Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Pain management center
PAIN MANAGEMENT CENTER PATIENT HISTORY
NAME: _______________________________________________________________
Please fill in completely (0) all circles (yes and no) as pertaining to your current symptoms. Constitutional Musculoskeletal Ophthalmology Neurology Dermatology Endocrinology Cardiology Hematology/Lymph Respiratory Allergy/Immune system Gastroenterology Psychology Male reproductive Female reproductive
How long have you had your pain? O 0-6 months O 6-12 months
O 1-5 years O 5-10 years O longer than 10 years
In the last 2-3 weeks when does your pain occur?
On a scale of 0 to 10, with 10 being the worst pain, mark where the severity of your pain is. O 0
Associated numbness O Yes O No Associated Tingling O Yes O No What was the setting when the problem first occured?
O prolonged keyboard activity O repetitive grasping
O sports (without obvious trauma) O squatting
Please describe your pain (quality): O aching
O penetrating O pins and needles O pressure
Please indicate those activities that INCREASE your pain: (check all that apply) O work
O foods or beverages O locale (i.e. home/work/etc.)
O medications O menstrual cycle O physical activites
O recreational drug use O sleep-related factors
Please indicate those activities that DECREASE your pain: (check all that apply) O walking
O emergency room treatment O elevating the affected area
O non weight bearing O supporting the extremity O avoiding stress
O language difficulty O mental status change
How many ER visits have you had in the last 3 months for pain?
Do you take any of the following anticoagulants? (check all that apply)
Have you tried any of these therapies: O acupressure
O nerve stimulation O occupational therapy
Have you tried any of these pain clinic treatments: O injection therapy O medications O physical therapy
Have you tried the following NSAIDS to help relieve your pain: O ibuprofen O aleve
Are you on Workers Comp?
Mark the appropriate information related to Worker's Compensation:
O unable to work at all since the injury
O able to work with restrictions since the injury
O temporary limitations after the injury
Litigation pending: O Yes
If you are involved in any lawsuits, who is the lawsuit against? (Check all that apply) O Worker's Compensation O Auto accident
Have you been to any of the following types of doctors? O Back Surgeon
Past Medical History Heart disease
Thyroid/endocrine problem O Yes O No Family History Is your father still alive?
Do you have children or other dependents at home? O Yes O No Social History What is your marital status? Are you currently employed? Are you on Disability? What type of disability do you have? Do you use alcohol to control your pain? O Yes O No Mark if you use any of the following drugs recreationally: O Amphetamines Dependency or addiction to drugs now or in the past? (Check all that apply) O Amphetamines
O Marijuana O Morphine O Oxycodone O Soma
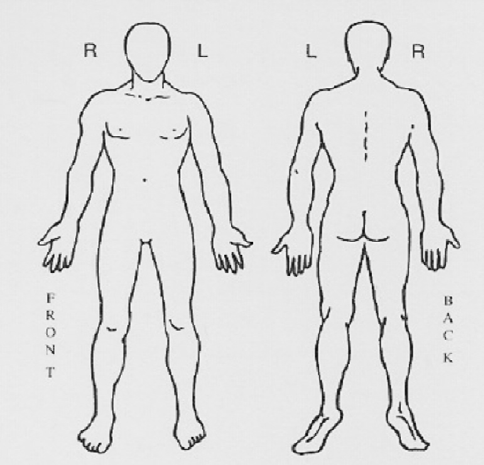
Please mark your pain area(s) on this diagram.
Ist Brain-Doping tatsächlich Doping? Zur medialen Definition pharmazeutischer leistungssteigernder Maßnahmen im Beruf und Alltag der Konzentration, Provigil® zur Erhöhung undVerlängerung der Wachsamkeit); Medikamente,»Forget sports doping. The next frontier iswelche die körperliche Leistungsfähigkeit erhö-brain doping.« So schreibt Karen Kaplan in ei-hen (z.B. Steroide). Viagr
“Not being able to go home after • Postpoliosyndrome , after polio-infection 1945, weakness left • Mammacarcinoma 1988: mamma-amputation and post-• Medication: carbaspirin calcium, metformin, simvastatin, • Mobility: did walk with rollator outdoors for longer distances • Personal care: independent; shopping with neighbor/children; • Relations/occupancy: divorced in 1988, two
 Please mark your pain area(s) on this diagram.
Please mark your pain area(s) on this diagram.