Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Mtct protocol
Prevention of mother-to-child transmission of HIV has become the flagship programme in the Western Cape Province and a shining example to the rest of the country and continent. Already, sixty percent of pregnant women attending public sector maternity services have access to MTCT prevention. By June 2002, this will have increased to ninety percent and universal coverage will be achieved by March 2003.
The MTCT prevention programme will save more than a thousand babies from HIV each year. When new regimens become available this number will be even higher until we reach a point when it will be a rare event for a baby to be born HIV positive in the Western Cape.
The MTCT programme has had wider spin-offs that are as important as its
direct effects. It has taken away the secrecy surrounding HIV. As more than
30 000 women have been tested for HIV in this programme over three
years the epidemic is no longer buried deep in the labyrinth of private life
but talked about openly. The public benefits of this must be substantial.
Another spin-off of the MTCT programme is that it has united us all
against the virus. Our decision to implement the programme has brought
together government, NGOs, clinicians and the community. A failure to
implement this programme would have split us all apart. Through MTCT prevention we have become one winning team.
The main reason for the success of the MTCT prevention programme is
that we have a large number of nurses, doctors, counsellors and other staff
Above – From “Mother to Child”, a film documenting the MTCT
who have shown such dedication and commitment to implementing this
programme that we could not fail. These wonderful individuals work in
Gauteng, courtesy Steps For The Future Initiative
provincial hospitals and MOUs, local authority clinics and NGOs.
Cover – From the Partnership Against Aids, Courtesy, National Department
This protocol has been written for these health workers. It will be a guide
and a learning tool to help them with the daily work of MTCT prevention throughout the Western Cape. It will also be of use to managers, patients, private health facilities and our colleagues in neighbouring provinces.
Two versions of the protocol have been published. A detailed protocol containing all the elements of the programme and a shorter, punchier version which serves as a quick reference. Make sure you get both! Many individuals have contributed to the preparation of this protocol and I would like to end by thanking them sincerely. Dr. Fareed Abdullah Deputy Director-General
Department of Health Western Cape ProvinceMarch 2002
Summary MTCT Protocol, Western Cape Province Page 1
The Department of Health of the Provincial Administration of the Western Cape (PAWC) has made
every effort to ensure the accuracy of the information in this protocol. The protocol may be freely
adapted and utilised in other settings on condition of appropriate acknowledgement of the source.
The information contained herein is being provided as submitted and PAWC makes no
representations or warranties, either express or implied, as to its accuracy, completeness or
appropriateness for a particular purpose. PAWC accepts no responsibility or liability with regard to
the reliance upon, or use of, such information outside of the mother-to-child transmission
prevention programme in the Western Cape.
The mention of certain manufacturer’s products does not imply that they are endorsed or
recommended by PAWC in preference to others of a similar nature that are not mentioned.
Summary MTCT Protocol, Western Cape Province Page 2
The purpose of this document is to rapidly orientate the midwife and attending medical staff on how to manage an HIV positive woman who comes into a nevirapine-based MTCT programme in the Western Cape Province. This summary protocol should be used in conjunction with:
the flowcharts that are included with this document
the various registers and stationary which are provided for the programme (indicated in bold in this protocol)
the full MTCT protocol which provides further resources for implementing the programme
Please note the guidelines for the management of HIV positive women are to be used together with the
obstetric management policies for the health facility. As situations arise, i.e. massive bleeding, elevated blood pressure, premature labour etc.; the i
precedence over the guidelines for the management of HIV positive women.
Overleaf is a list of registers and documents that should be available in the health facility. Copies of all of these appear in the full protocol.
Summary MTCT Protocol, Western Cape Province Page 3
4. Combined Counselling and Testing Register
6. Hospital Labour Ward Nevirapine Register 7. Hospital Baby Nevirapine Register
8. Milk Register 9. Baby Clinic Blood Test Register
10. Baby Clinic Post 9-Month Follow-up Register 11. Baby Register
2. Screening tool to identify mothers at risk
2. Identification stickers for antenatal
1. Rapid test instructions, and stock control forms 2. MTCT Consent Form 3. Nevirapine information card for mothers who are given nevirapine to take home
Summary MTCT Protocol, Western Cape Province Page 4
(1) At the booking visit all pregnant women will receive group health education on HIV/AIDS,
voluntary counselling and testing (VCT), and information on mother to child transmission (MTCT) of HIV.
(2) All new antenatal patients will in addition receive individual pre-test information and counselling
(3) If the patient consents to HIV testing, she will sign a consen
(4) After she has signed consent for HIV testing, she will go to the blood room, blood will be taken
and a rapid HIV test will be done. A licensed practitioner (midwife or laboratory assistant) must do the rapid HIV test.
(5) If the first test is negative, the woman is considered HIV-negative.
(6) If the first rapid test is positive, a second rapid test is done on a second sample using a different
If both tests are positive, the woman is HIV-positive
If the first test is positive and the second test is negative the woman is HIV
If HIV status is indeterminate, a blood sample must be sent to the laboratory (SAIMR/NHLS) for re-testing by the ELISA technique.
(8) After the test has been performed, the midwife or laboratory assistant will enter the results in the
er. Laboratory results must be given to the midwife or counsellor for post-
(9) All women regardless of their HIV status must receive post-test counselling. All pre and post-test
counselling sessions will be recorded in the Couns
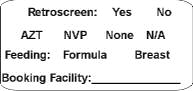
(10) If the woman tests HIV positive, she will be informed about the programme and offered
l stickers on their antenatal cards and folders. These are to be
completed by circling the appropriate choices, and entering the booking facility name.
Summary MTCT Protocol, Western Cape Province Page 5
(1) The midwife who palpates the pregnant woman in the antenatal clinic will ensure she returns at a
gestational age of 30 weeks in order for nevirapine to be dispensed. This (the anticipated visit) must be recorded in the Ant
(2) When the woman returns at 30 weeks gestation, the midwife dispenses a 200mg dose of
nevirapine. The midwife will also instruct the patient to take the nevirapine when she goes into labour or experiences rupture of membranes. This (the dispensing of nevirapine) is recorded in the Ant
(3) If a patient books at or after 29 weeks gestation the nevirapine will be given at the booking visit. (4) A card with written instructions will be given to the patient with the dose of nevirapine.
(5) If the pregnant woman is HIV infected, during antenatal care she will receive ongoing counselling
from attending midwives about breast milk transmission and about options to prevent transmission through replacement feeding or minimise transmission through exclusive breast-feeding. The patient should be assisted in making a decision on how to feed the baby prior to going into labour.
(6) Near term the patient must be re-educated regarding the taking of the nevirapine: with onset of
The midwife must also check that the patient
knows to present in early labour or immediately after rupture or membranes
has made a decision about how to feed her baby – choosing replacement feeding or
(7) The midwife must make sure that all the information is recorded on the antenata
the antenatal card and in the patient’s folder.
(8) All women will be informed of support groups within their area, or of a support group within the
Summary MTCT Protocol, Western Cape Province Page 6
COUNS ELLING REGISTER
APPL Y ANTEN ATAL STICKERS TO ANTEN ATAL C ARD AND TO FOLDER, AND DO R APID TES TING
BLOOD TEST REGISTER BLOOD TEST REGISTER COUNSELLING REGISTER COUNSELLING REGISTER MARK ANTENATAL STICKER: N/A MARK ANTENATAL STICKER: NVP MARK ANTENATAL STICKER: NONE ANTENATAL NEVIRAPINE REGISTER
CHILDBIRTH EDUCATION + CHECK NEVIRAPINE + COUNSEL &
DECIDE RE: FEEDING + FAMILY PLANNING + SUPPORT GROUP
Summary MTCT Protocol, Western Cape Province Page 7
Please note the guidelines for the management of HIV positive women are to be used together with the obstetric management policies for the health facility. As situations arise, i.e. massive bleeding, elevated blood pressure, premature labour etc.; the i
mother and baby takes precedence over the guidelines for the management of HIV positive women.
Upon admission, midwives should inquire if the woman took nevirapine at home.
If the patient is found to be in labour or to have ruptured membranes and did not take the nevirapine at home, she should be instructed to take her dose immediately.
If the patient does not have the nevirapine tablet distributed in clinic, she will be given a dose of nevirapine from the facility’s supply.
If nevirapine is re-dispensed, this must be documented in the Labou
labour ward. The reason for re-dispensing must be documented e.g. forgot, lost, false labour etc.
In the case of false labour or mistaken rupture of membranes: If the patient is evaluated before she has taken her nevirapine and is found to not be in true labour and not to have ruptured membranes, she is sent home to await more active labour. She is instructed to take her nevirapine with the onset of stronger and more regular contractions or with rupture of membranes. If she is evaluated after she has taken her nevirapine and is found not to be in true labour and not to have ruptured membranes, she is given another nevirapine tablet and sent home to await more active labour, and instructed to take this dose if active labour or rupture of membranes occur more than 24 hours after the initial dose. If a second dose is dispensed to the mother, this must also be recorded in the Labou
on a second occasion after taking a second nevirapine tablet and is still not in active labour, she is referred to a hospital for management.
In the case of an elective caesarean section, the nevirapine should be given at least 4 hours before surgery.
In the case of emergency caesarean section, nevirapine should have already been administered during labour.
Women can be given nevirapine in all stages of labour. It is only too late to give nevirapine if
the baby is delivering imminently (the head is crowning).
If a mother knows she is HIV-positive at delivery but is not in the MTCT programme, she may be offered nevirapine for her and her baby as
mme, including feeding practices and the importance of care, follow-up and HIV testing
for her baby. In such cases a clear plan should be made for infant follow-up and the provision of formula if required. (See circular H13/2002 in the Western Cape Province)
When the mother has not received nevirapine during labour, or has taken her nevirapine dose
less than two hours before delivery, the baby receives two doses of nevirapine (see page 10, item 3)
Artificial rupture of membranes should not be undertaken if progress of labour is adequate. Prolonged rupture of membranes should be avoided.
Summary MTCT Protocol, Western Cape Province Page 8
TAKE NEVIRAPINE NOW LABOUR NEV IRAPINE REGISTER REFERRAL LETTER LABOUR NEVIRAPINE REGISTER LABOUR NEVIRAPINE REGISTER
Summary MTCT Protocol, Western Cape Province Page 9
Management of the Neonate in the Obstetric Faci
Please note that in the case of premature births, appropriate adjustments to feeding and supplementation regimens will need to be made according to local guidelines for premature neonates and infants
(1) Nevirapine syrup is given to the baby within 4 to 72 hours of delivery. It is given at least one hour
prior to discharge in order to observe the baby for this period.
(2) If the baby vomits within one hour of nevirapine, a second dose of nevirapine is given and the
baby is observed for another hour. A third dose of nevirapine should not be given.
(3) If the mother did not take nevirapine or took her dose of nevirapine less than two hours prior to
delivery, the baby gets two doses of nevirapine, the first dose within one hour of life and a second dose one hour prior to discharge (and at least four hours after the first dose). If the baby will be in the MOU or nursery for longer, it is preferable to give the second dose of nevirapine later, up to 48-72 hours of life.
(4) This information (details of nevirapine given to the neonate) is recorded in the Labo
(5) Babies should receive their routine immunisations (OPV and BCG) in their first hours of life.
(6) If the baby is born outside of the MOU or hospital and presents to the clinic within 72 hours of
delivery (when the mother is known to be HIV-positive and is in the MTCT programme or gives her consent), nevirapine may be given to the baby as above. This should be noted on the baby register as ‘BBA’.
(7) On the Road to Health Card (RTHC), the baby will receive a MTCT bab
staff to identify the child at subsequent visits.
(8) The nursing staff must ask the mother what she decided antenatally about feeding her baby and
consult the antenatal sticker on the antenatal card. The baby must not be latched until the midwife knows the infant feeding method chosen by the mother.
(9) If the mother chooses to formula feed, the care provider (midwife, nurse or doctor) must ensure
the mother knows how to sterilise and mix the formula before discharge. An initial supply of
formula (1 kg) is supplied from the MOU or hospital and documented in the Mil
(10) If the mother chooses to breast-feed, EXCLUSIVE breast-feeding (nothing else but breast milk – no
tea, water or cereal) is strongly encouraged. This must take place for four months and the mother should rapidly wean the baby soon thereafter (consult the full MTCT protocol for details).
(11) The importance of clinical follow-up for the baby should be reinforced, and referral to a local clinic
that can provide appropriate follow-up is arranged.
Summary MTCT Protocol, Western Cape Province Page 10
TO BABYAT 60 MINS & 2ND DOSE AS
INDICATED BELOW (BUT AT LEAST 4 HRS MOU LABOUR NEVIRAPINE REGISTER HOSPITAL BABY NEVIRAPINE REGISTER NEONATAL NEVIRAPINE >4 HRS POST DELIVERY MOU LABOUR NEVIRAPINE REGISTER HOSPITAL BABY NEVIRAPINE REGISTER
< 72 HOURS AFTER DELIVE RY DOSE: BW >2kg = 0.6 ml BW <2kg = 0.2 ml/kg MOU LABOUR NEVIRAPINE REGISTER HOSPITAL BABY NEVIRAPINE REGISTER LABOUR NEVIRAPINE REGISTER BABY STICKER ONTO RTHC + PAEDIATRIC REFERRAL LETTER HOSPITAL BABY NEVIRAPINE REGISTER
Summary MTCT Protocol, Western Cape Province Page 11
(1) All HIV-exposed babies in the MTCT programme should arrive from the MOU or hospital within
one to two weeks of birth with a referral letter and sticker on the Road to Health Card. HIV care needs are further noted by the presence of a co-trimoxazole dosage and the need for formula.
(2) All babies are weighed, and the weight documented in the RTH card.
(3) Feeding practices are noted and reinforced. In particular, for those formula feeding the sister will
check the method of cleaning feeding utensils and mixing of formula, and for those breast-feeding, the sister will check the mother understands the concept of exclusive breast-feeding, that weight gain is adequate, and if necessary re-counsel the mother on her feeding choice.
(4) For each formula fed baby in the programme the clinic provides 2kg of formula (four 500g tins)
every fortnight (4 kgs per month) until six months of age. This is documented in the Bab
(5) Multivitamins (containing Vitamin A) are given to HIV exposed infants for nutritional support until
HIV infection is excluded. If multivitamins are not available, Vitamin A supplements should be given according to the schedule below every 6 months and documented on the RTHC.
(6) At six weeks of age all MTCT babies will begin co-trimoxazole prophylaxis three times per week.
This will continue until they are 12 months old or test negative for HIV. Co-trimoxazole is
continued beyond 12 months if the baby is HIV-positive and has symptoms of HIV such as: growth faltering, recurrent bacterial infections, pneumonia, thrush, severe nappy rash or has ever had PCP.
(7) Co-trimoxazole is dosed by weight and can be given once a day, three times a week – Monday,
Wednesday and Friday. The following is the once a day dosage. If given twice a day (bd) the dose should be divided in half.
(8) After formula is discontinued at 6 months, or after weaning for those babies being exclusively
breast-fed, the babies should be assessed within two to four weeks to see if there is evidence of growth faltering or if the baby otherwise meets the PEM criteria for ongoing formula or maize meal supplements.
tions to co-trimoxazole are rare but can present as generalised body rashes. If a mild
rash occurs refer the same day to an experienced HIV clinician for evaluation and possible switching to Dapsone (2 mg/kg daily).
sh involving skin, mouth, red eyes (if scabies or impetigo are ruled out) is a medical
emergency. Co-trimoxazole is stopped and the baby is immediately referred to a tertiary hospital. Switching to Dapsone will be required.
Summary MTCT Protocol, Western Cape Province Page 12
MTCT BABY REGISTER
CHECKFEEDING METHODS?GROWTH FALTERING?THRUSH / NAPPY RASH
?INTER-CURRENT DISEASE?DIARRHOEA / COUGH?TB CONTACTS
& RED EYES - REFER IMMEDIATELY
AT 9 MONTHS – Proceed to testing algorithm / flowchart
Summary MTCT Protocol, Western Cape Province Page 13
(11) Professional nurses see babies at two and six weeks and then every four to six weeks coordinated
with the immunisation schedule. The suggested visit schedule for the first year of life is: Weeks: 6,10,14 and18 and Months: 6,9,12,15, and 18. This can be increased if needed. In addition mothers will return every two weeks to collect formula feeds.
(12) Follow-up occurs at weeks 26 and 28 (seven months) to see if babies can sustain their weight after
the formula has been discontinued at six months.
(13) At monitoring visits the professional nurse should assess for the following clinical conditions. If they
are present, the baby is referred to a clinical nurse practitioner or doctor. The nurse:
checks for oral thrush or sores and nappy rash;
checks for fevers, if the baby is floppy or irritable;
(14) The professional nurse should also routinely asses:
The mother’s coping and general health. She encourages clinic visits for the mother and
Adherence with immunisations as per paediatric schedules.
The need for anti-worm treatment. This should be considered every six months starting at one year of age using Mebendazole (5 ml bd for 3 days) or Albendazole (200mg).
(1) All babies should be tested at 9 months using rapid HIV tests as for adults. Blood can be obtained
via heel sticks. The 9-month visit can be coordinated with the immunisation visit.
(2) At 9 months or at any age, an HIV-negative test means the baby is uninfected (unless the baby is
being breast-fed). An HIV-negative baby can be “graduated” from the MTCT programme.
(3) For babies with a positive HIV test at nine months, parents should be told that this may be a ”false
positive” result because some babies are slow in clearing their maternal antibodies. They will need to be re-tested at eighteen months.
(4) Babies testing positive at 9 months are entered into the Bab
(5) At 18 months, all remaining HIV-positive babies should be retested. By 18 months, all uninfected
(6) Breast-fed babies can contract the infection from breast milk. All breast-fed babies, even if testing
negative at 9 or 18 months, should be retested 3 months after weaning from breast milk.
(7) All test results are documented in the Baby C
Summary MTCT Protocol, Western Cape Province Page 14
RAPID TESTING AT 9 OR 18 MONTHS BLOOD TEST REGISTER BLOOD TEST REGISTER MTCT BABY REGISTER MTCT BABY REGIS TER POST 9-MONTH BABY FOLLOW-UP REGISTER
* unless breast-feeding is ongoing or was stopped in the last three months
Summary MTCT Protocol, Western Cape Province Page 15
They hold heir thrones in stewardship from God--responsible to Him. Consciously or unconsciously, all parents have adopted someform of government for their home. Some the tyrannical or dictatorialapproach, others the democratic, still others thematriarchal/patriarchal style. There are those who have chosenanarchy--with no law and even less order--while some jump from onetype to another, employin
Revisão da Literatura Evidências de eficácia da terapia cognitiva Evidences from the efficacy of the cognitive behavior therapy on schizophreniaElizA MARtHA dE PAivA bARREto1 , Hélio Elkis2 1 Psiquiatra, mestre em Psiquiatria pela Universidade de São Paulo (USP). Fellow em terapia cognitiva e comportamental pelo Departamento de Psiquiatria do Massachusetts General Hospital (EUA).













 Prevention of mother-to-child transmission of HIV has become the flagship programme in the Western Cape Province and a shining example to the rest of the country and continent. Already, sixty percent of pregnant women attending public sector maternity services have access to MTCT prevention. By June 2002, this will have increased to ninety percent and universal coverage will be achieved by March 2003.
The MTCT prevention programme will save more than a thousand babies from HIV each year. When new regimens become available this number will be even higher until we reach a point when it will be a rare event for a baby to be born HIV positive in the Western Cape.
The MTCT programme has had wider spin-offs that are as important as its
direct effects. It has taken away the secrecy surrounding HIV. As more than
30 000 women have been tested for HIV in this programme over three
years the epidemic is no longer buried deep in the labyrinth of private life
but talked about openly. The public benefits of this must be substantial.
Another spin-off of the MTCT programme is that it has united us all
against the virus. Our decision to implement the programme has brought
together government, NGOs, clinicians and the community. A failure to
implement this programme would have split us all apart. Through MTCT prevention we have become one winning team.
The main reason for the success of the MTCT prevention programme is
that we have a large number of nurses, doctors, counsellors and other staff
Above – From “Mother to Child”, a film documenting the MTCT
who have shown such dedication and commitment to implementing this
programme that we could not fail. These wonderful individuals work in
Gauteng, courtesy Steps For The Future Initiative
provincial hospitals and MOUs, local authority clinics and NGOs.
Cover – From the Partnership Against Aids, Courtesy, National Department
This protocol has been written for these health workers. It will be a guide
and a learning tool to help them with the daily work of MTCT prevention throughout the Western Cape. It will also be of use to managers, patients, private health facilities and our colleagues in neighbouring provinces.
Two versions of the protocol have been published. A detailed protocol containing all the elements of the programme and a shorter, punchier version which serves as a quick reference. Make sure you get both! Many individuals have contributed to the preparation of this protocol and I would like to end by thanking them sincerely. Dr. Fareed Abdullah Deputy Director-General
Department of Health Western Cape ProvinceMarch 2002
Summary MTCT Protocol, Western Cape Province Page 1
The Department of Health of the Provincial Administration of the Western Cape (PAWC) has made
every effort to ensure the accuracy of the information in this protocol. The protocol may be freely
adapted and utilised in other settings on condition of appropriate acknowledgement of the source.
The information contained herein is being provided as submitted and PAWC makes no
representations or warranties, either express or implied, as to its accuracy, completeness or
appropriateness for a particular purpose. PAWC accepts no responsibility or liability with regard to
the reliance upon, or use of, such information outside of the mother-to-child transmission
prevention programme in the Western Cape.
The mention of certain manufacturer’s products does not imply that they are endorsed or
recommended by PAWC in preference to others of a similar nature that are not mentioned.
Summary MTCT Protocol, Western Cape Province Page 2
The purpose of this document is to rapidly orientate the midwife and attending medical staff on how to manage an HIV positive woman who comes into a nevirapine-based MTCT programme in the Western Cape Province. This summary protocol should be used in conjunction with:
the flowcharts that are included with this document
the various registers and stationary which are provided for the programme (indicated in bold in this protocol)
the full MTCT protocol which provides further resources for implementing the programme
Please note the guidelines for the management of HIV positive women are to be used together with the
obstetric management policies for the health facility. As situations arise, i.e. massive bleeding, elevated blood pressure, premature labour etc.; the i
precedence over the guidelines for the management of HIV positive women.
Overleaf is a list of registers and documents that should be available in the health facility. Copies of all of these appear in the full protocol.
Summary MTCT Protocol, Western Cape Province Page 3
4. Combined Counselling and Testing Register
6. Hospital Labour Ward Nevirapine Register 7. Hospital Baby Nevirapine Register
8. Milk Register 9. Baby Clinic Blood Test Register
10. Baby Clinic Post 9-Month Follow-up Register 11. Baby Register
2. Screening tool to identify mothers at risk
2. Identification stickers for antenatal
1. Rapid test instructions, and stock control forms 2. MTCT Consent Form 3. Nevirapine information card for mothers who are given nevirapine to take home
Summary MTCT Protocol, Western Cape Province Page 4
Prevention of mother-to-child transmission of HIV has become the flagship programme in the Western Cape Province and a shining example to the rest of the country and continent. Already, sixty percent of pregnant women attending public sector maternity services have access to MTCT prevention. By June 2002, this will have increased to ninety percent and universal coverage will be achieved by March 2003.
The MTCT prevention programme will save more than a thousand babies from HIV each year. When new regimens become available this number will be even higher until we reach a point when it will be a rare event for a baby to be born HIV positive in the Western Cape.
The MTCT programme has had wider spin-offs that are as important as its
direct effects. It has taken away the secrecy surrounding HIV. As more than
30 000 women have been tested for HIV in this programme over three
years the epidemic is no longer buried deep in the labyrinth of private life
but talked about openly. The public benefits of this must be substantial.
Another spin-off of the MTCT programme is that it has united us all
against the virus. Our decision to implement the programme has brought
together government, NGOs, clinicians and the community. A failure to
implement this programme would have split us all apart. Through MTCT prevention we have become one winning team.
The main reason for the success of the MTCT prevention programme is
that we have a large number of nurses, doctors, counsellors and other staff
Above – From “Mother to Child”, a film documenting the MTCT
who have shown such dedication and commitment to implementing this
programme that we could not fail. These wonderful individuals work in
Gauteng, courtesy Steps For The Future Initiative
provincial hospitals and MOUs, local authority clinics and NGOs.
Cover – From the Partnership Against Aids, Courtesy, National Department
This protocol has been written for these health workers. It will be a guide
and a learning tool to help them with the daily work of MTCT prevention throughout the Western Cape. It will also be of use to managers, patients, private health facilities and our colleagues in neighbouring provinces.
Two versions of the protocol have been published. A detailed protocol containing all the elements of the programme and a shorter, punchier version which serves as a quick reference. Make sure you get both! Many individuals have contributed to the preparation of this protocol and I would like to end by thanking them sincerely. Dr. Fareed Abdullah Deputy Director-General
Department of Health Western Cape ProvinceMarch 2002
Summary MTCT Protocol, Western Cape Province Page 1
The Department of Health of the Provincial Administration of the Western Cape (PAWC) has made
every effort to ensure the accuracy of the information in this protocol. The protocol may be freely
adapted and utilised in other settings on condition of appropriate acknowledgement of the source.
The information contained herein is being provided as submitted and PAWC makes no
representations or warranties, either express or implied, as to its accuracy, completeness or
appropriateness for a particular purpose. PAWC accepts no responsibility or liability with regard to
the reliance upon, or use of, such information outside of the mother-to-child transmission
prevention programme in the Western Cape.
The mention of certain manufacturer’s products does not imply that they are endorsed or
recommended by PAWC in preference to others of a similar nature that are not mentioned.
Summary MTCT Protocol, Western Cape Province Page 2
The purpose of this document is to rapidly orientate the midwife and attending medical staff on how to manage an HIV positive woman who comes into a nevirapine-based MTCT programme in the Western Cape Province. This summary protocol should be used in conjunction with:
the flowcharts that are included with this document
the various registers and stationary which are provided for the programme (indicated in bold in this protocol)
the full MTCT protocol which provides further resources for implementing the programme
Please note the guidelines for the management of HIV positive women are to be used together with the
obstetric management policies for the health facility. As situations arise, i.e. massive bleeding, elevated blood pressure, premature labour etc.; the i
precedence over the guidelines for the management of HIV positive women.
Overleaf is a list of registers and documents that should be available in the health facility. Copies of all of these appear in the full protocol.
Summary MTCT Protocol, Western Cape Province Page 3
4. Combined Counselling and Testing Register
6. Hospital Labour Ward Nevirapine Register 7. Hospital Baby Nevirapine Register
8. Milk Register 9. Baby Clinic Blood Test Register
10. Baby Clinic Post 9-Month Follow-up Register 11. Baby Register
2. Screening tool to identify mothers at risk
2. Identification stickers for antenatal
1. Rapid test instructions, and stock control forms 2. MTCT Consent Form 3. Nevirapine information card for mothers who are given nevirapine to take home
Summary MTCT Protocol, Western Cape Province Page 4
 (1) At the booking visit all pregnant women will receive group health education on HIV/AIDS,
voluntary counselling and testing (VCT), and information on mother to child transmission (MTCT) of HIV.
(2) All new antenatal patients will in addition receive individual pre-test information and counselling
(3) If the patient consents to HIV testing, she will sign a consen
(4) After she has signed consent for HIV testing, she will go to the blood room, blood will be taken
and a rapid HIV test will be done. A licensed practitioner (midwife or laboratory assistant) must do the rapid HIV test.
(5) If the first test is negative, the woman is considered HIV-negative.
(6) If the first rapid test is positive, a second rapid test is done on a second sample using a different
If both tests are positive, the woman is HIV-positive
If the first test is positive and the second test is negative the woman is HIV
If HIV status is indeterminate, a blood sample must be sent to the laboratory (SAIMR/NHLS) for re-testing by the ELISA technique.
(8) After the test has been performed, the midwife or laboratory assistant will enter the results in the
er. Laboratory results must be given to the midwife or counsellor for post-
(9) All women regardless of their HIV status must receive post-test counselling. All pre and post-test
counselling sessions will be recorded in the Couns
(10) If the woman tests HIV positive, she will be informed about the programme and offered
l stickers on their antenatal cards and folders. These are to be
completed by circling the appropriate choices, and entering the booking facility name.
Summary MTCT Protocol, Western Cape Province Page 5
(1) The midwife who palpates the pregnant woman in the antenatal clinic will ensure she returns at a
gestational age of 30 weeks in order for nevirapine to be dispensed. This (the anticipated visit) must be recorded in the Ant
(2) When the woman returns at 30 weeks gestation, the midwife dispenses a 200mg dose of
nevirapine. The midwife will also instruct the patient to take the nevirapine when she goes into labour or experiences rupture of membranes. This (the dispensing of nevirapine) is recorded in the Ant
(3) If a patient books at or after 29 weeks gestation the nevirapine will be given at the booking visit. (4) A card with written instructions will be given to the patient with the dose of nevirapine.
(5) If the pregnant woman is HIV infected, during antenatal care she will receive ongoing counselling
from attending midwives about breast milk transmission and about options to prevent transmission through replacement feeding or minimise transmission through exclusive breast-feeding. The patient should be assisted in making a decision on how to feed the baby prior to going into labour.
(6) Near term the patient must be re-educated regarding the taking of the nevirapine: with onset of
The midwife must also check that the patient
knows to present in early labour or immediately after rupture or membranes
has made a decision about how to feed her baby – choosing replacement feeding or
(7) The midwife must make sure that all the information is recorded on the antenata
the antenatal card and in the patient’s folder.
(8) All women will be informed of support groups within their area, or of a support group within the
Summary MTCT Protocol, Western Cape Province Page 6
COUNS ELLING REGISTER
(1) At the booking visit all pregnant women will receive group health education on HIV/AIDS,
voluntary counselling and testing (VCT), and information on mother to child transmission (MTCT) of HIV.
(2) All new antenatal patients will in addition receive individual pre-test information and counselling
(3) If the patient consents to HIV testing, she will sign a consen
(4) After she has signed consent for HIV testing, she will go to the blood room, blood will be taken
and a rapid HIV test will be done. A licensed practitioner (midwife or laboratory assistant) must do the rapid HIV test.
(5) If the first test is negative, the woman is considered HIV-negative.
(6) If the first rapid test is positive, a second rapid test is done on a second sample using a different
If both tests are positive, the woman is HIV-positive
If the first test is positive and the second test is negative the woman is HIV
If HIV status is indeterminate, a blood sample must be sent to the laboratory (SAIMR/NHLS) for re-testing by the ELISA technique.
(8) After the test has been performed, the midwife or laboratory assistant will enter the results in the
er. Laboratory results must be given to the midwife or counsellor for post-
(9) All women regardless of their HIV status must receive post-test counselling. All pre and post-test
counselling sessions will be recorded in the Couns
(10) If the woman tests HIV positive, she will be informed about the programme and offered
l stickers on their antenatal cards and folders. These are to be
completed by circling the appropriate choices, and entering the booking facility name.
Summary MTCT Protocol, Western Cape Province Page 5
(1) The midwife who palpates the pregnant woman in the antenatal clinic will ensure she returns at a
gestational age of 30 weeks in order for nevirapine to be dispensed. This (the anticipated visit) must be recorded in the Ant
(2) When the woman returns at 30 weeks gestation, the midwife dispenses a 200mg dose of
nevirapine. The midwife will also instruct the patient to take the nevirapine when she goes into labour or experiences rupture of membranes. This (the dispensing of nevirapine) is recorded in the Ant
(3) If a patient books at or after 29 weeks gestation the nevirapine will be given at the booking visit. (4) A card with written instructions will be given to the patient with the dose of nevirapine.
(5) If the pregnant woman is HIV infected, during antenatal care she will receive ongoing counselling
from attending midwives about breast milk transmission and about options to prevent transmission through replacement feeding or minimise transmission through exclusive breast-feeding. The patient should be assisted in making a decision on how to feed the baby prior to going into labour.
(6) Near term the patient must be re-educated regarding the taking of the nevirapine: with onset of
The midwife must also check that the patient
knows to present in early labour or immediately after rupture or membranes
has made a decision about how to feed her baby – choosing replacement feeding or
(7) The midwife must make sure that all the information is recorded on the antenata
the antenatal card and in the patient’s folder.
(8) All women will be informed of support groups within their area, or of a support group within the
Summary MTCT Protocol, Western Cape Province Page 6
COUNS ELLING REGISTER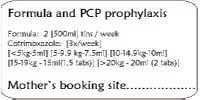 Management of the Neonate in the Obstetric Faci
Please note that in the case of premature births, appropriate adjustments to feeding and supplementation regimens will need to be made according to local guidelines for premature neonates and infants
(1) Nevirapine syrup is given to the baby within 4 to 72 hours of delivery. It is given at least one hour
prior to discharge in order to observe the baby for this period.
(2) If the baby vomits within one hour of nevirapine, a second dose of nevirapine is given and the
baby is observed for another hour. A third dose of nevirapine should not be given.
(3) If the mother did not take nevirapine or took her dose of nevirapine less than two hours prior to
delivery, the baby gets two doses of nevirapine, the first dose within one hour of life and a second dose one hour prior to discharge (and at least four hours after the first dose). If the baby will be in the MOU or nursery for longer, it is preferable to give the second dose of nevirapine later, up to 48-72 hours of life.
(4) This information (details of nevirapine given to the neonate) is recorded in the Labo
(5) Babies should receive their routine immunisations (OPV and BCG) in their first hours of life.
(6) If the baby is born outside of the MOU or hospital and presents to the clinic within 72 hours of
delivery (when the mother is known to be HIV-positive and is in the MTCT programme or gives her consent), nevirapine may be given to the baby as above. This should be noted on the baby register as ‘BBA’.
Management of the Neonate in the Obstetric Faci
Please note that in the case of premature births, appropriate adjustments to feeding and supplementation regimens will need to be made according to local guidelines for premature neonates and infants
(1) Nevirapine syrup is given to the baby within 4 to 72 hours of delivery. It is given at least one hour
prior to discharge in order to observe the baby for this period.
(2) If the baby vomits within one hour of nevirapine, a second dose of nevirapine is given and the
baby is observed for another hour. A third dose of nevirapine should not be given.
(3) If the mother did not take nevirapine or took her dose of nevirapine less than two hours prior to
delivery, the baby gets two doses of nevirapine, the first dose within one hour of life and a second dose one hour prior to discharge (and at least four hours after the first dose). If the baby will be in the MOU or nursery for longer, it is preferable to give the second dose of nevirapine later, up to 48-72 hours of life.
(4) This information (details of nevirapine given to the neonate) is recorded in the Labo
(5) Babies should receive their routine immunisations (OPV and BCG) in their first hours of life.
(6) If the baby is born outside of the MOU or hospital and presents to the clinic within 72 hours of
delivery (when the mother is known to be HIV-positive and is in the MTCT programme or gives her consent), nevirapine may be given to the baby as above. This should be noted on the baby register as ‘BBA’.