Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Asarhan.kau.edu.sa
Topiramate for the treatment of infants with early myoclonic encephalopathy Mohammed M. Jan, MBChB, FRCP(C), Saleh S. Baeesa, MBChB, FRCS(C), Zaitoon M. Shivji, RET, REMGT. Objectives:
Early myoclonic encephalopathy (EME) is a
were included. In addition to daily seizures, they all had
rare epileptic syndrome characterized by neonatal onset of
global hypotonia, developmental delay, and progressive
severe recurrent seizures of multiple types often resistant to
microcephaly. The syndrome was cryptogenic in 3, and one
antiepileptic drugs (AEDs). Topiramate (TPM) is a new AED,
which has a wide spectrum of antiepileptic activities
electroencephalograms showed generalized epileptic burst
suggesting a potentially valuable therapeutic profile. There is
suppression pattern. Infants were tried on multiple AEDs (6-
limited clinical data available on TPM use in infants and our
11, mean 7.5) with no success. Topiramate was added at age
aim is to report our experience with TPM for the treatment of
5-12 months (mean 9) reaching a maximum dose of 5.5-10
infants with intractable seizures secondary to EME.
mg/kg/day (mean 7.6). The infants were then followed for upto 19 months (mean 13.5). After introducing TPM, one infant
Methods:
Prospective, open label, add on trial of TPM in
became completely seizure free and 3 had significant (>50%)
treating a series of infants with EME at King Faisal Specialist
seizure reduction. Electroencephalograms in 3 infants showed
Hospital and Research Centre and King Abdul-Aziz
marked improvement. One infant had weight loss that
University Hospital, Jeddah, Kingdom of Saudi Arabia
resulted in discontinuing the drug after 6 months. Follow-up
between June 1999 and March 2002. Topiramate was started
renal ultrasound findings were normal in all infants.
at 12.5 mg/day and was increased by doubling the dose everyweek until the minimum effective dose was reached (seizure
Conclusions:
Topiramate is effective and safe in treating
free outcome) or up to a maximum of 10 mg/kg/day.
infants with intractable epilepsy secondary to EME.
Results:
Four consecutive infants (2 males and 2 females)
Neurosciences 2003; Vol. 8 (2): 110-112
arly myoclonic encephalopathy (EME) is a rare
multiple types (myoclonic, clonic, and tonic). The
epileptic syndrome that consists of 2 clinically
seizures are frequently resistant to antiepileptic drugs
similar syndromes closely related to infantile spasms.1
(AED). The electroencephalogram (EEG) shows
These include early infantile epileptic encephalopathy
striking epileptic burst suppression pattern that may
described by Ohtahara et al in 1987,2 and neonatal
later evolve to atypical or modified hypsarrhythmia.
myoclonic encephalopathy described by Aicardi in
Early myoclonic encephalopathy can be lesional (central
1990.3 Some authors suggested that the separation
nervous system (CNS) malformations, migration
between these syndromes might be artificial.4 In this
disorders), metabolic (mitochondrial, amino acid, and
paper, we will use the term early myoclonic
encephalopathy to be inclusive of both clinical entities.5
hyperglycinemia), or cryptogenic. Regardless of the
Early myoclonic encephalopathy is characterized by
etiology, infants with EME carry poor prognosis for
neonatal presentation of severe recurrent seizures of
complete seizure control and neuro-developmental
From the Department of Neurosciences, King Faisal Specialist Hospital and Research Centre, Jeddah, Kingdom of Saudi Arabia.
Received 8th July 2002. Accepted for publication in final form 2nd October 2002.
Address correspondence and reprint request to: Dr. Mohammed M. S. Jan, Department of Neurosciences, King Faisal Specialist Hospital and Research Centre,MBC J-76, PO Box 40047, Jeddah 21499, Kingdom of Saudi Arabia. Tel. +966 (2) 6677777 Ext. 5819. Fax. +966 (2) 6677777 Ext. 5813. E-mail:mmsjan@yahoo.com
TPM for early myoclonic encephalopathy . Jan et al
outcome.1-3,5 Topiramate (TPM) is a new AED, whichappears to have multiple modes of action includingsodium channel blockade, gamma-aminobutyric acidenhancement, glutamate antagonism, and weak carbonicanhydrase inhibition.6-8 This wide spectrum ofantiepileptic actions suggests a valuable and broadtherapeutic profile. There is limited clinical dataavailable on TPM use in infants and young children.9-17However, the current clinical experience is encouraging. Clinical trials have shown that TPM is effective whenused adjunctively in children with refractory partial andsecondary generalized seizures.12 It was also found to beuseful as adjunctive therapy in the management ofLennox-Gastaut syndrome, severe myoclonic epilepsy ofinfancy, and West syndrome.12-14 In this paper, we reportour experience with TPM for the treatment of infants
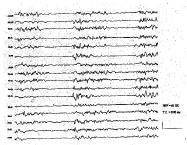
Figure 1 - Electroencephalogram (coronal montage) of a 7-month-old
infant diagnosed with early myoclonic encephalopathy before
with intractable seizures secondary to EME.
introducing topiramate. The features are consistent withgeneralized epileptic burst suppression pattern.
Methods. A series of consecutive infants diagnosedwith EME was identified prospectively. Patients were
explain their state. In addition these infants had global
identified through referrals and consultations to the
hypotonia, developmental delay, and progressive
pediatric neurology service at King Faisal Specialist
microcephaly. Brain computed tomography (CT) and
Hospital and Research Centre (KFSH&RC) and King
magnetic resonance imaging (MRI) were performed in
Abdul-Aziz University Hospital, both in Jeddah,
all cases and revealed mild nonspecific atrophy in 2. No
Kingdom of Saudi Arabia, between June 1999 and March
malformations or developmental abnormalities were
2002. King Abdul-Aziz University Hospital is the main
detected. Detailed metabolic workup was unrevealing
teaching center of the western region in collaboration
except in one girl who had nonketotic hyperglycinemia.
with KFSH&RC. Both are multispecialty adult and
The syndrome was therefore cryptogenic in the other 3
pediatric hospitals providing tertiary medical care for
infants. Initial EEGs showed generalized epileptic burst
most of the regional population of western KSA. Patient
suppression pattern (Figure 1). The infants were tried on
and disease related data was collected during the initial
multiple AEDs (6-11, mean 7.5) with no success,
visit. The diagnosis of EME was based on the clinical
including the newer AEDs, B6, steroids, and intravenous
features and EEG findings. The seizures were of
immunoglobulins. Before introducing TPM, the infants
neonatal onset, mixed, and intractable (defined as
were receiving 2-3 AEDs. Topiramate was added to the
recurrent seizures that failed to respond to at least 3
other AEDs at age 5-12 months (mean 9). The final
antiepileptic medication trials singly or in combination
Topiramate dose ranged between 50-100 mg/day (mean
despite using maximum doses or doses resulting in
65) divided twice per day, corresponding to 5.5-10 mg/
therapeutic drug levels). After consenting to drug use,
kg/day (mean 7.6). The infants were then followed for
infants were started on TPM in an open label, add on
up to 19 months (mean 13.5). After the introduction of
trial. Topiramate was added to the other antiepileptic
TPM, one infant became completely seizure free and 3
drug therapy at a starting dose of 12.5 mg/day and was
had significant (>50%) seizure reduction. All infants
gradually increased by doubling the dose every week
continued to receive other AEDs (1-2 in addition to
until the minimum effective dose was reached (achieving
TPM). The EEGs in 3 infants revealed marked
a seizure free outcome) or up to a maximum dose of 10
improvement in terms of epileptiform discharges, but
mg/kg/day. Follow-up by one pediatric neurologist was
continued to show background abnormalities. The EEG
performed to document therapeutic response and
features evolved to that of Lennox-Gastaut syndrome in
occurrence of side effects. Therapeutic response was
one boy who was followed to the age of 27 months. No
recorded as complete (no seizures), good (>50% seizure
side effects or drug interactions were noted in 3 infants.
reduction), fair (<50% seizure reduction), or none (no
One infant had initial weight loss and subsequent poor
weight gain that resulted in discontinuing the drug after6 months. Follow-up renal ultrasound was normal in all
Results. Four consecutive infants (2 males and 2
females) were included. All infants had many dailyseizures that started early in the neonatal period (mean
Discussion. The study results suggest that TPM is
age of 3 days). The seizures were of multiple types
an effective and well-tolerated AED when used in
(myoclonic, clonic, and tonic), however, myoclonic
infants with EME. Three of our infants had significant
seizures were the most common. There were no
seizure reduction and one became completely seizure
prenatal, natal, or postnatal complications that would
free. This is very impressive, as all of them had very
Neurosciences 2003; Vol. 8 (2) 111
TPM for early myoclonic encephalopathy . Jan et al
difficult seizures, which were resistant to multiple
AEDs. Most EEGs also showed marked improvement interms of epileptiform discharges. Other investigators
1. Aicardi J. Epilepsy and other seizure disorders. In: Diseases of
have successfully used TPM in infants primarily with
the nervous system in childhood. 2nd ed. London (UK): Mac
myoclonic epilepsy;13,14,16 however, there are no reports
of using it in EME. Our maximum dose did not exceed
2. Ohtahara S, Ohtsuka Y, Yamatogi Y, Oka E. The early infantile
epileptic encephalopathy with suppression bursts: developmental
10 mg/kg/day which was based on other reported
aspects. Brain Dev 1987; 9: 371-376.
experience and the drug company’s recommendations.
3. Aicardi J. Neonatal myoclonic encephalopathy and early
Preliminary data on the pharmacokinetics of TPM in
infantile epileptic encephalopathy. In: Neonatal seizures. New
infants appears to be linear with higher plasma clearance
York (NY): Raven Press; 1990. p. 41-49.
than that reported for older children, and therefore
4. Lombroso CT. Early myoclonic encephalopathy, early infantile
substantially higher than that reported for adults.15 This
epileptic encephalopathy and benign and severe infantile
means that infants may require significantly larger doses
contributions. J Clin Neurophysiol 1990; 7: 380-408.
per kilogram than older children and adults. These
5. Volpe JJ. Neonatal seizures. In: Neurology of the newborn. 4th
authors recommended titration to effect and not absolute
ed. Philadelphia (PA): WB Saunders Company; 2001. p.
TPM dose should guide therapy in this age group.15 It is
possible that higher doses (>10 mg/kg/day) may prove to
6. White HS, Brown D, Skeen GA, Woodbury DM. The
anticonvulsant topiramate displays a unique ability to potentiate
We did not encounter any significant side effects in 3
GABA evoked chloride currents. Epilepsia 1995; 36: S39.
infants, however, TPM had to be discontinued in one
7. White HS, Brown D, Skeen GA, Hamsworth WL, Sofia RD. The
investigational anticonvulsant topiramate potentiates GABA
infant because of weight loss. In one long term response
evoked currents in mouse cortical neurons. Epilepsia 1995; 36:
trial of TPM in infants with West syndrome, the drug
was well tolerated in that no patients discontinued
8. Severt L, Coulter DA, Sombati D, DeLoprenzo RJ. Topiramate
because of adverse events.14 This is also the experience
selectively blocks kainate currents in cultured hippocampal
of other investigators who used TPM in young infants.16
neurons. Epilepsia 1995; 36: S38.
Mild to moderate behavioral and cognitive side effects
9. Glauser TA. Preliminary observations on topiramate in pediatric
may be difficult to recognize in our young
epilepsies. Epilepsia 1997; 38: S37-S41.
10. Glauser TA. Topiramate use in pediatric patients. Can J Neurol
developmentally delayed patients. We used a slow rate
Sci 1998; 25: S8-S12.
of drug introduction and tended to use the minimum
11. Dooley JM, Camfield PR, Smith E, Lagevin P, Ronen G.
effective dose. Rapid dose titration has been implicated
Topiramate in intractable childhood onset epilepsy - a cautionary
in these side effects.13 Recently, Takeoka et al17 reported
note. Can J Neurol Sci 1999; 26: 271-273.
mild metabolic acidosis (decreased serum bicarbonate)
12. Ormrod D, McClellan K. Topiramate: a review of its use in
in children treated with TPM, presumably related to
childhood epilepsy. Paediatric Drugs 2001; 3: 293-319.
13. Nieto-Barrera M, Candau R, Nieto-Jimenez M, Correa A, del
carbonic anhydrase inhibition. We did not routinely
Portal LR. Topiramate in the treatment of severe myoclonic
screen for this abnormality in our patients. Caution is
epilepsy in infancy. Seizure 2000; 9: 590-594.
needed when TPM is used in infants with conditions that
14. Glauser TA, Clark PO, McGee K. Long term response to
may predispose to acidosis or poor weight gain.
topiramate in patients with west syndrome. Epilepsia 2000; 41:
Although long term safety and possible adverse
effects have not been fully established in infants, TPM
15. Glauser TA, Miles MV, Tang P, Clark P, McGee K, Doose DR.
may represent an option for infants with high seizure
Topiramate pharmacokinetics in infants. Epilepsia 1999; 40: 788-791.
frequency unresponsive to standard AED. We found it
16. Kugler SL, Sachdeo RC. Topiramate efficacy in infancy.
effective and safe in treating infants with intractable
Pediatr Neurol 1998; 19: 320-322.
epilepsy secondary to early myoclonic encephalopathy.
17. Takeoka M, Holmes GL, Thiele E, Bourgeois BF, Helmers SL,
Careful monitoring of the body weight is needed in these
Duffy FH, et al. Topiramate and metabolic acidosis in pediatric
epilepsy. Epilepsia 2001; 42: 387-392.
Acta Farm. Bonaerense 24 (4): 527-32 (2005) Recibido el 11 de junio de 2005Aceptado el 19 de julio de 2005Actividad Antiplasmódica In Vitro e Inhibición de la Formaciónde la β-Hematina de Plantas Colombianas de la Familia Annonaceae. Edison OSORIO 1, Gabriel ARANGO 1*, Edison GARCÍA 1, Katalina MUÑOZ 1, Grace RUIZ 2,David GUTIÉRREZ 2, Marco Antonio PACO 2 & Alberto GIMÉNEZ 2
EL PIPELINE DE PFIZER AVANZA EN ÁREAS TERAPÉUTICAS PRIORITARIAS • Los ensayos clínicos de Fase III para el primer inhibidor JAK para la artritis reumatoide y tanezumab para el dolor han empezado recientemente • La compañía alcanza su objetivo de comenzar la Fase III de 12 nuevos medicamentos en un año Madrid, 13 de abril, 2009 –Pfizer acaba de publ
 TPM for early myoclonic encephalopathy . Jan et al
outcome.1-3,5 Topiramate (TPM) is a new AED, whichappears to have multiple modes of action includingsodium channel blockade, gamma-aminobutyric acidenhancement, glutamate antagonism, and weak carbonicanhydrase inhibition.6-8 This wide spectrum ofantiepileptic actions suggests a valuable and broadtherapeutic profile. There is limited clinical dataavailable on TPM use in infants and young children.9-17However, the current clinical experience is encouraging.
TPM for early myoclonic encephalopathy . Jan et al
outcome.1-3,5 Topiramate (TPM) is a new AED, whichappears to have multiple modes of action includingsodium channel blockade, gamma-aminobutyric acidenhancement, glutamate antagonism, and weak carbonicanhydrase inhibition.6-8 This wide spectrum ofantiepileptic actions suggests a valuable and broadtherapeutic profile. There is limited clinical dataavailable on TPM use in infants and young children.9-17However, the current clinical experience is encouraging.