Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
9515a
7. Untreated acute cervicitis or vaginitis, including bacterial vaginosis, until
deliberation by a group of experts and staff of the CDC, but they should not
The uterus should sound to a depth of 6 to 9 centimeters (cm). Insertion of an
Should the patient’s relationship cease to be mutually monogamous, or
be construed as rules suitable for use in all patients. Adequate PID treatment
IUD into a uterine cavity measuring less than 6.0 cm by sounding may increase
should her partner become HIV positive, or acquire a sexually transmitted
8. Copper-containing IUDs should not be inserted in the presence of diagnosed
requires the application of current standards of therapy prevailing at the time
the incidence of expulsion, bleeding, pain, perforation, and possibly,
disease, she should be instructed to report this change to her clinician
of occurrence of the infection with reference to the prescription labeling of the
immediately. It may be advisable to recommend the use of a barrier method
as a partial protection against acquiring sexually transmitted diseases until
Clinicians are cautioned that it is imperative for them to become thoroughly
Prescribing Information
Genital actinomycosis has been associated primarily with long-term IUD use. If
familiar with the instructions for use before attempting placement of the
the ParaGard® T 380A can be removed.
10. Patient or her partner has multiple sexual partners.
actinomycosis occurs, promptly institute appropriate antibiotic therapy and remove
ParaGard® T 380A. To reduce the possibility of insertion in the presence of an
Continuing Care of Patients Using ParaGard® T 380A Patients should be counseled that this product does not protect against HIV
11. Conditions associated with increased susceptibility to infections with micro-
existing undetermined pregnancy, the optimal time for insertion is the latter
Any inquiries regarding pain, odorous discharge, bleeding, fever, genital
infection (AIDS) and other sexually transmitted diseases.
organisms. Such conditions include, but are not limited to, leukemia, acquired
EMBEDMENT
part of the menstrual period, or one or two days thereafter. The ParaGard®
lesions or sores, or a missed period should be promptly responded to and
The ParaGard® T380A should only be inserted, managed, and removed by
immune deficiency syndrome (AIDS), and I.V. drug abuse.
T 380A should not be inserted postpartum or postabortion until involution of
clinicians that are thoroughly familiar with these procedures.
Partial penetration or embedment of the ParaGard® T 380A in the endometrium or
the uterus is complete. The incidence of perforation and expulsion is greater
myometrium can result in difficult removal. In some cases this can result in break-
If examination during visits subsequent to insertion reveals that the length
if involution is not complete. Data also suggest that there may be an increased
13. A previously inserted IUD that has not been removed.
age of the IUD, necessitating surgical removal.
of the threads has visibly or palpably changed from the length at time of
risk of perforation and expulsion if the woman is lactating.8,9 Other recent
insertion, the ParaGard® T 380A should be considered displaced and should
PERFORATION
You have received a Patient Package Insert that Federal Regulations (21 CFR
WARNINGS
studies report no increased incidence of perforation or expulsion in lactating
be removed. A new ParaGard® T 380A may be inserted at that time or
310.502) require you to furnish to each patient who is considering the use of the
Partial or total perforation of the uterine wall or cervix may occur with use of the
during the next menses if it is certain that conception has not occurred. Under
PREGNANCY
ParaGard® T 380A. The rate of perforation in randomized trials of the ParaGard®
The ParaGard® T 380A should be placed at the fundus of the uterine cavity.
no circumstances should reinsertion with an expelled ParaGard® T 380A be
Effects on the offspring when pregnancy occurs with the ParaGard® T 380A in place
T 380A has been 1 in 1,360. Insertions immediately after the expulsion of the
The Patient Package Insert contains information on the safety and efficacy of the
Proper placement enhances contraceptive effectiveness and helps avoid
attempted. A new ParaGard® T 380A should be inserted.
placenta are not known to be associated with increased risks of perforation, but
ParaGard® T 380A. Before inserting the ParaGard® T 380A:
perforation and partial or complete expulsion that could result in pregnancy.
Since the ParaGard® T 380A may be partially or completely expelled,
Septic Abortion
insertion later in the first postpartum month, particularly during lactation, has been
• You should read the physician prescription labeling and be familiar with all the
associated with an increased risk of perforation.8,9 Thus, unless performed
Patients experiencing menorrhagia and/or metrorrhagia following IUD
patients should be reexamined and evaluated shortly after the first
Reports indicate an increased incidence of septic abortion with septicemia,
immediately postpartum, insertion should be delayed to the second postpartum
insertion may be at risk for the development of hypochromic microcytic
postinsertion menses, but no later than 3 months afterwards. Thereafter, at
septic shock, and death in patients becoming pregnant with an IUD in place.
anemia. Careful consideration of this risk must be given before insertion in
least annual examination with appropriate evaluation, including a “Pap” smear,
• You should counsel the patient and answer her questions about contraception,
month. IUD insertion immediately postabortion in the first trimester is not known
Most of these reports have been associated with, but are not limited to, the
patients with anemia or a history of menorrhagia or hypermenorrhea. Patients
and if indicated, gonococcal and chlamydial laboratory evaluations, should
the ParaGard® T 380A, and the information in the Patient Package Insert.
to be associated with increased risks of perforation, but insertion after second
mid-trimester of pregnancy. In some cases, the initial symptoms have been
trimester abortion should be delayed until the second postabortion month.
receiving anticoagulants or having a coagulopathy may have a greater risk of
be carried out. The ParaGard® T 380A should be kept in place no longer than
• You and the patient should read each section of the Patient Package Insert,
insidious and not easily recognized. If pregnancy should occur with an IUD
and if the patient agrees, she may sign a consent form provided for your con-
in situ, the IUD should be removed if the string is visible and removal is easily
The possibility of perforation must be kept in mind during insertion and at the time
Syncope, bradycardia, or other neurovascular episodes may occur during
In the event a pregnancy is confirmed during ParaGard® T 380A use, the
accomplished. Of course, manipulation may result in spontaneous abortion. If
of any subsequent examination. If perforation occurs, the ParaGard® T 380A shouldbe removed as soon as possible. A surgical procedure may be required. Abdominal
insertion or removal of IUDs, especially in patients with a previous disposition
The Patient Package Insert is also available in Spanish and other foreign languages.
removal proves to be difficult, or if threads are not visible, interruption of the
adhesions, intestinal penetration, intestinal obstruction, and local inflammatory reac-
to these conditions or cervical stenosis.
• Determine whether the pregnancy is ectopic and take appropriate
Address requests to FEI Products LLC or telephone 1-800-322-4966.
pregnancy should be considered and offered as an option. Rates of mortalitywith and without contraception are shown in Table I.
tion with abscess formation and erosion of adjacent viscera may result if the ParaGard®
Use of an IUD in patients with cervicitis should be postponed until treatment
T 380A is left in the peritoneal cavity. There are reports of migration after insertion. Continuation of Pregnancy
• Inform patient of the risks of leaving an IUD in situ or removing it during
Patients with valvular or congenital heart disease are more prone to develop
If the patient elects to maintain the pregnancy and the IUD remains in situ, she
MEDICAL DIATHERMY
pregnancy, and of the lack of data on the long term effects of the ParaGard®
subacute bacterial endocarditis than patients who do not have valvular or
should be warned that there is an increased risk of spontaneous abortion and
The use of medical diathermy (short-wave and microwave) in a patient with a metal-
T 380A on the offspring of women who have had it in utero during
congenital heart disease. Use of an IUD in these patients may represent a
sepsis. In addition, she is at increased risk of premature labor and delivery. As
containing IUD may cause heat injury to the surrounding tissue. Therefore,
conception or gestation (see WARNINGS). This information should include
potential source of septic emboli. Patients with known congenital heart
a consequence of premature birth, the fetus is at increased risk of damage. She
medical diathermy to the abdominal and sacral areas should not be used on pa-
the risk of septic spontaneous abortion with the IUD in situ.
disease who may be at increased risk should be treated with appropriate
should be followed more closely than the usual obstetrical patient. The patient
tients with a ParaGard® T 380A in place.
• If possible, the ParaGard® T 380A should be removed after the patient
antibiotics at the time of insertion.
must be advised to report immediately all abnormal symptoms, such as flu-
EFFECTS OF COPPER
has been warned of the risks of removal. If removal is difficult, the patient
like syndrome, fever, abdominal cramping or pain, bleeding or vaginal discharge,
Patients requiring chronic corticosteroid therapy or insulin for diabetes should
Additional amounts of copper available to the body from the ParaGard® T 380A
should be counseled about and offered pregnancy termination.
because generalized symptoms of septicemia may be insidious.
be monitored with special care for infection.
may precipitate symptoms in women with Wilson’s disease. The incidence of
• If the ParaGard® T 380A is left in place, the patient’s course should be
ECTOPIC PREGNANCY
Wilson’s disease is approximately 1 in 200,000. The long term effects of intrauter-
Since the ParaGard® T 380A may be partially or completely expelled, patients
Patients with a history of ectopic pregnancy are at an increased risk of
ine copper to a child conceived in the presence of an IUD are unknown.
should be reexamined and evaluated shortly after the first postinsertion menses,
subsequent pregnancies being ectopic. Although current data indicate that
but no later than 3 months afterwards. Thereafter, annual examination with
ADVERSE REACTIONS RISKS OF MORTALITY
appropriate evaluation, including a “Pap” smear, should be carried out. The
DESCRIPTION
there is no increased risk of ectopic pregnancy in patients using the ParaGard®
The available data from a variety of sources have been analyzed to estimate the
These adverse reactions are not listed in any order of frequency or severity.
T 380A and some data suggest there may be a lower risk than the general
ParaGard® T 380A should be kept in place no longer than 10 years.
risk of death associated with various methods of contraception. The estimates of
Reported adverse reactions with intrauterine contraceptives include: endometritis;
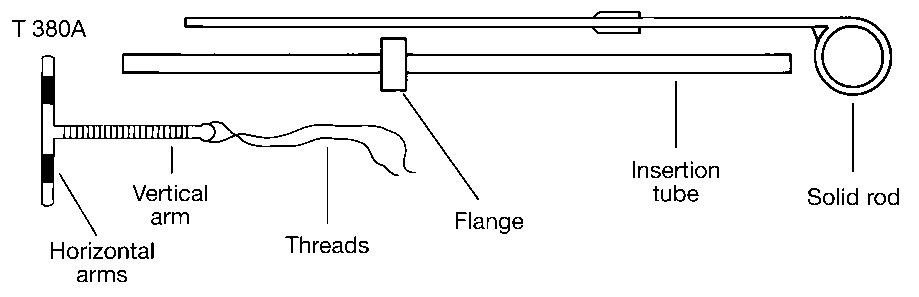
The polyethylene body of the ParaGard® T 380A is wound with approximately
population using no method of contraception, a pregnancy which occurs with
risk of death include the combined risk of the contraceptive method plus the risk
The patient should be told that some bleeding or cramps may occur during
spontaneous abortion; septic abortion; septicemia; perforation of the uterus and
176 mg of copper wire and carries a copper collar of approximately 68.7 mg of
the ParaGard® T 380A in place is more likely to be ectopic than a pregnancy
of pregnancy or abortion in the event of method failure. The findings of the analy-
the first few weeks after insertion. If these symptoms continue or are severe
cervix; embedment; fragmentation of the IUD; pelvic infection; tubo-ovarian
copper on each of its transverse arms. The exposed surface areas of copper are
occurring without ParaGard® T 380A.2-4 Therefore, patients who become
she should report them to her physician. She should be instructed on how to
abscess; tubal damage; vaginitis; leukorrhea; cervical erosion; pregnancy;
380 ± 23 mm.2 The dimensions of the ParaGard® T 380A are 36 mm in the
pregnant while using the ParaGard® T 380A should be carefully evaluated for
check to make certain that the threads still protrude from the cervix and
ectopic pregnancy; fetal damage; difficult removal; complete or partial expulsion
vertical direction and 32 mm in the horizontal direction. The tip of the vertical arm
the possibility of an ectopic pregnancy. TABLE I – Annual Number of Birth-Related or Method-Related Deaths
cautioned that there is no contraceptive protection if the ParaGard® T 380A
of the IUD, particularly in those patients with uteri measuring less than 6.0 cm
of the ParaGard® T 380A is enlarged to form a bulb having a diameter of 3 mm. Associated with Control of Fertility per 100,000 Non-Sterile Women,
Special attention should be directed to patients with delayed menses, slight
has been expelled. She should check frequently, at least after each menstrual
by sounding; menstrual spotting; prolongation of menstrual flow; anemia;
The ParaGard® T 380A is equipped with a monofilament polyethylene thread
by Fertility Control Method According to Age
metrorrhagia and/or unilateral pelvic pain, and to those patients who wish to
period. She should be cautioned not to dislodge the ParaGard® T 380A by
amenorrhea or delayed menses; pain and cramping; dysmenorrhea; backaches;
which is tied through the bulb, resulting in two threads at the tip to aid in removal
terminate a pregnancy because of IUD failure, to determine whether ectopic
Age Group
pulling on the thread. If a partial expulsion occurs, removal is indicated.
dyspareunia; neurovascular episodes, including bradycardia and syncope
of the IUD. The ParaGard® T 380A contains barium sulfate to render it radiopaque. 35-39 40-44
Rarely, a copper-induced urticarial allergic skin reaction may develop in women
secondary to insertion. Uterine perforation and IUD displacement into the abdomen
The ParaGard® T 380A is packaged together with an insertion tube and solid rod
PELVIC INFECTION (PELVIC INFLAMMATORY DISEASE, PID)
using a copper-containing IUD. If the symptoms of such an allergic response
have been followed by peritonitis, abdominal adhesions, intestinal penetration,
in a Tyvek®-polyethylene pouch and then sterilized. The insertion tube is equipped
The ParaGard® T 380A is contraindicated in the presence of PID or in women with
occur, the patient should be instructed to tell the consulting physician that a
intestinal obstruction, and cystic masses in the pelvis. (Certain of these adverse
with a movable flange to aid in gauging the depth to which the insertion tube is
a history of PID. Use of all IUDs, including the ParaGard® T 380A, has been asso-
copper-containing device is being used.
reactions can lead to loss of fertility, partial or total removal of reproductive organs,
inserted through the cervical canal and into the uterine cavity.
ciated with an increased incidence of PID. Therefore, a decision to use the ParaGard®
hormonal imbalance, or death.) Urticarial allergic skin reaction may occur.
The effect of magnetic resonance imaging of the pelvis was investigated in
T 380A must include consideration of the risks of PID. The highest rate of PID has
one study13 in women with the CU-7® (Intrauterine Copper Contraceptive) and
CLINICAL PHARMACOLOGY CLINICAL STUDIES
been reported to occur after insertion and up to four months thereafter. A study
the LIPPES LOOP™ IUD. The CU-7® has a different configuration and
Available data indicate that the contraceptive effectiveness of the ParaGard® T 380A
suggests that the highest incidence occurs within 20 days postinsertion, then falls,
contains less copper than the ParaGard® T 380A. The results of the study
Different event rates have been reported with the use of different intrauterine
is enhanced by copper being released continuously from the copper coil and
remaining constant thereafter.5 Administration of prophylactic antibiotics has been
indicate that neither the CU-7® nor the LIPPES LOOP™ were moved under
contraceptives. Inasmuch as these rates are usually derived from separate
sleeves into the uterine cavity. The exact mechanism by which metallic copper
reported, although studies do not confirm the utility of this prophylactic measure
the influence of the magnetic field nor did they heat during the spin-echo
studies conducted by different investigators in several populations, they cannot
enhances the contraceptive effect of an IUD has not been conclusively demon-
in reducing PID. PID can necessitate hysterectomy and can also lead to tubo-ovar-
sequences usually employed for pelvic imaging.
be compared with precision. Considerably different rates are likely to be obtained
strated. Various hypotheses have been advanced, including interference with sperm
ian abscesses, tubal occlusion and infertility, and tubal damage that can predis-
Insertion Prophylaxis
because event rates per unit of time tend to decrease as studies are extended,
transport, fertilization, and implantation. Clinical studies with copper-bearing
pose to ectopic pregnancy. PID can result in peritonitis and, infrequently, in death.
Observe strict asepsis at insertion; clean the endocervix with an antiseptic solu-
since more susceptible subjects discontinue due to expulsions, adverse
IUDs also suggest that fertilization is prevented either due to an altered number
The effect of PID on fertility is especially important for women who may wish to
tion, because the presence of organisms capable of establishing PID cannot be
reactions, or pregnancy, leaving the study population richer in less susceptible
determined by appearance, and because IUD insertion may be associated with
subjects. In clinical trials conducted by The Population Council14,15 and WHO,
Women at special risk of PID
introduction of vaginal bacteria into the uterus. Data do not confirm the utility of
use-effectiveness of the ParaGard® T 380A as calculated by the life table method
INDICATIONS AND USAGE
was determined through ten (10) years of use.
The risk of PID appears to be greater for women who have multiple sexual
prophylactic administration of antibiotics in reducing the incidence of PID, and their
The ParaGard® T 380A is indicated for intrauterine contraception. ParaGard®
partners and also for those women whose sexual partners have multiple sex-
PRECAUTIONS
use in nursing women is not recommended.
Data suggest a higher pregnancy rate in women under 20.14,15,17
T 380A is highly effective. Table II and Table III list an expected pregnancy rate
ual partners, as PID is most frequently caused by sexually transmitted dis-
Requirements for Continuation and Removal
for one year between 0.7 and 0.5, respectively. ParaGard® T 380A should not be
Patients should be counseled that this product does not protect against HIV
The ParaGard® T 380A must be replaced before the end of the tenth year of
infection (AIDS) and other sexually transmitted diseases. PID warning to ParaGard® T 380A users
use. There is no evidence of decreasing contraceptive efficacy with time before
All women who choose the ParaGard® T 380A must be informed prior to
Patient Counseling
ten years, but the contraceptive effectiveness at longer times has not been
RECOMMENDED PATIENT PROFILE
insertion that IUD use has been associated with an increased incidence of PID
Prior to the insertion, the physician, nurse, or other trained health professional must
established; therefore, the patient should be informed of the known duration
The ParaGard® T 380A is recommended for women who have had at least one
and that PID can necessitate hysterectomy, can cause tubal damage leading
provide the patient with the Patient Package Insert. The patient should be given
of contraceptive efficacy and be advised to return in 10 years for removal and
child, are in a stable, mutually monogamous relationship, and have no history of
to ectopic pregnancy or infertility or, in infrequent cases, can cause death.
the opportunity to read the information and discuss fully any questions she may
possible insertion of a new ParaGard® T 380A.
Patients must be taught to recognize and report to their physician promptly
have concerning the ParaGard® T 380A as well as other methods of contraception.
The ParaGard® T 380A should be removed for the following medical reasons:
any symptoms of pelvic inflammatory disease. These symptoms include de-
Patient Evaluation and Clinical Considerations
menorrhagia- and/or metrorrhagia-producing anemia; pelvic infection; genital
CONTRAINDICATIONS
velopment of menstrual disorders (prolonged or heavy bleeding), unusual
A complete medical and social history, including that of the partner, should be
actinomycosis; intractable pelvic pain; dyspareunia; pregnancy, endometrial
vaginal discharge, abdominal or pelvic pain or tenderness, dyspareunia, chills,
obtained to determine conditions that might influence the selection of an IUD.
or cervical malignancy; uterine or cervical perforation; increase in length of the
The ParaGard® T 380A should not be inserted when one or more of the follow-
A physical examination should include a pelvic examination, a “Pap” smear,
threads extending from the cervix, or any other indication of partial expulsion. Asymptomatic PID
and appropriate tests for any other forms of genital disease, such as gonor-
Insertions immediately following placental delivery or first trimester abortion
1. Pregnancy or suspicion of pregnancy.
may result in threads becoming slightly longer as the uterus involutes and may
PID may be asymptomatic but still result in tubal damage and its sequelae.6,7
rhea and chlamydia laboratory evaluations, if indicated. If actinomyces-like
2. Abnormalities of the uterus resulting in distortion of the uterine cavity.
organisms are detected on the Pap smear, they should be cultured to deter-
not represent expulsion or partial expulsion. Treatment of PID
3. Acute pelvic inflammatory disease or a history of pelvic inflammatory
mine whether genital actinomyces is present. The physician should determine
If the retrieval threads cannot be visualized, they may have retracted into the
Following diagnosis of PID, or suspected PID, bacteriologic specimens should
uterus or have been broken, or the ParaGard® T 380A may have been broken,
be obtained and antibiotic therapy should be initiated promptly. Removal of
4. Postpartum endometritis or infected abortion in the past 3 months.
The uterus should be carefully sounded prior to the insertion to determine the
or the ParaGard® T 380A may have been expelled. Localization may be made
the ParaGard® T 380A after initiation of antibiotic therapy is usually appropri-
degree of patency of the endocervical canal and the internal os, and the
by feeling with a probe, X-ray, or sonography. When the physician elects to
5. Known or suspected uterine or cervical malignancy, including unresolved,
ate. Time should be allowed for therapeutic blood levels to be reached prior
direction and depth of the uterine cavity. In occasional cases, severe cervical
recover a ParaGard® T 380A with the threads not visible, the removal
to removal. Guidelines for PID treatment are available from the Center for
stenosis may be encountered. Do not use excessive force to overcome this
6. Genital bleeding of unknown etiology.
Disease Control (CDC), Atlanta, Georgia. The guidelines were established after
TABLE II ParaGard® T 380A Footnotes to Table IV: HOW TO LOAD AND INSERT ParaGard® T 380A REFERENCES (Intrauterine Copper Contraceptive)
1. Among typical couples who initiate use of a method (not necessarily for the first
After the arms are released, the insertion tube should be moved upward gently,
time), the percentage who experience an accidental pregnancy during the first
1. Alvarez F et al: New insights on the mode of action on intrauterine contraceptives
To minimize the chance of introducing contamination, do not remove the ParaGard®
until the resistance of the fundus is felt. This will assure placement of the T at the
year if they do not stop use for any other reason.
in women. Fertil Steril 1988; 49:768-773.
T 380A from the insertion tube prior to placement in the uterus. Do not bend the
highest possible position within the endometrial cavity (Fig. 4). GROSS ANNUAL TERMINATION AND CONTINUATION RATES
2. Among couples who initiate use of a method (not necessarily for the first time)
2. World Health Organization’s Special Programme of Research, Development and
arms of the ParaGard® T 380A earlier than 5 minutes before it is to be introduced
PER 100* USERS
and who use it perfectly (both consistently and correctly), the percentage who
Research Training in Human Reproduction: A multinational case-control study of
All Copper T 380A IUD Acceptors
experience an accidental pregnancy during the first year if they do not stop use
ectopic pregnancy. Clin Reprod Fertil 1985; 3:131-143. Combined Population Council and WHO Studies
In the absence of sterile gloves, this can be accomplished without destroying
3. Ory HW, Women’s Health Study: Ectopic pregnancy and intrauterine contracep-
3. Among couples attempting to avoid pregnancy, the percentage who continue to
sterility by folding the arms in the partially opened package. Place the partially opened
tive devices: New perspectives. Obstet Gynecol 1981; 57:137-144.
package on a flat surface and pull the solid rod partially from the package so it will
4. Marchbanks PA et al: Risk factors for ectopic pregnancy: A population-based
4. The percentages failing in columns (2) and (3) are based on data from popula-
not interfere with assembly. Place thumb and index finger on top of package on
study. JAMA 1988; 259:1823-1827.
tions where contraception is not used and from women who cease using contra-
ends of the horizontal arms. Push insertion tube against arms of ParaGard® T 380A
5. Farley TMM et al: Intrauterine devices and pelvic inflammatory disease: An in-
ception in order to become pregnant. Among such populations, about 89% become
as indicated by arrow in Fig. 1A to start arms folding.
ternational perspective. Lancet 1992; 339:785-788.
pregnant within one year. This estimate was lowered slightly (to 85%) to represent
6. Cramer DW et al: Tubal infertility and the intrauterine device. N Engl J Med 1985;
the percentage who would become pregnant within 1 year among women now
relying on reversible methods of contraception if they abandoned contraception
7. Daling JR et al: Primary tubal infertility in relation to the use of an intrauterine de-
vice. N Engl J Med 1985; 312:937-941.
5. Foams, creams, gels, vaginal suppositories, and vaginal film.
8. Heartwell SF, Schlesselman S: Risk of uterine perforation among users of intra-
6. Cervical mucous (ovulation) method supplemented by calendar in the pre-
uterine devices. Obstet Gynecol 1983; 61:31-36.
ovulatory and basal body temperature in the post-ovulatory phases.
9. Chi I-C, Kelly E: Is lactation a risk factor of IUD and sterilization-related uterine
perforations? A hypothesis. Int J Gynaecol Obstet 1984; 22:315-317.
10. Harlap S, Kost K, Forrest JD: Preventing pregnancy, protecting health: a new look at
9. The treatment schedule is one dose as soon as possible (but no more than
birth control choices in the United States. The Alan Guttmacher Institute 1991; 1-129.
*Rates were calculated by weighing the annual rates by the number of subjects
72 hours) after unprotected intercourse, and a second dose 12 hours after the
11. Chi I-C et al: Performance of the Copper T 380A Intrauterine device in breast
starting each year for each of the Population Council (3536 acceptors) and the
first dose. The hormones that have been studied in the clinical trials of postcoital
feeding women. Contraception 1989; 39:603-618.
World Health Organization (1396 acceptors) trials.
hormonal contraception are found in Nordette, Levlen, Lo/Ovral (1 dose is
12. Farr G, Rivera R: Interactions between intrauterine contraceptive device use and
4 pills), Triphasil, Tri-Levlen (1 dose is 4 yellow pills), and Ovral (1 dose is 2 pills).
Withdraw the solid rod while holding the insertion tube stationary (Fig. 5).
breast-feeding status at time of intrauterine contraceptive device insertion. Analysis
10. However, to maintain effective protection against pregnancy, another method of
of TCu-380A acceptors in developing countries. Am J Obstet Gynecol 1992;
TABLE III
contraception must be used as soon as menstruation resumes, the frequency or
Complete the bending by bringing the thumb and index finger together using the
GROSS ANNUAL EVENT RATES PER 100 CONTINUING USERS
duration of breastfeeds is reduced, bottle feeds are introduced, or the baby
13. Mark AS, Hricak H: Intrauterine contraceptive devices: MR imaging. Radiology
other hand to maneuver the insertion tube to pick up the arms of the ParaGard®
BY YEAR AND PARITY
T 380A (Fig. 1B). Insert no further than necessary to insure retention of the arms.
14. Sivin I, Stern J: Long-acting, more effective Copper T IUDs: A summary of US
Introduce the solid rod into the insertion tube from the bottom alongside the threads
HOW SUPPLIED
experience, 1970-1975. Stud Fam Plann 1979; 10:263-281.
until it touches the bottom of the ParaGard® T 380A.
15. Sivin I, Schmidt F: Effectiveness of IUDs: A review. Contraception 1987; 36:55-84.
Available in cartons of one (NDC 50907-0380-6) or five (NDC 50907-0380-7)
16. Trussell J: The Essentials of Contraception, in R.A. Hatcher, et al: Contraceptive
sterile units. Each ParaGard® T 380A is packaged in a Tyvek®-polyethylene pouch,
Technology, 16th Revised Ed., New York, Irvington, 1994, p. 113-114.
together with an insertion tube and solid rod.
17. World Health Organization (WHO): Mechanism of action, safety, and efficacy of
intrauterine devices. Report of a WHO Scientific Group. Technical Report Series
753. Geneva; World Health Organization, 1987, p. 22. INSTRUCTIONS FOR USE
Rates were calculated by combining the experience on a weighted basis from
ParaGard® T 380A
both an international study by the World Health Organization (2110 women) and
(Intrauterine Copper Contraceptive)
a U.S. study by GynoPharma Inc. (230 women).
The lowest expected and typical failure rates during the first year of continuous
CLINICIANS SHOULD BE THOROUGHLY FAMILIAR WITH PARAGARD®
use of all contraceptive methods are listed in Table IV (Adapted from
T 380A INSERTIONS, MANAGEMENT, AND REMOVAL PROCEDURES. PREVIOUS EDUCATION RE: SURGICAL PROCEDURES WILL REQUIRE
Withdraw the insertion tube from the cervix. Be sure sufficient length of the threads
VARYING LEVELS OF EXPERIENCE.
Adjust the movable flange so that it indicates the depth to which the
are visible (approximately 1 in. or 2.5 cm.) to facilitate checking for the presence
TABLE IV - Percentage of women experiencing a contraceptive failure dur-
The ParaGard® T 380A (Intrauterine Copper Contraceptive) represents a different
ParaGard® T 380A should be inserted and the direction in which the arms of the
of the ParaGard® T 380A (Fig. 6). Notation of length of the threads should be made
ing the first year of typical use and the first year of perfect use
design in intrauterine contraceptives. Physicians are, therefore, cautioned that they
ParaGard® T 380A will open. At this point, make certain that the horizontal arms of
and the percentage continuing use at the end of the first year,
should become thoroughly familiar with instructions for insertion before attempt-
the ParaGard® T 380A and the long axis of the flange lie in the same horizontal
United States.16
ing placement of the ParaGard® T 380A. The insertion technique is different in
plane. Introduce the loaded insertion tube through the cervical canal and upwards
several respects from that employed with other intrauterine contraceptives and the
until the ParaGard® T 380A lies in contact with the fundus. The movable flange
% of Women Experiencing an % of Women
physician should pay particular attention to the drawings and commentary
Accidental Pregnancy Within the Continuing Use at First Year of Use One Year3
A single ParaGard® T 380A is placed at the fundus of the uterine cavity. Typical Use1 Perfect Use2
The ParaGard® T 380A may be inserted at any time during the cycle. However, it
is essential that pregnancy be ruled out before insertion.
The ParaGard® T 380A is indicated for use up to 10 years. Therefore, the ParaGard®
T 380A must be removed and a new one inserted on or before 10 years from the
PRELIMINARY PREPARATION AND INSERTION
Before insertion, you and the patient will want to review the Patient Package
Insert. If the patient agrees, she may sign the Consent Form provided for your
Refer to CONTRAINDICATIONS, WARNINGS, and PRECAUTIONS.
Pelvic examination is to be performed prior to insertion of the ParaGard®
HOW TO REMOVE ParaGard® T 380A
T 380A, including a cervical “Pap” smear, and gonococcal and chlamydial
evaluations, if indicated, and any other necessary specific tests.
To remove the ParaGard® T 380A, pull gently on the exposed threads. The arms of
If appropriate, commence antibiotic prophylaxis one hour before insertion.
the ParaGard® T 380A will fold upwards as it is withdrawn from the uterus. Even if
removal proves difficult, the ParaGard® T 380A should not remain in the uterus after
Use of aseptic technique during insertion is essential.
To release the arms of the ParaGard® T 380A, withdraw the insertion tube not more
2 inch while the solid rod is not permitted to move. This releases the arms of
The endocervix should be cleansed with an antiseptic solution and a tenacu-
lum applied to the cervix with downward traction for correction of the
angulation as well as stabilization of the cervix.
With a speculum in place, gently insert a sterile sound to determine the depth
and direction of the uterine canal. Be sure to determine the position of the
Any intrauterine procedure can result in severe pain, bradycardia, and syncope.
It is generally believed that perforations, if they occur, are encountered at the time
Emergency Contraceptive Pills: Treatment initiated within 72 hours after
of insertion, although the perforation may not be detected until some time later.
unprotected intercourse reduces the risk of pregnancy by at least 75%.9
The position of the uterus should be determined during the preinsertion exam-ination. Great care must be exercised during the preinsertion sounding and
Lactational Amenorrhea Method: LAM is a highly effective temporary method of
subsequent insertion. No attempt should be made to force the insertion.
Manufactured by FEI Products LLCN. Tonawanda, New York 14120
Dallmayr in München gilt als der Inbegriff für Genuss. Es ist das Stamm-haus veredelter Spitzenkaffees und der Treffpunkt von Gourmets aus aller Welt. Das Unternehmen wird mit viel Liebe zum Detail, Respekt vor dem Fachwissen der Mitarbeiter und Stolz auf eine lebendige Tradition geführt. Qualität und Service erster Klasse sind hier Berufung und Passion – jeden Tag. Es geht bei Dallmayr nich
CHECKLIST OF REQUIREMENTS FOR DRUG DISTRIBUTOR / MANUFACTURER; MEDICAL DEVICE; COSMETIC ESTABLISHMENTS General Requirements: (ALL FORMS TO BE ACCOMPLISHED IN TRIPLICATE) _________ Information as to activity of the establishment _________ Notarized Accomplished Petition Form / Joint Affidavit of Undertaking _________ Photocopy of Business Name Registration with DTI (if single proprietor); with SEC
 7. Untreated acute cervicitis or vaginitis, including bacterial vaginosis, until
deliberation by a group of experts and staff of the CDC, but they should not
The uterus should sound to a depth of 6 to 9 centimeters (cm). Insertion of an
Should the patient’s relationship cease to be mutually monogamous, or
be construed as rules suitable for use in all patients. Adequate PID treatment
IUD into a uterine cavity measuring less than 6.0 cm by sounding may increase
should her partner become HIV positive, or acquire a sexually transmitted
8. Copper-containing IUDs should not be inserted in the presence of diagnosed
requires the application of current standards of therapy prevailing at the time
the incidence of expulsion, bleeding, pain, perforation, and possibly,
disease, she should be instructed to report this change to her clinician
of occurrence of the infection with reference to the prescription labeling of the
immediately. It may be advisable to recommend the use of a barrier method
as a partial protection against acquiring sexually transmitted diseases until
Clinicians are cautioned that it is imperative for them to become thoroughly
Prescribing Information
7. Untreated acute cervicitis or vaginitis, including bacterial vaginosis, until
deliberation by a group of experts and staff of the CDC, but they should not
The uterus should sound to a depth of 6 to 9 centimeters (cm). Insertion of an
Should the patient’s relationship cease to be mutually monogamous, or
be construed as rules suitable for use in all patients. Adequate PID treatment
IUD into a uterine cavity measuring less than 6.0 cm by sounding may increase
should her partner become HIV positive, or acquire a sexually transmitted
8. Copper-containing IUDs should not be inserted in the presence of diagnosed
requires the application of current standards of therapy prevailing at the time
the incidence of expulsion, bleeding, pain, perforation, and possibly,
disease, she should be instructed to report this change to her clinician
of occurrence of the infection with reference to the prescription labeling of the
immediately. It may be advisable to recommend the use of a barrier method
as a partial protection against acquiring sexually transmitted diseases until
Clinicians are cautioned that it is imperative for them to become thoroughly
Prescribing Information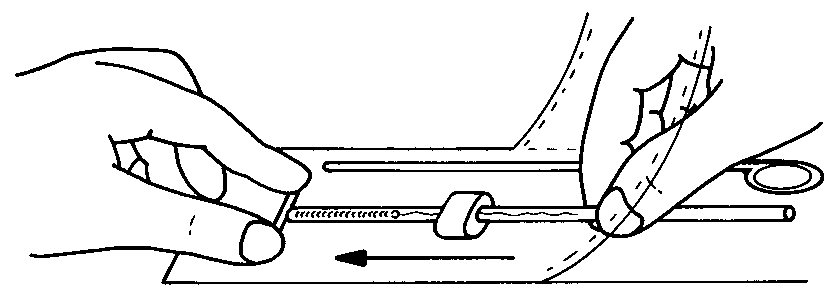
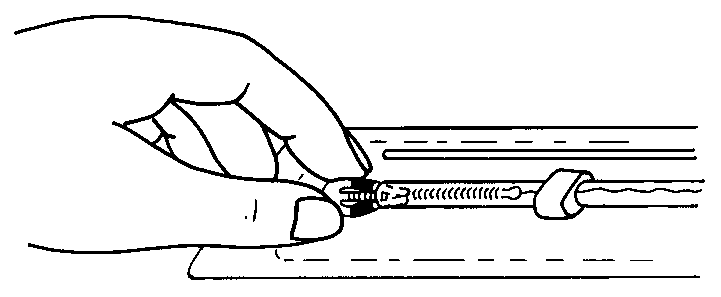
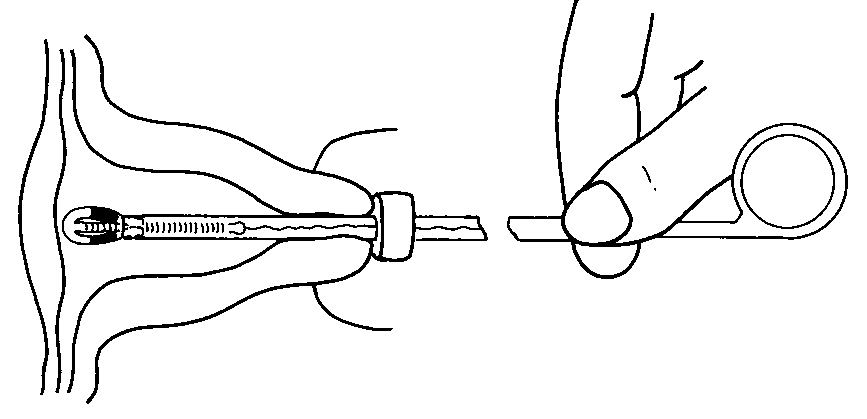
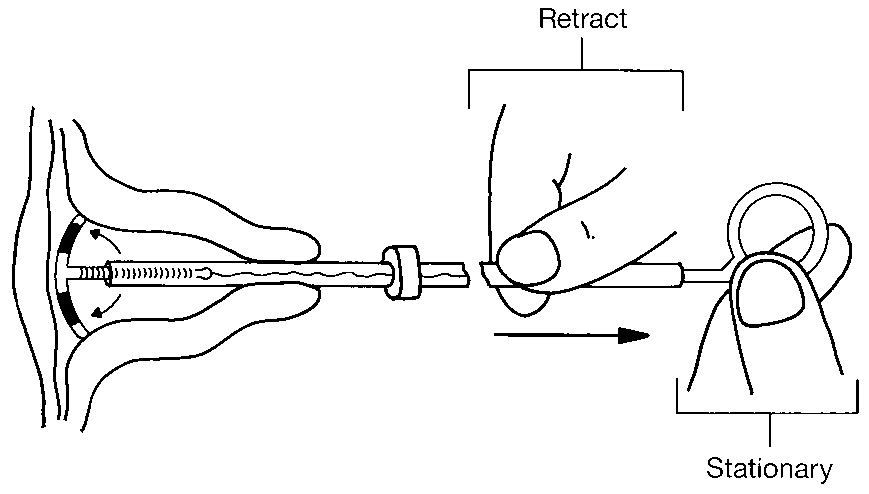
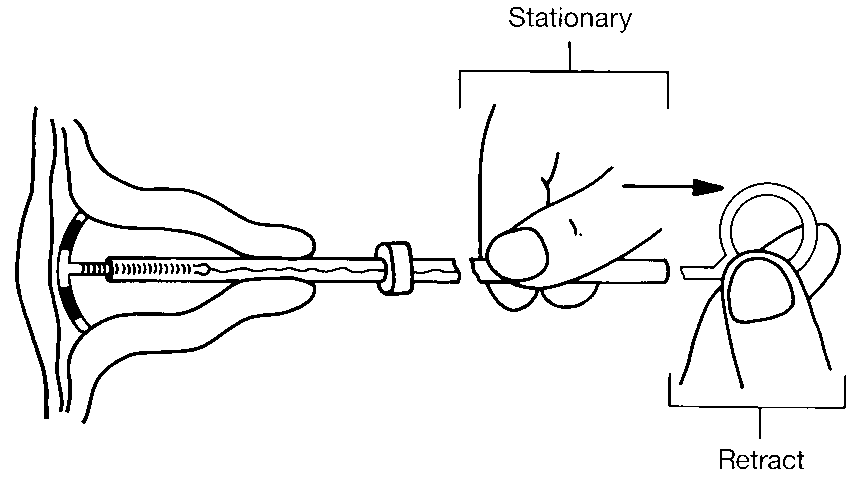
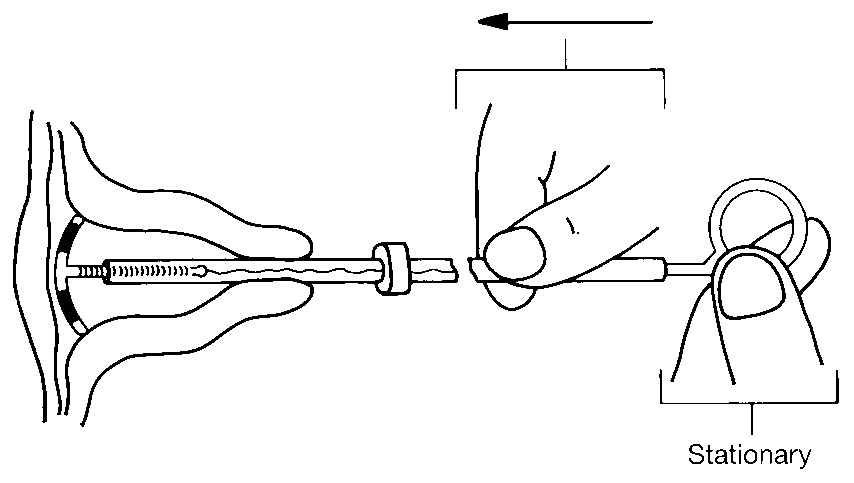
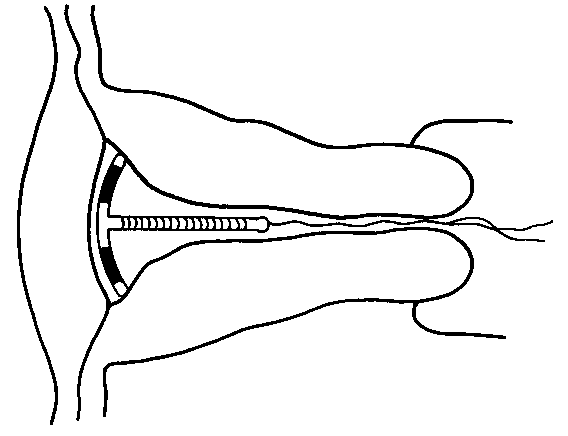 TABLE II ParaGard® T 380A
TABLE II ParaGard® T 380A