Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Ozoneultraclean.com
infection control and hospital epidemiology
Use of Gaseous Ozone for Eradication
mg/L), and linezolid (MIC, 0.75 mg/L), and was susceptibleto mupirocin by disk diffusion; the strain was resistant to
of Methicillin-Resistant Staphylococcus
oxacillin (MIC, 24 mg/L) and erythromycin (MIC, 16 mg/L)
aureus From the Home Environment
by E-test, and to clindamycin by disk diffusion test (disso-
of a Colonized Hospital Employee
ciated resistance). The other patients on the ward and thepersonnel involved with her care were screened for MRSA. Hero E. L. de Boer, MD;
In our institution, a set of screening cultures includes at least
Carla M. van Elzelingen-Dekker, BSc;
nose, throat, and perineum swab specimens and, for persons
Cora M. F. van Rheenen-Verberg, BSc;
with eczema or skin lesions, a skin swab specimen. Two other
Lodewijk Spanjaard, MD, PhD
patients and 2 nurses carried the same strain of MRSA. After8 weeks, all colonized patients had been discharged and 1nurse had multiple cultures negative for MRSA.
An intensive care nurse with eczema was repeatedly treated for meth-
Cultures of additional swab specimens of the nose and skin
icillin-resistant Staphylococcus aureus (MRSA) carriage. Because cul-
lesions from the other nurse remained positive for MRSA (Fig-
tures remained positive for MRSA, her house was investigated.
ure). She had constitutional eczema with continually fluctu-
Thirty-four percent of environmental samples yielded MRSA. Her
ating activity, which was treated with several creams. MRSA
children and cat were free of MRSA. The house was decontaminated
eradication treatment was initiated (Figure). In our institution,
with gaseous ozone. All subsequent cultures were negative for MRSA.
this approach is only attempted when eczema is quiescent. The
This decontamination cost i2,000 (approximately $2,400).
initial culture after the initiation of MRSA eradication treat-
Infect Control Hosp Epidemiol 2006; 27:1120-1122
ment was negative for MRSA, but later cultures revealed con-tinuing carriage. Three additional courses of anti-MRSA treat-
In most countries, methicillin-resistant Staphylococcus aureus
ment were prescribed. Antimicrobial agents used in the 5
(MRSA) is widespread in hospitals. In The Netherlands, na-
courses of treatment (the duration of all treatments was 7 days)
tional policy is to keep the prevalence of MRSA at the current
were as follows: courses 1 and 3, mupirocin nasal ointment,
level of less than 1% of all S. aureus isolates.1 Because hospital
chlorhexidine scrub, and vancomycin (250 mg orally every 6
employees’ hands are an important route of transmission of
hours); course 2, mupirocin nasal ointment, chlorhexidine
MRSA, cultures are regularly collected from staff in contact
scrub, vancomycin (250 mg orally every 6 hours), rifampin
with an MRSA-colonized patient to identify carriage. Em-
(600 mg orally every 24 hours), and doxycycline (100 mg orally
ployees carrying MRSA are treated with a variety of measures,
every 24 hours); and courses 4 and 5, mupirocin nasal oint-
including administration of mupirocin nasal ointment, chlor-
ment, chlorhexidine scrub, vancomycin (250 mg orally every
hexidine scrub, and orally administered antimicrobial agents.
6 hours), doxycycline (100 mg orally every 24 hours), and
Failure to eradicate carriage is often associated with a risk
linezolid (600 mg orally every 12 hours).
factor (eg, eczema or wounds), but reinfection after successful
Because the nurse had persistent MRSA colonization, re-
eradication also occurs. A possible source of MRSA outside
training for another post was considered. She became de-
hospitals is the home environment, including family mem-
pressed because of the threat of a switch from her favored
bers, pets, and surfaces of furniture. We could not find a
occupation and was treated with antidepressants. After the
published report of disinfection of rooms and furniture with
fourth course of anti-MRSA treatment, results of 3 weekly
ozone, which is often used as an industrial disinfectant but
culture sets were negative, and she returned to work in Oc-
infrequently tested for possible medical applications.2-6 This
tober 2002. However, screening cultures were positive for
report describes the successful use of gaseous ozone to erad-
MRSA a month later. All MRSA isolates from the nurse
icate MRSA in the home environment, which was responsible
showed the same susceptibility pattern, as did the isolates
for repeated infection of a nurse with eczema who had re-
from the index patient, the contact patients, and the other
nurse. The possibility of reinfection in the home was con-sidered, and environmental screening of her house was per-
formed 2 weeks later. Thirty-two sites in the house were
In December 2001, cultures of specimens from a pediatric
sampled using sweep plates containing mannitol salt agar with
intensive care patient unexpectedly yielded MRSA (phage type
2 mg/L of oxacillin. In addition, swab specimens from her 2
I64). By E-test (AB Biodisk), the strain was susceptible to
children (nose, throat, and perineum specimens) and her cat
tetracycline (minimal inhibitory concentration [MIC], 0.094
(throat, perineum, and coat specimens) were obtained. Eleven
mg/L), trimethoprim-sulfamethoxazole (MIC, 0.75 ϩ 14.25
(34%) of the environmental cultures yielded MRSA (Table).
mg/L), vancomycin (MIC, 1.5 mg/L), rifampin (MIC, !0.016
Her children and the cat tested negative for MRSA.
ozone for mrsa decontamination of the home
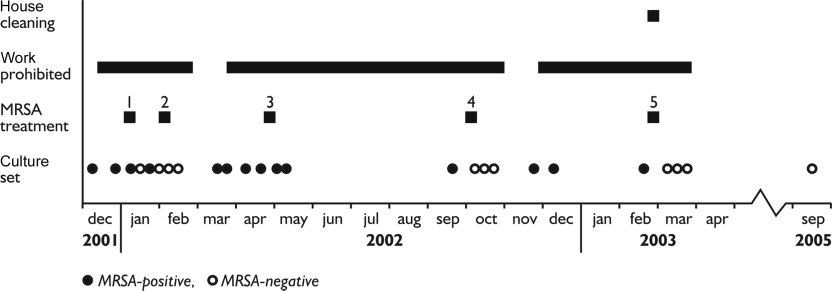
Culture results for the nurse colonized with methicillin-resistant Staphylococcus aureus (MRSA) and control measures used,
A salvage company was asked to decontaminate the house.
The company advised discarding the carpet, couch, and cur-tains and using gaseous ozone for all rooms of the house.
It is difficult to eradicate MRSA from a carrier with eczema,
The rooms were treated one after the other. Metal objects
especially when present on the hands. The risk of MRSA
were temporarily put in another room. An ozone generator
spreading into the environment is significant because of the
and ventilators were placed in the house to circulate the
high shedding of skin flakes. If eczema is in remission and
ozone, which is heavier than air. The generator produced
multiple courses of eradication therapy fail, the most likely
approximately 35 g of ozone during 10 hours and was re-
cause is reinfection from family members, pets, or the home
moved after 24 hours. The concentration of ozone was es-
environment. The last possibility appears most plausible in
timated at 12 ppm but was not measured. Each room was
this case, because the family members and pet were free of
hermetically closed during the decontamination period and
MRSA. This means that the staphylococci should have sur-
was subsequently thoroughly ventilated. The nurse, her 2 chil-
vived approximately 6 weeks in the home environment (Fig-
dren, and the cat stayed with relatives for a week. Then the
ure). Studies have shown that some MRSA isolates can in-
nurse was treated again. Two days after the house was cleaned,
deed survive in dust or on synthetics for more than 5
several specimens for culture were obtained from the house
weeks.7,8 Environmental MRSA eradication should be care-
and the nurse. All yielded negative results, and the nurse
fully planned, and the choice of the method for disinfection
started working again in April 2003. Swab specimens of the
of rooms and furniture needs to be considered. Commonly
nose, throat, perineum, and skin lesions were obtained
used hospital disinfectants, such as ethanol, chlorine, and
monthly until April 2004 and again in September 2005. All
disinfectants that are less often used in The Netherlands, such
cultures remained negative for MRSA. The cost of this de-
as phenolics and quaternary ammonium compounds, are not
contamination procedure was i2,000 (approximately $2,400:
appropriate for use with house furniture.
salvage company, i1,500; discarded furniture, i500), which
Two studies have described decontamination of the home
environment for refractory MRSA carriage in healthcare
table. Results of Cultures of Specimens Obtained From the Home EnvironmentBefore Ozone Disinfection
Armchair, carpet, cat’s scratching post,
curtains, piano, remote control, andtelephone
MRSA, methicillin-resistant Staphylococcus aureus.
infection control and hospital epidemiology
workers.9,10 Allen et al.9 used a general-purpose detergent to
we describe the successful use of gaseous ozone to eradicate
thoroughly clean all hard furnishings, whereas all carpets and
MRSA from a widely contaminated home environment.
soft furnishings were steam-cleaned. Masterton et al.10 statedthat the house was thoroughly vacuumed and damp dusted.
In both situations, some of the old furniture was replaced,
We thank the nurse and her family, for their cooperation; Mr. A. de Reus
and the hospital employee was treated together with MRSA-
and Mr. E. Meijer, for advice; Dr. R. Behrens, for critical review of the text;
colonized family members. All remained free of MRSA.
and the National Institute of Public Health and the Environment (Bilthoven),
Ozone is often used as a disinfectant in the pharmaceutical
and food industry and as a disinfectant of water and con-taminated cloths. It is the treatment of choice to clean a houseafter a fire, to eliminate the foul burnt smell. Only a few
From the Departments of Occupational Health (H.E.L.d.B) and Medical
Microbiology (C.M.v.E.-D., C.M.F.v.R.-V., L.S.), Academic Medical Center,
studies describe possible medical applications of ozone,2,3 be-
cause it is toxic, necessitating respiratory protection for work-
Address reprint requests to Lodewijk Spanjaard, MD, PhD, Laboratory of
ers, and as a potent oxidizer is detrimental to metals. Ozone
Bacteriology, Academic Medical Center, L-1-243, P.O. Box 22660, 1100 DD
oxidizes the bacterial cell wall and cytoplasmic membrane,
Amsterdam, The Netherlands (L.Spanjaard@amc.uva.nl).
and fungi are equally susceptible. The dose response for mi-
Received March 18, 2005; accepted March 18, 2006; electronically pub-
croorganism inactivation is in the following order (low to
᭧ 2006 by The Society for Healthcare Epidemiology of America. All rights
high dose): gram-negative bacteria, vegetative gram-positive
reserved. 0899-823X/2006/2710-0017$15.00.
bacteria, yeasts, molds, and Bacillus spores.5,6 The ozone con-centration necessary to kill MRSA appears to be higher than
that needed to kill methicillin-sensitive S. aureus.2,4 Berring-ton and Pedler2 tested the effect of gaseous ozone on MRSA
1. Tiemersma EW, Bronzwaer SL, Lyytikainen O, et al. Methicillin-resistant
in hospital rooms. They found that not all places in the room
Staphylococcus aureus in Europe, 1999-2002. Emerg Infect Dis 2004; 10:
became free of MRSA and therefore concluded that this
2. Berrington AW, Pedler SJ. Investigation of gaseous ozone for MRSA
method was inadequate for decontamination. However, they
decontamination of hospital side-rooms. J Hosp Infect 1998; 40:61-65.
ran the ozone generators for only 4-7 hours. On the basis of
3. Cardoso CC, Fiorini JE, Ferriera LR, Gurjao JW, Amaral LA. Disinfection
the experience of the salvage company and the favorable result
of hospital laundry using ozone: microbiological evaluation. Infect Con-
in the present case, it appears wise to use generators for 10
trol Hosp Epidemiol 2000; 21:248.
hours, along with devices to circulate the ozone. The latter
4. Yamayoshi T, Tatsumi N. Microbicidal effects of ozone solution on meth-
are necessary to disperse the gas equally, because gaseous
icillin-resistant Staphylococcus aureus. Drugs Exp Clin Res 1993; 19:59-64.
5. Moore G, Griffith C, Peters A. Bactericidal properties of ozone and its
ozone is heavier than air. All rooms should be tightly sealed
potential application as a terminal disinfectant. J Food Prot 2000; 63:
to prevent loss of ozone. After decontamination, specimens
for screening cultures should be collected. During the de-
6. Li CS, Wang YC. Surface germicidal effects of ozone for microorganisms.
contamination period, all inhabitants need to be accom-
AIHA (Fairfax, VA) 2003; 64:533-537.
modated elsewhere and MRSA carriers must be treated to
7. Neely AN, Maley MP. Survival of enterococci and staphylococci on hos-
pital fabrics and plastic. J Clin Microbiol 2000; 38:724-726.
8. Wagenvoort JH, Penders RJ. Long-term in-vitro survival of an epidemic
The cost of ozone cleaning and disinfection was i2,000
MRSA phage-group III-29 strain. J Hosp Infect 1997; 35:322-325.
(approximately $2,400). In 1997, Allen et al.9 reported the
9. Allen KD, Anson JJ, Parsons LA, Frost NG. Staff carriage of methicillin-
cost for cleaning, laundering, and replacement of furnishings
resistant Staphylococcus aureus (EMRSA 15) and the home environment:
to be approximately £2,000 (approximately $3,500).
a case report. J Hosp Infect 1997; 35:307-311.
10. Masterton RG, Coia JE, Notman AW, Kempton-Smith L, Cookson BD.
In conclusion, we describe how environmental screening
Refractory methicillin-resistant Staphylococcus aureus carriage associated
is essential for investigating refractory MRSA carriage, even
with contamination of the home environment. J Hosp Infect 1995; 29:
in the presence of a risk factor such as eczema. Furthermore,
MAY 4, 2001 VOL.27 NO.17 After The Banner Advertisers explore new ground in efforts to exploit the Net Magazine Current Issue Superstar violinist Vanessa-Mae has a new album coming out in May called Subject to Change. The title is apt, at least from a marketing standpoint, because of the innovative way studio EMI Music Asia Magazine archive is promoting the record ov
Varför de läkepedagogiska och socialterapeutiska kärnvärdena byter skepnad Många har upplevt att det finns ett behov att modernisera våra kärnvärden, förenkla vissa moment och göra texten mera tillgänglig för att komma närmare dagens språkbruk. Ett exempel bland flera, är att ersätta termen ”funktionshinder” med ”funktionsnedsättning” vilket idag är den korrekta ben
 ozone for mrsa decontamination of the home
Culture results for the nurse colonized with methicillin-resistant Staphylococcus aureus (MRSA) and control measures used,
A salvage company was asked to decontaminate the house.
ozone for mrsa decontamination of the home
Culture results for the nurse colonized with methicillin-resistant Staphylococcus aureus (MRSA) and control measures used,
A salvage company was asked to decontaminate the house.