Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Nitte.edu.in2
NUJHS Vol. 2, No.4, December 2012, ISSN 2249-7110
Nitte University Journal of Health Science
LAPAROSCOPIC ADRENALECTOMY IN PEDIATRIC PATIENTS - A REPORT OF 2 CASES. Sandeep B. Rai , Rajesh Ballal , Raghu Shankar
Professor and Head, Associate Professor, Pediatric Surgery, Professor and head, Department of Surgery,
Justice K.S. Hedge Medical College, NITTE University, Mangalore - 575 018. Raghu Shankar
Associate Professor, Pediatric Surgery, Justice K.S. Hegde charitable super speciality hospital,
Deralakatte, Mangalore - 575 018, Karnataka.
Phone : +91 824 2204471 E-mail : drraghubhat@yahoo.com
Abstract : Reporting on the laparoscopic technique for adrenal disease in children and adolescents has been limited. Laparoscopic adrenalectomy are been performed in selected patients in centers with advanced laparoscopic expertise. Here we report two cases of laparoscopic adrenalectomy done for functional adrenal tumors in pediatric patients. Keywords : Laparoscopic adrenalectomy, feminizing adrenal tumor, Cushing's adenoma. Introduction : The adrenal gland is considered suitable for laparoscopic resection because of its relatively small size and retroperitoneal location. Laparoscopic adrenalectomy (L A) has become the standard procedure for benign adrenal masses in adults. Despite multiple studies in the adults, Quick Response Code
this technique in pediatric p a t i e n t s . I n f r e q u e n t i n d i c a t i o n s f o r
adrenalectomy in children and small body habitus
pediatric patients. Also, neuroblastoma is the most
common adrenal lesion in this age group and this lesion is
LAPAROSCOPIC ADRENALECTOMY - Sandeep B. Rai
NUJHS Vol. 2, No.4, December 2012, ISSN 2249-7110
Nitte University Journal of Health Science
infiltrative and invasive in nature. As laparoscopic skills
However, the superior margin could not be defined well.
have developed in the pediatric surgical community,
Hence, keeping the possibility of malignancy, a biopsy was
laparoscopic adrenalectomies are being performed for
taken. Histopathology showed a benign adrenal tumor,
selected pediatric patients. However, this procedure is
Cushing's adenoma . And so, in the next sitting a week
been performed in centers with advanced laparoscopic
later, transperitoneal laparoscopic adrenalectomy was
expertise. We report two cases of adrenal tumors in
carried out. Recovery was uneventful. Child was started on
pediatric patients who were managed with laparoscopic
oral liquids the next day and progressed to full diet on the
subsequent day. The final histopathology revealed an intermediate grade adrenocortical tumor. Case report : Case 1 : A six year old male child was referred with Technique:
gynecomastia of six months duration. Child had been
For LA, the patient is placed in the 90° lateral decubitus
evaluated elsewhere and was receiving systemic steroids
position with the operative side up.
for the past three weeks. Examination revealed cushiongoid facies with bilateral gynecomastia. Other
A bolster is placed underneath the lumbar region and the
systemic examination findings were within normal limits.
table flexed maximally to create the largest possible
The size of the penis was normal for the age and bilateral
distance between the costal margin and the iliac crest.
testes were normal. Serum estradiol was found elevated
Ports were introduced at the sites shown in the figure 1&2.
three times the normal value, and serum cortisol level was
Adrenal vein was seen only after initial dissection of the
normal. Abdominal sonology showed a 3.5 cmx 2.6 cm
mass from lateral, inferior and superior borders using the
mass lesion in the right adrenal gland with specks of
harmonic dissector. Adrenal vein was coagulated with the
calcification. CT abdomen showed a well encapsulated
harmonic dissector blades. The remaining gland was freed
right adrenal tumor. Transperitoneal laparoscopic
by circumferential dissection. In the first case at the
adrenalectomy was done. Post –op recovery was
completion of laparoscopic dissection, the hemostasis
uneventful. As the histopathology revealed malignant
achieved was in doubt. Hence, to ensure absolute
adrenocortical feminizing tumor. Child received
hemostasis, a small subcostal incision was put which also
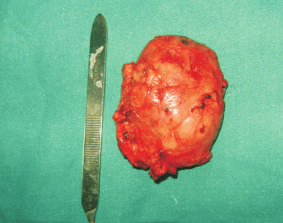
served to retrieve the specimen. Similarly, in the second case the small subcostal incision was used to deliver the
Case 2: An eleven month old male child presented with
excessive weight gain and excessive body hair. On examination, child had cushingoid features, hirsutism and
Discussion:
weighed 11 kgs . However, there were no features of
The laparoscopic approach for excision of adrenal gland
precocious puberty. Child had borderline hypertension.
was first described by Gagner et al in 1992. Laparoscopic
Systemic examination including abdominal, respiratory,
adrenalectomy has become the gold standard for removing
cardiovascular and central nervous system did not reveal
adrenal lesions of almost any pathology in adults. Despite
any abnormality. Serum cortisol levels were found to be
infrequent cases in the pediatric population, the wide
grossly elevated with the value of 36.14 microgram/dl (5.7-
applicability of laparoscopy to multiple pediatric surgeries
16.6). Random sugar was 97mg/dl; creatinine, sodium and
has enabled pediatric surgeons with necessary skill and
potassium levels of serum were normal. Contrast
equipment to perform laparoscopic adrenalectomies.
enhanced CT of the abdomen showed a well-defined
Potential benefits of laparoscopic adrenalectomy are
heterogeneously enhancing, 4.3 cmx3.7 cm soft tissue
similar to those of other minimally invasive procedures,
density lesion arising from the right adrenal. There was no
including decreased postoperative pain, shorter
evidence of local invasion. A diagnosis of Right side
hospitalization, and faster return to normal activity.
functional adrenal tumor was made. Child was taken up for
The principal approaches described for L A are the
laparoscopic adrenalectomy. The mass was noted to be of
transperitoneal and the retroperitoneal approach. The
about 6x5 cm, well encapsulated and compressing the IVC.
LAPAROSCOPIC ADRENALECTOMY - Sandeep B. Rai
NUJHS Vol. 2, No.4, December 2012, ISSN 2249-7110
Nitte University Journal of Health Science
lateral transperitoneal approach offers a more efficient
patient . The surgeon's experience also should be
working space and excellent exposure. It has been
considered in these cases. Relative contraindications
advocated by many to be the preferred approach.
include uncorrectable coagulopathy and previous trauma
in the region of spleen and kidney .
The indications for adrenal surgery differ in adults and children. Literature reveals neuroblastic tumours to be the
Conclusion:
most common adrenal lesions, requiring excision in the
Laparoscopic adrenalectomy can be performed safely and
pediatric age group. The safety and feasibility of LA for all
effectively with a short hospital stay and minimal blood loss
stages of neuroblastomas in pediatric patients (including
in pediatric patients. Patient selection for laparoscopy is
infants) has been documented in earlier studies.
crucial and is dependent on the child's body habitus, as
Although no absolute contraindications to LA has been
well as the experience of the surgical and anaesthetic
clearly identified in adults, open approach has been
teams. A low threshold for open conversion in the early
preferred in malignancies with metastatic nodes in
phase of the learning curve is recommended.
periaortic area and close to the bladder. However, in
Acknowledgment:
children, LA has even been suggested as an option for
Our sincere thanks to department of pediatrics and
residual tumours that have a favourable cytoreductive
department of anaesthesia, without whom the clinical
response to chemotherapy . Rather than stating an
course would not have been a smooth one. Also, thanking
absolute contraindicated mass size for pediatric patients,
the nursing staff of the pediatric ward.
the size of the tumor may limit the laparoscopic approach when evaluated individually relative to the size of the
Reference : 1. Gagner M, Lacorix A, Bolte E. Laparoscopic adrenalectomy in Cushing's
syndrome and pheochromocytoma. N Engl J Med 1992;327:1033.
2. Vargas HI, Kavoussi LR, Bartlett DL, Wagner JR, Venzon DJ, Fraker DL, et
al. Laparoscopic adrenalectomy: A new standard of care. Urology 1997;49:673-8.
3. Gil-Cardenas A, Cordon C, Gamino R, Rull JA, Gomez-Perez F, Pantoja
JP, et al. Laparoscopic adrenalectomy: Lessons learned from an initial series of 100 patients. Surg Endosc 2008;22: 991-4.
4. Suzuki K, Kageyama S, Hirano Y, et al: Comparison of 3 surgical
approaches to laparoscopic adrenalectomy: A nonrandomized, background matched analysis. J Urol 166:437-443, 2001
5. Miller K.A , Albanese.C, Harrison.M, Farmer.D, Ostlie D.J, Gittes G,
Holcomb G.W III. Experience with laparoscopic adrenalectomy in pediatric patients. J Pediatr Surg 2002 37:979-982.
6. Skarsgard ED, Albanese CT. The safety and efficacy of laparoscopic
adrenalectomy in children. Arch Surg 2005;140:905-8
7. Kadamba P, Habib Z, Rossi L. Experience with laparoscopic
adrenalectomy in children. J Pediatr Surg 2004;39:764-7
8. Gagner M, Pomp A, Heniford BT, et al: Laparoscopic
adrenalectomy:Lessons learned from 100 consecutive procedures. Ann Surg 226:238-247, 1997
LAPAROSCOPIC ADRENALECTOMY - Sandeep B. Rai
Donderdag 6 december 2007 Arnhem Sinds een rit in een achtbaan op 30 april voelde ik een stekende pijn onder in mijn rug vlak naast de wervelkolom onder. De pijn bleef zeuren tot 30 mei, toen ik meedeed met een voetbalpartijtje tegen de E-pupillen die ik train. Bij een verkeerde pass die ik toch probeerde aan te nemen maakte ik een beweging die ervoor zorgde dat het in mijn rug schoot. De pijn v
7. Untreated acute cervicitis or vaginitis, including bacterial vaginosis, until deliberation by a group of experts and staff of the CDC, but they should notThe uterus should sound to a depth of 6 to 9 centimeters (cm). Insertion of anShould the patient’s relationship cease to be mutually monogamous, orbe construed as rules suitable for use in all patients. Adequate PID treatmentIUD into

 NUJHS Vol. 2, No.4, December 2012, ISSN 2249-7110
Nitte University Journal of Health Science
LAPAROSCOPIC ADRENALECTOMY IN PEDIATRIC PATIENTS
NUJHS Vol. 2, No.4, December 2012, ISSN 2249-7110
Nitte University Journal of Health Science
LAPAROSCOPIC ADRENALECTOMY IN PEDIATRIC PATIENTS