coryell W. The Inventory to Diagnose Depression
(IDD): a self report scale to diagnose major depressive disorder. J
28. Tucker P, Adamson P, Miranda R, et al. Paroxetine increases heart
rate variability in panic disorder. J Clin Psychopharm 1997;17:
17. Venkatesh G, Fallen EL, Kamath MV, et al. Double blind placebo
controlled trial of short term transdermal scopolamine on heart rate
29. Kleiger RE, Bigger JT, Bosner MS, et al. Stability over time of vari-
variability in patients with chronic heart failure. Heart 1996;76:
ables measuring heart rate variability in normal subjects. Am J Car-
18. Rogosa D, Brandt D, Zimowski M. A growth curve approach to the
30. Cook JR, Bigger JT, Kleiger R, et al. Effect of atenolol and diltiazem
measurement of change. Psych Bull 1982;92:726-48.
on heart rate variability in normal persons. J Am Coll Cardiol
19. Ahern DK, Gorkin L, Anderson JL, et al. Biobehavioural variables
and mortality or cardiac arrest in the cardiac arrhythmia pilot study
31. Kamath MV, Fallen EL. Diurnal variations in neurocardiac rhythms
in acute myocardial infarction. Am J Cardiol 1991;68:155-60.
20. Schleifer SJ, Macari-Hinson MM, Coyle DA. The nature and course
32. Ziegler MG, Wilner KD. Sertraline does not alter the beta adrener-
of depression following myocardial infarction. Arch Intern Med
gic blocking activity of atenolol in healthy male volunteers. J Clin
21. Frasure-Smith N, Lesperance F, Talajic M. Depression and 18
33. Task Force on Heart Rate Variability. Standards of measurement,
month prognosis after myocardial infarction. Circulation 1995;91:
physiological interpretation and clinical use. Eur Heart J 1996;17:
22. Travella JI, Forrester AW, Schultz SR, et al. Depression following
34. Shapiro PA, Lesperance F, Frasure-Smith N, et al. An open label
myocardial infarction: a one year longitudinal study. Int J Psychiatry
preliminary trial of sertraline for treatment of major depression after
acute myocardial infarction (the SADHAT trial). Am Heart J 1999;
23. Anderson IK, Martin GR, Ramage AG. Central administration of 5-
Koskiniemi Marjaleena Publications Pietiläinen-Nicklén Jenna, Oskari Virtanen, Pekka Kolehmainen, Maija Lappalainen, Lass Uotila, Oili Salonen, Markus Färkkilä, Marjaleena Koskiniemi ADEM and virus infection. J Clin Virol. In Press Jussi O. Virtanen, Jenna Pietilainen-Nicklen, Lasse Uotila, Markus Farkkila, Antti Vaheri, Marjaleena Koskiniemi. Intrathecal human herpesvirus 6 antibodi
Home Page > Newsroom > News Releases > PECO > News Release News Releases October 14, 2004 - UC GREEN, PECO & OTHERS TEAM UP TO PLANT 50 TREES IN UNIVERSITY CITY WHAT: Hundreds of volunteers and representatives from local corporations and agencies gather together to not only plant trees -- but also plant the Fact Sheet right tree in the right p
 American Heart JournalVolume 142, Number 4
McFarlane et al 619
American Heart JournalVolume 142, Number 4
McFarlane et al 619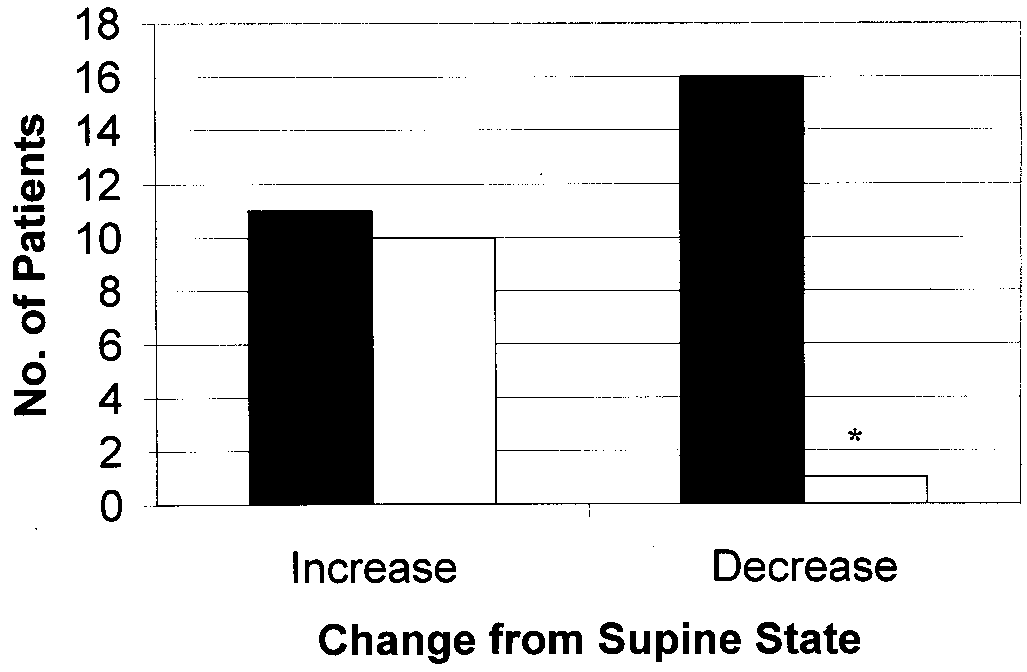
 620 McFarlane et al
620 McFarlane et al