Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Ios.ecache.cn
I n c i d e n c e , C o s t , a n d O u t c o m e s o f B l e e d i n g a n d C h e m o t h e r a p y D o s e M o d i fi c a t i o n A m o n g S o l i d T u m o r P a t i e n t s W i t h C h e m o t h e r a p y - I n d u c e d T h r o m b o c y t o p e n i a
By Linda S. Elting, Edward B. Rubenstein, Charles G. Martin, Danna Kurtin, Saul Rodriguez, Esa Laiho,
Krishnakumari Kanesan, Scott B. Cantor, and Robert S. Benjamin
Purpose: To describe the incidence and outcomes of apy delays occurred during 6% of cycles among pa- bleeding and chemotherapy dose modifications associ- tients with more than five previous cycles (P ؍ .003), ated with chemotherapy-induced thrombocytopenia radiotherapy (P ؍ .03), and disseminated disease (P ؍ (platelets < 50,000/L). .04). They experienced similar clinical outcomes but Patients and Methods: Six hundred nine patients used significantly more resources. Dose reductions oc- with solid tumors or lymphoma were followed-up dur- curred during 15% of cycles but were not associated ing 1,262 chemotherapy cycles complicated by throm- with poor clinical outcomes or excess resource utiliza- bocytopenia for development of bleeding, delay or tion. Significantly shorter survival and higher resource dose reduction of the subsequent cycle, survival, and utilization were observed among the 20% of patients resource utilization. The association between survival who failed to achieve an adequate response to platelet and bleeding or dose modification was examined using transfusion. the Cox proportional hazards model. Predisposing fac- Conclusion: The incidence of bleeding is low among tors were identified by logistic regression. solid tumor patients overall but exceeds 20% in some Results: Bleeding occurred during 9% of cycles subgroups. These subgroups are easily identifiable us- among patients with previous bleeding episodes (P < ing routinely available clinical information. A clinical .0001), baseline platelets less than 75,000/L (P < prediction rule is being developed. Poor response to .0001), bone marrow metastases (P ؍ .001), poor per- platelet transfusion is a clinically and financially signif- formance status (P ؍ .03), and cisplatin, carboplatin, icant downstream effect of thrombocytopenia and war- carmustine or lomustine administration (P ؍ .0002). rants further investigation. Major bleeding episodes resulted in shorter survival J Clin Oncol 19:1137-1146. 2001 by American and higher resource utilization (P < .0001). Chemother- Society of Clinical Oncology.
SINCE THE relationship between hemorrhage and the effective,15-17theyarenotwithoutsideeffectsandtheircost
depth of thrombocytopenia was first described among
will likely exceed the cost of platelet transfusions. It is
patients with acute leukemia in 1960,1 its importance to
unclear whether the potential cost of these agents is justified
patients with solid tumors has been debated. Although this
by the risk of serious clinical outcomes of profound or
relationship was confirmed by Belt et al in 19782 and later
prolonged thrombocytopenia among solid tumor patients.
by Dutcher et al,3 it was clear that hemorrhage was far less
There are insufficient data from patients who have re-
likely among patients with solid tumors than among their
ceived modern chemotherapy regimens to address these
counterparts with acute leukemia. It was suggested that this
issues; the last comprehensive study of thrombocytopenia
decreased risk of hemorrhage did not justify the costs or
among patients with lymphoma or solid tumors was pub-
risks of platelet transfusion at a threshold of 20,000 plate-
lished in 1984.3 For that reason, we studied episodes of
lets/L among patients with solid tumors.4-9 Nevertheless,
practice evolved toward use of a threshold of 20,000
those that resulted in major or minor bleeding, a delay of
platelets/L below which prophylactic transfusions wereadministered.10,11
Two recent developments have added new fuel to this
From the Department of Health Services Research, The University of
longstanding debate. First, three trials have provided evi-
Texas M.D. Anderson Cancer Center, Houston, TX.
dence that the 20,000-platelet threshold may be overly
Supported in part by a grant from Genetics Institute, Inc, Cam-
conservative for patients with leukemia.12-14 Given the
Presented in part at the Thirty-Third Annual Meeting of the
lower rate of bleeding observed among patients with solid
American Society of Clinical Oncology, May 17-20, 1997, Denver, CO.
tumors, re-examination of the potential benefits of prophy-
Address reprint requests to Linda S. Elting, DrPH, Department of
laxis is justified. Furthermore, platelet growth factors are
Health Services Research, The University of Texas M.D. AndersonCancer Center, 1515 Holcombe Blvd, Box 40, Houston, TX 77030;
currently being tested in clinical and preclinical trials. One
of these, interleukin-11, is commercially available. Studies
2001 by American Society of Clinical Oncology.
to date suggest that although these agents may be quite
Journal of Clinical Oncology, Vol 19, No 4 (February 15), 2001: pp 1137-1146
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
more than 7 days in the subsequent cycle of chemotherapy,
Table 1. Characteristics of Underlying Neoplasms and Common
or a reduction in the dose of the subsequent cycle. We
Chemotherapy Regimens
focused on three related questions: How frequently are
bleeding episodes or chemotherapy dose modification asso-
ciated with thrombocytopenia among patients with solid
tumors? Are the outcomes of these events sufficiently
serious and/or costly to justify prophylaxis? If so, which
patients are at sufficiently high risk to justify the use of
prophylactic platelet transfusions or growth factors?
A retrospective cohort consisting of a random sample of 609 patients
with solid tumors or lymphoma, stratified by underlying neoplasm, was
selected from among all patients who developed chemotherapy-in-
duced thrombocytopenia between January 1, 1994, and December 31,
1995. This cohort was followed-up through December 31, 1996, for
development of clinically significant thrombocytopenia and through
December 31, 1997, for survival. For each eligible patient, all cycles of
chemotherapy that occurred during the study period were included,
provided that thrombocytopenia developed. To insure complete ascer-
tainment of events, only patients whose entire care was provided by our
institution were included. Patients with leukemia and bone marrow
transplant recipients were excluded, as were those who received
After these exclusions, 1,262 cycles with thrombocytopenia were
studied in the 609 patients. Fifty-two percent of patients were female,
and the median age was 52 years (range, 17 to 87 years). They had
received a median of five cycles of chemotherapy in the past (range, 0
to 19 cycles); 92 patients (15%) were chemotherapy-naive. One half
(51%) had disseminated disease, whereas 81 (13%) were receiving
adjuvant or neoadjuvant chemotherapy in the absence of clinically
Patients with lymphoma, sarcoma, breast, and genitourinary cancers
contributed the largest number of cycles to the study (Table 1).
Chemotherapy regimens commonly used for these malignancies (flu-
orouracil, doxorubicin, and cyclophosphamide; cyclophosphamide,
vincristine, doxorubicin, and decadron; doxorubicin or etoposide plus
cisplatin, cytarabine, and prednisone; cisplatin, cyclophosphamide, and
doxorubicin; cyclophosphamide, doxorubicin, vincristine, and pred-
nisone; and doxorubicin plus either ifosfamide or platinum) were
predictably frequent. Platinum-based regimens were used in 41% of
cycles. With the exception of patients with lymphoma (who received
either doxorubicin or etoposide plus methylprednisolone, high-dose
cytarabine, and cisplatin) and sarcoma (who received high doses of
ifosfamide and doxorubicin), standard doses of chemotherapy were
administered in the majority of cases. Overall, 16% of the cycles
involved adjuvant or neoadjuvant therapy. However, there were signifi-
Abbreviations: FAC, fluorouracil, doxorubicin, cyclophosphamide; CVD,cis-
cant differences in this rate, depending on the underlying malignancy. For
platin, vinblastine, dacarbazine; CVAD, cyclophosphamide, vincristine, doxo-
example, more than 60% of cycles administered to patients with breast
rubicin, decadron; ASHAP; doxorubicin, cisplatin, cytarabine, prednisone;
ESHAP, etoposide, cisplatin, cytarabine, prednisone; CISCA, cisplatin, cyclo-phosphamide, doxorubicin; MINT, mesna, ifosfamide, mitoxantrone, pacli-
taxel; MINE, mesna, ifosfamide, mitoxantrone, etoposide; MIME, mesna,
All paper and electronic medical records of eligible patients were
ifosfamide, methotrexate, etoposide; CHOP, cyclophosphamide, doxorubicin,
reviewed. These included the paper medical record, electronic data-
vincristine, prednisone; MAID, mesna, doxorubicin, ifosfamide, dacarbazine;
bases containing all hospital and clinic visits, tumor registry and
ACE, doxorubicin, cyclophosphamide, etoposide; PIE, cisplatin, ifosfamide,
survival data, diagnostic test results, blood products transfused, and
etoposide; CyVADic, cyclophosphamide, vincristine, doxorubicin, dacarba-
pharmaceutical agents prescribed, as well as electronic records of
zine; POMB, cisplatin, vincristine, mitomycin, bleomycin; PVC, procarbazine,
patients enrolled on clinical research protocols. Information about
vincristine, carmustine; FND, fludarabine, mitoxantrone, decadron.
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
bleeding obtained from these sources was supplemented by data from
experienced bleeding or dose modification. The Kaplan-Meier method
The Ambulatory Treatment Center and Emergency Center Database,
was used for this analysis. Factors associated with shorter survival were
which contains clinical and resource utilization data pertaining to all
examined using the Cox proportional hazards regression model. For
outpatient chemotherapy and transfusion episodes and all visits to the
this analysis, factors were entered in the stepwise regression model
using the maximum partial likelihood ratio method.
Information from paper sources was transcribed by physician ab-
The secondary goal of this study was to generate hypotheses about
stractors and information from databases was transferred electronically.
high-risk groups for future study. For this analysis, demographic and
A 10-item set of variables (unknown to the abstractors) was collected
clinical factors were tested first for association with bleeding, chemo-
both manually and electronically for estimation of the frequency of
therapy delay, and dose reduction in separate univariate analyses
errors with manual transcription (Ͻ 3%). Additionally, a predetermined
(because they are not mutually exclusive events). Two-tailed 2 tests
set of key data items was validated by a separate reviewer in all cases
were used to test the significance of discrete variables and two-tailed t
to ensure 100% accuracy of critical items.
tests, continuous variables. Factors shown to be significant predictors inunivariate analysis (P Ͻ .10) were included in logistic regression
analyses. For this analysis, only those factors that are routinelyavailable on day 1 of the chemotherapy cycle in all solid tumor patients
Thrombocytopenia was defined as platelets less than 50,000/L.
were used, because the decision to administer prophylactic platelet
Bleeding was characterized as either minor (World Health Organiza-
growth factors is made at this time. Separate regression analyses were
tion grades 1 or 2, including petechiae, ecchymoses, superficial
conducted for bleeding, chemotherapy delay, and dose reduction.
bleeding of gums, microscopic hematuria, blood-tinged sputum, mild
Continuous variables were categorized or dichotomized for the regres-
epistaxis, and vaginal bleeding not requiring RBC transfusion) or major
sion analyses. The goodness of fit of the models was estimated using
(World Health Organization grades 3 or 4, including fatal hemorrhage
the Hosmer-Lemeshow statistic. Statistical analyses were computed
or epistaxis, vaginal bleeding, or major organ hemorrhage requiring
using BMDP Dynamic (Version 7, BMDP Statistical Software, Inc.,
RBC transfusion). Chemotherapy delay was defined as more than 7
days’ delay in the next planned cycle of chemotherapy. Dose reductionwas defined as a decrease of 20% or more or discontinuation of the
planned dose of any antineoplastic agent during the next cycle. Theseevents are not mutually exclusive; cycles with bleeding were occasion-
How Frequent Are Episodes of Bleeding and
ally accompanied by chemotherapy delay or dose reduction.
The extent of disease dissemination for each cycle was recorded and
dichotomized for regression analysis as either limited (no evidence of
Bleeding occurred during 111 cycles (9%) (Table 2).
disease or local disease) or disseminated (one or more site of metas-
Most episodes of bleeding were minor, including mild
tasis). The duration of thrombocytopenia was computed using the lastvalue carried forward method, as is typical in observational studies and
epistaxis during 31 cycles, petechiae and ecchymoses dur-
clinical trials. Resource utilization was described only during throm-
ing 19 cycles, and occasional cases of bleeding gums, mild
bocytopenia for each cycle. Resources used when platelet counts
vaginal bleeding, bloody urine, or sputum. All episodes of
exceeded 50,000/L were not considered.
minor bleeding resolved. Major hemorrhage occurred dur-
Performance status was measured on day 1 of each cycle using the
ing 43 cycles (3%). The most common sites were nasal (13
Zubrod score.18 Poor performance status was defined as Zubrod scoreless than 2. The presence of comorbidities was measured on day 1 of
cycles), gastrointestinal hemorrhage, (eight cycles), bladder
each cycle of chemotherapy using the Charlson score.19
hemorrhage, (five cycles), and vaginal or pulmonary hem-orrhage (four each). Bleeding was significantly more com-
mon during cycles complicated by febrile neutropenia (11%
The primary goals of this study were to estimate the incidence per
v 7%; P ϭ .02). The relationship between major hemorrhage
chemotherapy cycle, outcomes, and resource utilization associated with
and febrile neutropenia was particularly striking; major hem-
bleeding and chemotherapy dose modification and to describe changes
orrhage occurred during 5% of cycles complicated by febrile
in these parameters longitudinally over several cycles. Because of the
neutropenia but only 2% of those without febrile neutropenia
impact of the presence of febrile neutropenia on each of theseoutcomes, an analysis stratified by this factor was conducted. The unit
(P ϭ .002). Multiple sites of hemorrhage were involved in six
of analysis for this study was a cycle of chemotherapy, except in the
episodes. Although CNS tumors or metastases were present
case of survival analysis, which was conducted with the patient as the
during 129 cycles and prior CNS radiation therapy in 77
unit of analysis. Between two and 16 cycles were included in 288 of the
cycles, only one CNS hemorrhage occurred in a patient who
609 patients. Multiple cycles from a single patient were included to
provide accurate estimates of the magnitude of these problems amongcancer patients who are at risk of developing the events and use
A delay of more than 7 days in the next cycle of
resources during each of their multiple cycles of chemotherapy.
chemotherapy occurred during 99 cycles (8%). Most delays
Incidence is reported as the percentage of cycles with the event; 95%
(67%) were between 8 and 14 days; however, a delay of
confidence limits are also reported.
more than 30 days occurred during 15 cycles. A reduction in
Duration of survival after bleeding or chemotherapy dose modifica-
the dose of the subsequent cycle of chemotherapy was far
tion was the primary outcome of interest. The median time to survivalwas computed from the first day of one randomly chosen cycle for each
more common (17%). A delay or dose reduction for the
patient in order to provide a sufficient sample of patients who had
subsequent cycle followed 22% of the 111 cycles with
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
Table 2. Incidence of Bleeding and Chemotherapy Dose Modifications
Abbreviation: CI, confidence interval. *P ϭ .02. †P ϭ .002. ‡P ϭ .0005.
episodes of bleeding. Decisions to delay or reduce the dose
of 26 months (Table 3). The Cox proportional hazards
during a subsequent cycle were multifactorial. Approxi-
regression analysis illustrates this phenomenon. The pres-
mately 30% of delays or dose reductions resulted from
ence of disseminated disease (odds ratio [OR], 3.5; P Ͻ
infection and prolonged or profound granulocytopenia,
.0001), poor performance status (OR, 2.1; P Ͻ .0001), and
despite the presence of thrombocytopenia. However, in the
age Ն 65 years (OR, 1.8; P ϭ .0008) were associated with
remainder, thrombocytopenia contributed to the decision to
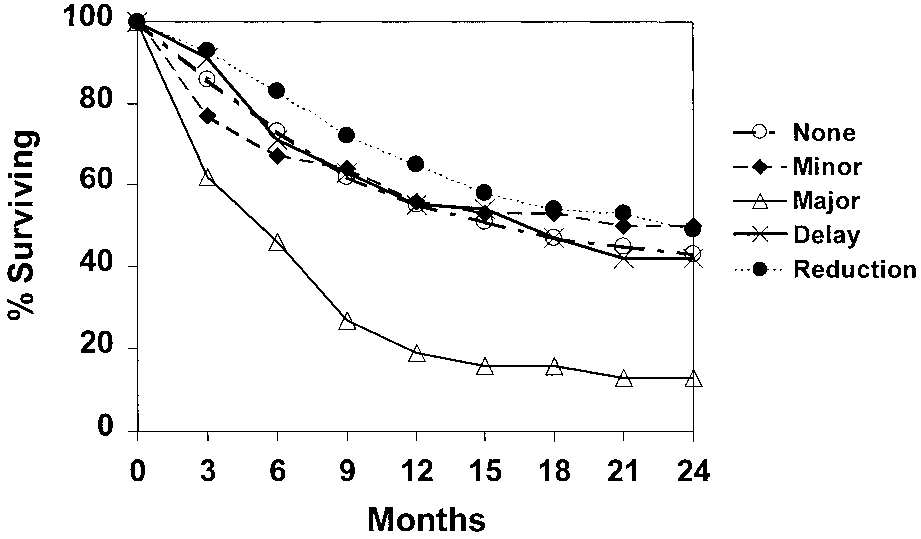
far shorter durations of survival. Minor bleeding episodes
delay or reduce subsequent doses, and in approximately
and chemotherapy dose delays and reductions did not
30%, prolonged or profound thrombocytopenia was the sole
contribute to shorter survival; only a major bleeding episode
was significantly associated (OR, 1.9; P ϭ .02) with shortersurvival (Fig 1). Although the presence of febrile neutropenia
How Serious Are the Outcomes of Bleeding Episodes and
did not contribute to shorter median survival times, mortality at
30 days was significantly more common during cycles com-
Episodes of thrombocytopenia complicated by bleeding
plicated by febrile neutropenia (6% v 2%; P Ͻ .0001).
were significant in both human and resource utilization
Episodes of bleeding were significantly associated with a
terms. In four patients, death was attributed at least in part
decrement or no increment in platelet count after transfusion
to hemorrhage (one adrenal hemorrhage, one gastrointesti-
compared with cycles with dose modifications or no events
nal, one bladder, and one massive hemorrhage at multiple
(47% v 17%; P Ͻ .0001). However, the overall rate of poor
sites). Overall, patients survived a median of only 5.9
response to platelet transfusion was surprisingly high during
months after cycles complicated by major bleeding episodes
all cycles (19%) and for both random-donor platelets (23%)
compared with more than 15 months after cycles without an
and single-donor platelets (15%). Poor response to platelet
episode of major bleeding (P Ͻ .0001) (Table 3). Twenty-
transfusion was observed most commonly during chemo-
one percent of the patients with major bleeding episodes
therapy cycles in males (56%); patients with lymphoma
died within 30 days of the cycle onset, compared with only
(45%), genitourinary malignancies (15%), or sarcoma
4% of the remaining patients (P Ͻ .0001).
(14%); those who had undergone more than 10 cycles of
When the extent of the underlying malignancy and other
chemotherapy in the past; and those with widely dissemi-
prognostic factors are considered, striking differences
nated disease (69%). Bleeding was associated with a failure
emerge. For example, the difference in survival after major
to achieve adequate response to platelet transfusion in 37%
bleeding episodes was limited to patients with disseminated
of cycles compared with only 12% of cycles during which
underlying disease. The few patients with limited disease
an adequate response was achieved (P Ͻ .0001). Although
who developed major bleeding episodes survived a median
this may be due partially to consumption of platelets at
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
Table 3. Outcomes of Thrombocytopenia
*The number of patients at each increment level divided by the number of patients who received platelet transfusions.
bleeding sites, episodes of bleeding during previous cycles
death of the patient (including the four patients whose
were also associated with poor increments (14% v 6%; P ϭ
deaths were attributed to hemorrhage) compared with only
.004). Nineteen percent of cycles during which a poor
3% of patients who responded to platelet transfusion (P Ͻ
response to platelet transfusion was observed ended in the
.0001). Forty-one percent of these patients also receivedsingle-donor platelets during that cycle and, among these,23% experienced a decrement in platelet count after single-donor platelets. It is notable that during this time period,platelet transfusions were filtered by the blood bank forpatients with hematologic malignancies and for bone mar-row transplant recipients only. Therefore, only the lym-phoma patients in this study received platelet transfusionsfiltered in the blood bank. All platelet transfusions wereadministered through filters. What Resources Are Used During Cycles Complicated byBleeding and Dose Modifications?
Not surprisingly, hospitalization during thrombocytope-
Fig 1. Kaplan Meier analysis illustrating the survival disadvantage of
nia was required more frequently (70%) during major
episodes of major bleeding. Patients receiving adjuvant or neoadjuvant therapy have been removed from the analysis.
bleeding episodes than those without (43%) (P ϭ .001) and
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
Table 4. Resource Utilization During Thrombocytopenia
Platelet units (mean units/per cycle), all
Abbreviations: ER, emergency room; SD, single donor platelet.
for an average of 2 more days (P ϭ .007) (Tables 3 and 4).
Considering the severity of outcomes and excessive
Hospitalization was significantly more common during
resource utilization, episodes of bleeding were considered
cycles complicated by febrile neutropenia (78% v 11%; P Ͻ
of sufficient import for further study. Although not associ-
.0001) and was required in 91% of cycles complicated by
ated with poor outcomes, chemotherapy delays were asso-
both major bleeding and febrile neutropenia. Clinic visits
ciated with sufficient increases in resource utilization to
and emergency center visits were also more frequent during
justify further study. However, the outcomes and resource
cycles with clinically significant thrombocytopenia. Plate-
utilization associated with dose reductions were virtually
lets were transfused during 80% of cycles with bleeding but
indistinguishable from those observed during cycles with no
only 41% of those without bleeding (P Ͻ .0001). Signifi-
event. Therefore, we studied predisposing factors for bleed-
cantly more units of platelets were transfused during bleed-
ing episodes and chemotherapy delays.
ing cycles than those without bleeding (17 units v 5 units;P Ͻ .0001) and single-donor platelets were also required
What Factors Predispose to Episodes of Bleeding and
more frequently (P ϭ .0001) (Table 4). The increased risk
of bleeding during cycles complicated by febrile neutrope-
Bleeding was associated with poor performance status
nia was accompanied by a corresponding increase in the use
(P ϭ .007) and multiple comorbidities (P ϭ .006) (Table 5).
of platelet transfusions (55% v 34%; P Ͻ .0001). Addition-
The association between performance status and episodes of
ally, more units of platelets were transfused during febrile
bleeding was particularly pronounced when the perfor-
neutropenia, even when bleeding did not occur.
mance status was declining, regardless of the actual perfor-
Failure to achieve an adequate response after platelet
mance status level observed. The incidence of bleeding was
transfusion may be a financially significant event. Overall,
unrelated to sex, ethnicity, or age.
patients who experienced a decrement in platelets received
The risk of bleeding was also unrelated to the specific
an average of 31 units of platelets for that cycle. Patients
underlying malignancy (Table 6). However, it was associ-
who experienced no increment received 18 units, those with
ated with disseminated disease (P ϭ .0001), bone marrow
an increment of 1,000 platelets per unit, 17 units, and those
metastases (P Ͻ .0001), prior episodes of bleeding (P Ͻ
who achieved an increment more than 1,000 platelets per
.0001), or a baseline platelet count less than 75,000/L
unit received only 8 units for that cycle (P Ͻ .0001).
(P Ͻ .0001). Delays of the subsequent cycles were uncom-
Patients who failed to achieve an adequate response to
mon during adjuvant chemotherapy (P ϭ .0001) but were
platelet transfusion were hospitalized an average of 8 days
significantly more common when the baseline platelet count
during thrombocytopenia compared with only 4 days for
was less than 50,000/L (P Ͻ .0001). The presence of
patients who responded to platelet transfusion (P Ͻ .0001).
necrotic tumor did not predispose to bleeding. Delays were
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
Table 5. Risk of Bleeding and Chemotherapy Dose Modification Related Table 6. Risk of Bleeding and Chemotherapy Dose Modification Related to Patients’ Characteristics to Disease Characteristics
more common when necrotic tumor was present, although
this difference did not reach statistical significance (P ϭ
.17). During cycles in which febrile neutropenia accompa-
nied thrombocytopenia, major bleeding episodes were sig-
nificantly more common (P ϭ .0008).
Numerous previous cycles of chemotherapy did not
predispose to bleeding whereas chemotherapy delays were
associated with more than five previous cycles (P ϭ .0008)
(Table 7). Previous radiation therapy did not predispose to
bleeding but was associated with a high risk of delay in a
subsequent cycle of chemotherapy (41% v 22%, P ϭ .001).
Concurrent radiation therapy was not associated with an
increased risk of bleeding or chemotherapy delay. Regi-
mens containing mitomycin, carmustine, or lomustine pre-disposed to bleeding, although these agents were used onlyoccasionally. Cisplatin- or carboplatin-based regimens were
contribution of each of these factors to the risk of clinically
also associated with higher rates of bleeding. Minor bleed-
significant thrombocytopenia. Based on the differing risk
ing episodes and chemotherapy delays were more common
profiles suggested by the univariate analysis, separate re-
during cycles in which prophylactic platelet transfusions
gression models were developed for bleeding and chemo-
were administered (P ϭ .01 and .07, respectively). Bleeding
therapy delay. The single most significant predictor of
and delays were significantly associated with both the depth
bleeding was a prior history of bleeding (P Ͻ .0001) (Table
and duration of thrombocytopenia. Bleeding was particu-
8). Measures of poor bone marrow function, such as a
larly common during cycles in which the platelet count fell
baseline platelet count less than 75,000 and the presence of
below 10,000/L (7% v 21%; P Ͻ .0001). In fact, the rate
bone marrow metastases, were also significant predictors of
of bleeding doubled (from 5% to 10%) when the platelet
bleeding (P ϭ .0001 and .005, respectively), as was a poor
count fell below 20,000/L and doubled again (from 10% to
performance status (P ϭ .05). Other factors shown to be
21%) when the count fell below 10,000/L (Fig 2).
predictive in univariate analysis (such as disseminated
Because of the correlation among many of the predictive
neoplastic disease and specific chemotherapeutic agents)
factors, logistic regression was used to identify the unique
did not prove to be significant predictors in the multiple-
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
Table 7. Risk of Bleeding and Chemotherapy Dose Modification Related to Treatment Characteristics Fig 2. Relationship between the nadir of platelet counts and the risk of bleeding demonstrating excess rates below 10,000 platelets/L.
variable model. A delay in the subsequent cycle of chemo-
therapy was predicted by the presence of disseminated
neoplastic disease (P ϭ .04) and measures of previous
insults to the bone marrow such as prior radiation therapy
(P ϭ .03) and numerous previous cycles of chemotherapy
Major hemorrhage during chemotherapy-induced throm-
bocytopenia is a serious clinical problem. This is particu-
larly true of CNS or major organ hemorrhage. Numerous
units of platelets are administered to patients with cancer
each year with the goal of preventing such events. However,
the actual risk of these events, particularly among patients
with solid tumors, has been disputed. Similar disputes
surround the importance of chemotherapy delays and dose
reductions. We examined the incidence and outcomes of
these events to inform decisions to use prophylactic platelet
transfusions and growth factors in these patients.
The primary impetus for this study was the lack of data
on the incidence of bleeding among thrombocytopenic
patients with solid tumors who have received modern
chemotherapy regimens. However, despite major changes in
chemotherapy regimens, our findings were remarkably sim-
ilar to those described in the past. We observed bleeding in
9% of patients with thrombocytopenia, Belt et al2 reported
bleeding in 10% of similar patients in 1978, and Dutcher et
al3 reported bleeding among 15% in 1984. We observed
only a single episode of CNS hemorrhage, despite a
significant proportion of patients (Ͼ 10%) at high risk. The
NOTE. Multiple high risk indicates more than one of the following: cisplatin,
consistency of these findings supports the notion that solid
carboplatin, lomustine, carmustine, paclitaxel, procarbazine.
tumor patients with similar depth and duration of thrombo-
Abbreviations: XRT, radiation therapy; ANC, absolute neutrophil count.
cytopenia share a common risk of bleeding, regardless ofthe specific chemotherapy regimen that is administered.
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
Table 8. Multiple Variable Models of Risk of Bleeding and Chemotherapy Dose Modification
NOTE. Hosmer-Lemeshow Goodness of Fit Test: bleeding model, P ϭ .70; delay model, P ϭ .98. For this statistic, high P values (approaching 1.0) indicate a
good fit to the data whereas lower P values (approaching 0) indicate a poor fit to the data.
Abbreviation: CI, confidence interval.
Our data also suggest that in addition to a common risk of
chemotherapy delays were different, they were similar to
bleeding during thrombocytopenia, solid tumor patients
those predisposing to bleeding in that they were illustrative
share common predisposing factors that are host-specific
of poor bone marrow reserve (prior radiation therapy and
rather than neoplasm-specific. Most notable among these is
numerous previous cycles of chemotherapy) and poor per-
a history of bleeding. Also among these are factors sugges-
formance status (disseminated disease). Thus these patients
tive of poor bone marrow function, such as a low baseline
are also easily identifiable by using information available on
platelet count and bone marrow metastasis, as well as poor
day 1 of a cycle of chemotherapy. It may be desirable from
performance status. Although tested in univariate and mul-
a cost standpoint to identify these patients, and, therefore,
tiple variable analyses, the specific neoplasm was not useful
this may be a fruitful area of research.
in predicting an episode of bleeding.
In contrast to dose delays, dose reductions led to neither
Our results combined with previous data confirm that
poorer outcomes nor increased resource utilization. Although
among thrombocytopenic solid tumor patients, the risk of
the benefit of high doses has been demonstrated for some
bleeding is low, overall. However, when episodes of
malignancies (particularly leukemia, multiple myeloma, some
bleeding do occur, they are associated with poor clinical
lymphomas, and sarcomas), for many other solid tumors, little
outcomes and significantly increased resource utilization.
or no advantage has been demonstrated to high-dose regimens
We have demonstrated that there are easily identifiable
with substantial toxicity.20 In our Cox proportional hazards
subsets of this population in whom the risk of bleeding
model of survival, dose reduction did not prove to be signifi-
exceeds 20%. Given these findings, a single strategy (or
cantly associated with shorter durations of survival, despite an
threshold) for bleeding prophylaxis of all thrombocyto-
overrepresentation of patients with lymphoma and sarcoma in
penic solid tumor patients is unlikely to provide the most
whom this difference might have been expected to be impor-
cost-effective solution; an individualized approach is far
tant. If this benefit does indeed exist, it may be limited to a
more attractive. We are currently developing a clinical
subset of patients with solid tumors.
prediction rule based on this multiple-variable risk model
Finally, we have reported strikingly high rates of
to guide the use of prophylactic platelet transfusions and
inadequate response to both random-donor (23%) and
growth factors for individual patients in this population.
single-donor (15%) platelet transfusion for this popula-
Delays in chemotherapy were uncommon (6%). Com-
tion. Although this was not a primary objective of the
pared with cycles with no event, delays were associated
study, we report these results to stimulate hypotheses and
with higher resource utilization but not poorer clinical
future study, because this may be among the most
outcomes. Although the specific factors that predisposed to
clinically and financially significant effects of thrombo-
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
cytopenia. Numerous platelet transfusions (often of the
multifactorial, and it is possible that their poor responses
single-donor variety) were required for maintenance of
to transfusion resulted from consumption of platelets at
hemostasis by patients who failed to achieve an adequate
their extensive bleeding sites. Nevertheless, this associ-
response to transfusion. Considering the average cost of
ation—when considered together with the previously
platelet transfusions in the United States (Ͼ $500), this
mentioned observations—reinforces a concern that has
can be an extremely costly undertaking.21
been voiced by many clinicians. Excessive use of platelet
From both a clinical and a statistical standpoint, it is
transfusions for prophylaxis and treatment, early in the
difficult to determine whether poor increments led to
course of malignancy, may result in patients who are
bleeding or whether bleeding and its attendant, numerous
refractory to all platelet transfusions later in the course of
transfusions led to poor increments. Although tests of
their malignancy, when they are at highest risk of
statistical significance suggest that the association be-
bleeding. Our data underscore the importance of this
tween these factors is unlikely to have occurred by
concern. Prospective study of this significant downstream
chance, both may be due to a third factor (such as
effect of thrombocytopenia should be a high priority.
consumption of platelets at bleeding sites). Whatever the
We conclude that some, but not all, solid tumor patients are
causal relationship, the excess mortality among patients
at sufficiently high risk of serious clinical outcomes to justify
who failed to achieve adequate increments after transfu-
aggressive bleeding prophylaxis during chemotherapy-induced
sion (19% v 3%) is troubling. This finding is doubly
thrombocytopenia. Our ongoing research focuses on the de-
significant when viewed in the light of the observation
velopment of an easy-to-use clinical prediction rule to guide
that all four patients whose deaths were caused in part by
individualized prescription of prophylactic platelet transfusions
thrombocytopenia-induced hemorrhage experienced in-
and growth factors. We encourage further research on the
adequate increments after both random-donor and single-
downstream clinical and financial effects of failure to achieve
donor platelet transfusions. These patients’ deaths were
adequate platelet increments after platelet transfusion.
1. Gaydos LA, Freireich EJ, Mantel N: The quantitative relation
13. Rebulla P, Finazzi G, Marangoni F, et al: The threshold for
between platelet count and hemorrhage in patients with acute leukemia.
prophylactic platelet transfusions in adults with acute myeloid leuke-
2. Belt RJ, Leite C, Haas CD, et al: Incidence of hemorrhagic
14. Wandt H, Frank M, Ehninger G, et al: Safety and cost effec-
complications in patients with cancer. JAMA 239:2571-2574, 1978
tiveness of a 10 x 109/L trigger for prophylactic platelet transfusions
3. Dutcher JP, Schiffer CA, Aisner M, et al: Incidence of thrombo-
compared with 20 x 109/L trigger: A prospective comparative trial
cytopenia and serious hemorrhage among patients with solid tumors.
in 105 patients with acute myeloid leukemia. Blood 91:3601-3606,
4. Goldberg GL, Gibbon DG, Smith HO, et al: Clinical impact of
15. Tepler I, Elias L, Smith II JW, et al: A randomized placebo-
chemotherapy-induced thrombocytopenia in patients with gynecologic
controlled trial of recombinant human interleukin-11 in cancer patients
with severe thrombocytopenia due to chemotherapy. Blood 87:3607-
5. Fanning J, Hilgers RD, Murray KP, et al: Conservative manage-
ment of chemotherapy-induced thrombocytopenia in women with
16. Isaacs C, Robert NJ, Bailey FA, et al: Randomized placebo-
gynecologic cancers. Gynecol Oncol 59:191-193, 1995
controlled study of recombinant human interleukin-11 to prevent
6. Beutler E: An iconoclastic view of conventional wisdom in
chemotherapy-induced thrombocytopenia in patients with breast cancer
hematology. Arch Intern Med 139:221-223, 1979
receiving dose-intensive cyclophosphamide and doxorubicin. J Clin
7. Baer MR, Bloomfield CD: Controversies in transfusion medicine:
Prophylactic platelet transfusion therapy—Pro. Transfusion 32:377-
17. Basser R: Clinical use of thrombopoietic growth factors. ASCO
8. Schiffer CA: Prophylactic platelet transfusion. Transfusion 32:
18. Zubrod CG, Schneiderman M, Frei E, et al: Appraisal of
methods for the study of chemotherapy of cancer in man: Comparative
9. Beutler E: Platelet transfusions: The 20,000/L trigger. Blood
trial of nitrogen mustard and trimethylene thiophosphoramide. J Chron
10. Pisciotto PT, Benson K, Hume AB, et al: Prophylactic versus
19. Charlson ME, Pompei P, Ales KL, et al: A new method of
therapeutic platelet transfusion practices in hematology and/or oncol-
classifying prognostic comorbidity in longitudinal studies: Develop-
ogy patients. Transfusion 35:498-502, 1995
ment and validation. J Chron Dis 40:373-383, 1987
11. Norfolk DR, Ancliffe PJ, Contreras M, et al: Concensus confer-
20. Savarese DM, Hsieh C, Stewart FM: Clinical impact of chemo-
ence on platelet transfusion: Royal College of Physicians of Edinburgh.
therapy dose escalation in patients with hematologic malignancies and
solid tumors. J Clin Oncol 15:2981-2995, 1997
12. Heckman K, Weiner G, Davis C, et al: Randomized study of
21. Cantor SB, Elting LS, Hudson DV, et al: Pharmacoeconomic
prophylactic platelet transfusion threshold during induction therapy for
analysis of rhIL-11 for secondary prophylaxis of thrombocytopenia in
adult acute leukemia: 10,000/ml versus 20,000/ml. J Clin Oncol
solid tumor patients receiving chemotherapy. Proc Am Soc Clin Oncol
Downloaded from jco.ascopubs.org on January 7, 2009 . For personal use only. No other uses without permission.
Copyright 2001 by the American Society of Clinical Oncology. All rights reserved.
PRAXIS FÜR KINDER- UND JUGENDPSYCHIATRIE, PSYCHOSOMATIK UND PSYCHOTHERAPIE Dr. med. Sigrun Wirth FA für Psychosomatik und Psychotherapie ADHS (Aufmerksamkeitsdefizit-Hyperaktivitätsstörung) bei Erwachsenen ie ADHS bei Kindern ist eine Störung, die Dinge konzentrieren, die sie interessieren, nicht D ittlerweile in der Bevölkerung weitläufig aber auf solche, die für sie un
 CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
Table 3. Outcomes of Thrombocytopenia
CHEMO-INDUCED THROMBOCYTOPENIA IN SOLID TUMORS
Table 3. Outcomes of Thrombocytopenia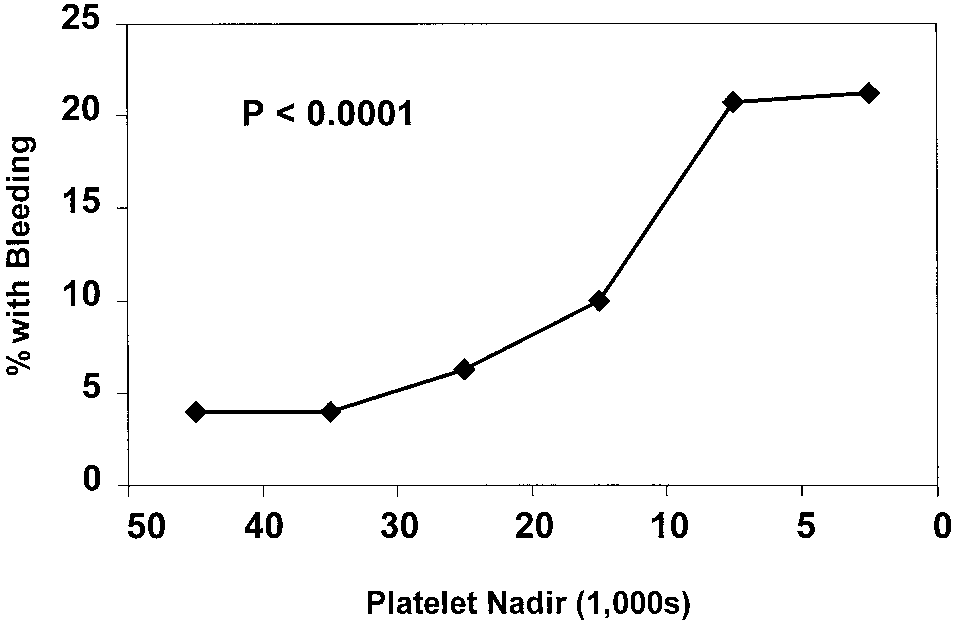 Table 7. Risk of Bleeding and Chemotherapy Dose Modification Related
Table 7. Risk of Bleeding and Chemotherapy Dose Modification Related