Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
69250all_new
INTRATHECAL BACLOFEN WITHDRAWAL SYNDROME FOLLOWING POSTERIOR SPINAL FUSION FOR NEUROMUSCULAR SCOLIOSIS: A CASE REPORT
Pedro Fernandes, M.D.1; Lori Dolan, Ph.D.2; Stuart L. Weinstein, M.D.2
ABSTRACT
paresthesia, hyperthermia, hypotension, hallucinations,
Because of the increased number of patients
delusions, confusion, psychosis and seizures.6 Auditory
with neuromuscular scoliosis receiving intrathe-
and visual hallucinations have also been reported in pa-
cal baclofen therapy, we report a clinical case of
tients with oral baclofen withdrawal.14,15 According to the
withdrawal. We hope to make physicians aware of
manufacturer, advanced IBWS may resemble autonomic
this potentially serious complication where signs
dysreflexia, sepsis, malignant hyperthermia, neuroleptic
and symptoms may be difficult to interpret due to
malignant syndrome, or other conditions associated with
population characteristics.
a hypermetabolic state or widespread rhabdomyolysis.16 These symptoms are seen mostly in spinal-cord injury
INTRODUCTION
patients where the diagnosis may be difficult to make
Intrathecal baclofen (ITB) is increasingly being used
due to possible confusion with autonomic dysreflexia.
for the treatment of spasticity in cerebral palsy patients.
In the pediatric population, we are aware of only one
The response rate has been reported as being up to 97
case (following posterior spinal fusion for scoliosis) where
percent with use of less than one percent of the systemic
baclofen was not delivered despite a normal-functioning
dose.1,2,3,4 Intrathecal baclofen withdrawal symptoms
pump. This report offered no details concerning the
(IBWS) are less frequently reported than withdrawal
type of surgery or possible cause for catheter malfunc-
from oral baclofen.5 Symptoms are difficult to interpret
tion.17 Because of the increased number of patients with
and in some cases can be life threatening.5,6,7,8,9,10,11,12
neuromuscular scoliosis receiving intrathecal baclofen
Symptoms develop when central nervous system levels
therapy, we report a clinical case of withdrawal to make
of baclofen decrease over a short period of time. This
physicians aware of this potentially serious complication
may be precipitated by pump malfunction or failure, cath-
where signs and symptoms may be difficult to interpret
eter obstruction or failure, or decline in pump reservoir
drug level. Of these possible problems, complications related to the catheter itself are by far the most frequent
CASE REPORT
and affect up to 40 percent of patients with ITB pumps.13
An 18-year-old female with spastic quadriplegia and
Patients usually return to a baseline level of spasticity,
scoliosis was treated with posterior spinal fusion and
frequently became agitated, and experience sleepless-
instrumentation necessitated by curve progression and
ness with IBWS. Other symptoms include pruritis,
increased difficulty sitting. She had low-normal intel-ligence, mild dysarthria and no psychiatric history. Her first baclofen pump had been inserted four years previ-
ously and was revised eight months prior to her spinal
fusion because of pump malfunction (Figure 1).
Av. Professor Egas Moniz 1649-028Lisbon, Portugal
A T2 to sacrum fusion was performed using Luque-
Galveston instrumentation. During this procedure, the
2University of Iowa Hospitals and Clinics
catheter entrance into the lumbar spine was carefully
Department of Orthopaedics and Rehabilitation
localized and dissected free in order to protect it dur-
ing the procedure. The surgery was uneventful with no
lori-dolan@uiowa.edu, stuart-weinstein@uiowa.edu
complications and blood loss was estimated at 400cc
The initial postoperative course was uncomplicated.
University of Iowa Hospitals and ClinicsDepartment of Orthopaedics and Rehabilitation
On postoperative day (POD) two the patient had an
abrupt onset of multiple symptoms of delirium, includ-
ing fluctuating levels of awareness and orientation, but
stuart-weinstein@uiowa.edu319-356-1872 Telephone
mainly hallucinations. She was dysarthric but was able
to describe visualization of insects all over the room. She
P. Fernandes, L. Dolan, and S. L. WeinsteinFigure 2 (left) and Figure 3 (right). Sitting anterior-posterior and lateral post-operative radiographs.
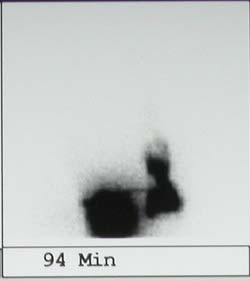
tartrate). On POD 4 a pediatric psychiatry consultation was obtained and the hypothesis of ITB withdrawal was suggested. Pump malfunction was now considered. Halo-peridol (2.5 mg at night and 2.5-5 mg PRN as a rescue dose for breakthrough agitation) was ordered. Telem-etrics ruled out pump malfunction (setting: 225μg/day, 9.4 μg/hour). The last refill had been two months before surgery. Cerebro-spinal fluid results were as follows: glucose 54 mg/dl (normal >50% serum level), protein 160 mg/dl (normal, 14 - 45 mg/dl), 150 nucleated cells/μL (normal, <5 cells/μL) and 7534 red blood cells(RBC)/μL (normal =0 RBC/μL) with xanthochromia evident. After the reservoir was filled with a radionuclide, a significant accumulation of the isotope tracer was revealed outside the spinal canal by scintigram (Figures 4, 5). Therefore,
Figure 1. Sitting anterior-posterior pre-operative radiograph.
the most likely diagnosis for the symptoms was baclofen withdrawal syndrome caused by a catheter leak. Oral
was afebrile, heart rate was 133 beats per minute, blood
baclofen with rapid titration up to 60mg/day and halo-
pressure was 109/59 mmHg and respiratory rate was
peridol were started with resolution of the symptoms
18 per minute. Hemoglobin and hematocrit were 12.2
within 72 hours. The patient was discharged on POD
g/dl and 33 percent, respectively. The metabolic workup
8 and was kept on oral baclofen until six months post-
was normal. She was on hydromorphone (Dilaudid),
operatively when the catheter was revised.
morphine, codeine, acetaminophen, diphenydramine, and promethazine. With the hypothesis of drug-related
DISCUSSION
delirium, the morphine was discontinued. Despite these
Intrathecal baclofen withdrawal syndrome should al-
measures, the patient continued to be symptomatic with
ways be considered as a possible complication after pos-
increased spasticity and visual hallucinations, and sleep
terior spinal instrumentation for cerebral palsy patients
disturbance. On POD 3 all hydromorphone, codeine,
with a baclofen pump. Compromised communication
and diphenydramine was discontinued and she was
abilities in these patients and the possible confusion with
switched to oral acetaminophen and Ambien® (zolpidem
epileptic seizure or post-operative sepsis can challenge
Intrathecal Baclofen Withdrawal Syndrome following Posterior Spinal Fusion for Neuromuscular Scoliosis
tion, the catheter can be breached accidentally; if this is recognized, it should be repaired by a proper tube connector. During the procedure, the catheter can also be caught by one of the many instruments in the field and pulled out to a level distal to the intended level or even from the spinal canal itself. If a unit rod is used, pas-sage under a taut catheter can be problematic unless a reasonable amount of catheter has been mobilized. This technical difficulty can be avoided if the neurosurgeon leaves extra catheter coiled near the spine, or by using a modular system. For example, Alden et al. reported a case where the catheter was left in place during posterior
Figure 4 (left) and Figure 5 (right). Radionuclide study at 0 minutes and at 94 minutes showing tracer leak outside spinal column.
spinal fusion for scoliosis. The patient was readmitted for hyperthermia and severe spasms with clonus in both upper and lower extremities. Pump interrogation
the proper diagnosis. When IBWS is suspected, a com-
showed no problems, but catheter exploration and divi-
plete work-up may have to be undertaken to delineate
sion near the spinal entrance revealed no spontaneous
Hallucinations in this setting can be very disturbing,
The last alternative that may be considered is to sec-
as patients tend to develop paranoic ideas with intense
tion the catheter during the procedure and then recon-
anxiety. This has also been reported in patients with
nect it with the appropriate connector at the end of the
Parkinson’s disease who take oral baclofen, but usually
procedure. If this is done, it must be coordinated with the
disappears soon after reintroduction of the drug.14,15
neurosurgical service to insure that the pump catheter
In this case, the probable cause for the withdrawal
system is functioning properly afterward.
syndrome was a small nick created in the catheter
Treatment of IBWS relies on reinstitution of the
tubing during the dissection process. To prevent this
intrathecal baclofen infusion. In severe cases, bolus
complication, three options are available to the surgeon:
administration via lumbar puncture may be needed until
The catheter can be removed during exposure and
catheter reinsertion is attempted. In the case related
reintroduced at the end of the procedure with a Thuhy
above, the differential diagnosis has to be made between
needle; catheter preservation can be attempted through
autonomic dysreflexia, malignant hyperthermia and
delicate dissection and isolation; or the catheter can be
neuroleptic malignant syndrome. Dantrolene (10mg/
sectioned and reattached at the end of the procedure
kg) or benzodiazepine infusions can be very effective
and even life-saving.9,21 If the problem is recognized early,
Although the first option seems straightforward, it has
high-dose oral or enteric baclofen (>120 mg/day in six
been related to low-pressure headaches secondary to
to eight divided doses for adults) can be effective if the
presumed cerebrospinal fluid (CSF) leakage. Segal et al.
patient’s condition permits.9 In children younger than
presented five patients with spastic quadriplegia having
12 years of age, lower doses may have to be used since
a baclofen pump who underwent posterior spinal fusion
safety is not well established and the manufacturer’s rec-
and then developed persistent positional headaches and
ommended maximum daily dose is 80 mg. Side effects
vomiting, with an inability to sit upright for some time in
such as sedation, general nervous system depression
two patients. These symptoms were due to cerebrospinal
and hypotension should be well monitored.
fluid leaks after reintroduction of the catheter. These potentials should always be anticipated when this first
CONCLUSION
Increasing numbers of patients with spastic cerebral
For a number of years, the senior author has per-
palsy are being treated with ITB. Those scheduled for
formed posterior spinal fusion by isolating the catheter,
posterior spinal fusion and instrumentation should be
mobilizing as much of it as possible, and protecting it
made aware of the potentially devastating complications
during surgery (the second alternative). Although this
associated with interruption of intrathecal baclofen which
method avoids the morbidity associated with CSF leaks
may occur as a complication of surgery. Surgeons must
and the need for additional procedures to restore the
be aware of this potential risk and develop strategies
pump catheter system, this approach has some potential
to prevent interruption of baclofen delivery and to deal
complications. Injury to the catheter may occur at many
with a disruption, should it occur. Early recognition of
points in the procedure. During dissection and mobiliza-
ITB withdrawal syndrome is mandatory, as it can be a
P. Fernandes, L. Dolan, and S. L. Weinstein
potentially life-threatening complication. Full investiga-
11. Kao LW, Amin Y, Klirk M, Turner M. Intrathecal
tion, according to established protocols, is essential to
baclofen withdrawal mimicking sepsis. J. Emerg Med
rule out all possible causes for ITB delivery failure.
12. Tur ner MR, Gainsborough N. Neuroleptic REFERENCES
malignant-like syndrome after abrupt withdrawal of
Greenberg MI, Hendrickson RG. Baclofen with-
baclofen. J Psychopharmaco 2001;15(1):61-63.
drawal following removal of an intrathecal baclofen
13. Penn RD, York NM. Catheter systems for intrathe-
pump despite oral baclofen replacement. Clin Toxicol-
cal drug delivery. J Neurosurg 1995; 83:215-7.
14. Lees AJ, Clarke CRA, Harrison MJ. Hallucinations Swigar ME, Bowers MB. Baclofen withdrawal and
after withdrawal of baclofen. Lancet 1977; 1(8016):
neuropsychiatric symptoms: a case report and review
of other case literature. Compr Psychiatry 1986; 27:
15. Stien R. Hallucinations after sudden withdrawal of
baclofen. Lancet 1977; 2(8027): 444-5. Hyser CL, Drake ME. Status epilepticus after ba-
16. Food and Drug Administration Med Watch. 2002
clofen withdrawal. J Natl Med Assoc 1984; 76(5):533-
Safety Alert – Lioresal (baclofen injection). Accessed
November 28, 2007. http://www.fda.gov/medwatch/
Garbedian-Ruffalo SM, Ruffalo RL. Adverse ef-
fects secondary to baclofen withdrawal. Drug Intell
17. Alden TD, L ytle RA, Park TS, Noetzel MJ, Clin Pharma 1985; 19:304-306. Ojemann JG. Intrathecal baclofen withdrawal: case Rivas D, Chancellor MB, Hill K, Freedman M.
report and review of the literature. Child’s Nerv Syst
Neurological manifestations of baclofen withdrawal.
J Urology 1993; 150:1903-1905.
18. Pasquier Y, Cahana A, Schnider A. Subdural Olmedo R, Hoffman RS. Withdrawal syndromes.
catheter migration may lead to baclofen pump dys-
Emerg Med Clin North Am 200; 18(2): 273-88.
function. Spinal cord 2003; 41:700-7002. Barker I, Grant IS. Convulsions after abrupt with-
19. Bardutzky J, Tronnier V, Schwab S, Meinck HM.
drawal of baclofen. Lancet 1982;2:556-7.
Intrathecal baclofen for stiff-person syndrome: life-
Mandac BR, Hurvitz EA, Nelson V. Hyperthermia
threatening intermittent catheter leakage. Neurology
associated with baclofen withdrawal and increased
spasticity. Arch Phys Med Clin North AM, 2000:18:273-
20. Segal LS, Wallach DM, Kanev PM. Potential
complications of posterior spine fusion and instru-
Coffey RJ et al. Abrupt withdrawal syndrome from
mentation in patients with cerebral palsy treated with
intrathecal baclofen: recognition and management
intrathecal baclofen infusion. Spine 2005; 30(8):E219-
of a potentially life-threatening syndrome. Arch Phys Med Rehabil. 2002; 83:735-41.
21. Reeves RK, Stolp-Smith KA, Christopherson
10. Green LB, Nelson VS. Death after acute withdrawal MW. Hyperthermia, rhabdomyolysis, and dissemi-
of intrathecal baclofen: case report and literature
nated intravascular coagulation associated with ba-
review. Arch Phys Med Rehabil 1999;80:1600-4.
clofen pump catheter failure. Arch Phys Med Rehabil1998;79:353-356.
IV Thiotepa/Busulfan/Fludarabine/ATG for Unrelated Donor Allograft INDICATIONS Acute myeloid leukaemia, acute lymphoblastic leukaemia, non-Hodgkin’s lymphoma: for unrelated donor allogeneic transplants PRE-ASSESSMENT • Ensure pre-transplant investigations are carried out as per protocol B3.10b • Ensure patient has triple or double lumen Hickman line insitu. • Ensure


 P. Fernandes, L. Dolan, and S. L. Weinstein
Figure 2 (left) and Figure 3 (right). Sitting anterior-posterior and
P. Fernandes, L. Dolan, and S. L. Weinstein
Figure 2 (left) and Figure 3 (right). Sitting anterior-posterior and 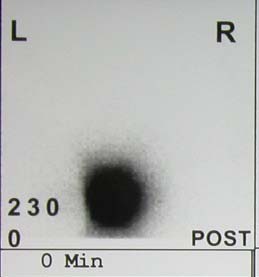
 Intrathecal Baclofen Withdrawal Syndrome following Posterior Spinal Fusion for Neuromuscular Scoliosis
tion, the catheter can be breached accidentally; if this is recognized, it should be repaired by a proper tube connector. During the procedure, the catheter can also be caught by one of the many instruments in the field and pulled out to a level distal to the intended level or even from the spinal canal itself. If a unit rod is used, pas-sage under a taut catheter can be problematic unless a reasonable amount of catheter has been mobilized. This technical difficulty can be avoided if the neurosurgeon leaves extra catheter coiled near the spine, or by using a modular system. For example, Alden et al. reported a case where the catheter was left in place during posterior
Figure 4 (left) and Figure 5 (right). Radionuclide study at 0 minutes
Intrathecal Baclofen Withdrawal Syndrome following Posterior Spinal Fusion for Neuromuscular Scoliosis
tion, the catheter can be breached accidentally; if this is recognized, it should be repaired by a proper tube connector. During the procedure, the catheter can also be caught by one of the many instruments in the field and pulled out to a level distal to the intended level or even from the spinal canal itself. If a unit rod is used, pas-sage under a taut catheter can be problematic unless a reasonable amount of catheter has been mobilized. This technical difficulty can be avoided if the neurosurgeon leaves extra catheter coiled near the spine, or by using a modular system. For example, Alden et al. reported a case where the catheter was left in place during posterior
Figure 4 (left) and Figure 5 (right). Radionuclide study at 0 minutes