Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Linus101.li.funpic.de
Genes and Immunity (2006) 00, 1–4& 2006 Nature Publishing Group All rights reserved 1466-4879/06 $30.00
SHORT COMMUNICATIONThe interleukin-10 gene promoter polymorphismÀ1087AG does not correlate with clinical outcome in non-Hodgkin’s lymphoma
D Kube1, T-D Hua1, M Klo¨ss2, B Kulle3,4, J Brockmo¨ller5, L Wojnowski5,6, M Lo¨ffler2, M Pfreundschuh7and L Tru¨mper11Department of Internal Medicine Hematology and Oncology, Georg-August Universita¨t Go¨ttingen, Mainz, Germany; 2University ofLeipzig, Mainz, Germany; 3Institute of Epidemiology, Mainz, Germany; 4Section of Statistics, Institute of Basic Medical Science,University of Oslo, Oslo, Norway; 5Department of Pharmacology and Toxicology, Mainz, Germany; 6University Mainz, Institute ofPharmacology, Mainz, Germany and 7Department of Internal Medicine I, Saarland University, Homburg/Saar for the DSHNHL(German High Grade NHL Study Group), Mainz, Germany
The Interleukin 10 (IL-10) gene is highly polymorphic, and the IL-10À
(rs1800896) gene variation is the only so far studied
intensively in association with certain diseases. Conflicting data have been published about an association of IL-10À
variation with lower rates of complete remission and lower overall survival (OS) in patients with diffuse large B-cell lymphoma. To further investigate this in malignant lymphoma, we established the IL-10 genotypes in patients from the NHL-B1/ B2 studiesfrom the German High-Grade Non-Hodgkin’s Lymphoma Study Group. In our study, allele frequencies of lymphoma patientsare comparable as in healthy controls. No increase of IL-10
alleles was found. In addition we did not find any difference in
OS or event-free survival between patients with IL-10
and the other genotypes. Comparable results were obtained for the
IL-10 loci at À3538 (A/T), À1354 (A/G), À824 (C/T) and À597 (A/C) (rs1800890, rs1800893, rs1800871 and rs1800872). Genes and Immunity (2006) 0, 000–000. doi:10.1038/sj.gene.6364364
With conventional chemotherapy, long-term remission
Interleukin 10 (IL-10) is an important immunoregula-
can be achieved in approximately 50% of patients with
tory cytokine in man and is part of a balanced network of
disseminated ‘aggressive’ lymphoma. The disease in-
immunoregulatory factors, where it also stimulates
cidence is increasing, but aetiologic factors contributing
proliferation of certain B-cell malignancies or suppresses
to this phenomenon remain still largely unknown.
the immune response against lymphomas.1 IL-10 is
Although it is a curable disease, many patients do not
produced by a number of cells including normal and
achieve complete remission (CR), or they relapse after
neoplastic B cells, stimulated monocytes/macrophages
conventional chemotherapy. Tumour- and host-related
and subsets of T cells. IL-10 has been implicated in
parameters are likely to reflect some underlying biologic
certain infectious diseases, autoimmunity, transplanta-
mechanisms and differences in the response to therapy
tion tolerance and tumorigenesis.2–15 Polymorphisms in
may be related to genetic factors of the host.
the IL-10 50-flanking region genetically affect inter-
One suggestion is that deregulated components of the
individual differences in IL-10 production.16–21 Increased
immune system may be linked to the incidence and
IL-10 plasma levels and poor outcome of some lympho-
clinical course of lymphomas. Cytokines are major
ma entities have been shown, suggesting an role for IL-10
mediators of inflammation and deregulated expression
of defined subsets of cytokines was found to be
Recently Lech-Maranda and co-workers reported that
associated with lymphoid malignancies. Therefore, at-
homozygocity for À1087A (rs1800896 A/G) of the IL-10
tempts to clarify the mechanisms involved in immune
promoter is associated with lower rates of complete
UNCORRECTED PROOF
deregulation in lymphoma should contribute to a
remission and lower overall survival (OS) in patients
better understanding of the clinical course of these
with diffuse large B-cell lymphoma (DLBCL), whereas
Berglund and co-workers showed an absence of such anassociation.22,23 In a recent epidemiological multicenterstudy, evidence was provided that for carriers of the IL-
Correspondence: D Kube, Georg-August Universita¨t Go¨ttingen,
10À3538A allele (rs1800890 A/T) the risk of NHL is
Department of Internal Medicine Hematology and Oncology,
doubled, but this was not verified by a follow-up
To further investigate IL-10 promoter gene variations
Received 8 August 2006; revised 30 October 2006; accepted 31October 2006
in malignant lymphoma, we established the IL-10À1087
Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
genotype, in comparison to IL-10À3538, IL-10À1354, IL-
All patients included in this study received anthracy-
10À824 and IL-10À597 genotypes (rs 1800893, 1800871 and
cline-containing regimens, consisting of CHOP/CHOEP
1800872, respectively) in patients from the NHL-B1/ B2
(cyclophosphamide, adriamycin, vincristine, etoposide,
studies from the German High-Grade Non-Hodgkin’s
prednisone).26,27 Complete remission (CR) was defined as
Lymphoma Study Group (DSHNHL) and compared it
the disappearance of all disease manifestations for at
with OS and event-free survival (EFS).26,27 We used for
least 2 months after the final restaging. EFS was
this analysis a homogeneous, equally treated cohort of
determined from the onset of treatment until either
patients with non-Hodgkin’s Lymphoma (NHL). Pa-
disease progression, initiation of salvage therapy; or
tients were eligible if they had previously untreated,
additional (off-protocol) treatment, relapse, death or in
biopsy-confirmed, aggressive NHL according to the
case of no event OS was determined from the onset of
Revised European-American Lymphoma Classification
treatment until the last follow-up evaluation or death
(translated into the World Health Organization (WHO)
from any cause. Within 5 years the OS was 60.2% (95%
classification). Patients were excluded if the diagnosis of
confidence interval: 54.8:65.5) for all and 61.8% (95%
aggressive lymphoma was not confirmed (i.e., no
confidence interval: 55.3:68.3) for the DLBCL subgroup.
pathology review was available) or if the diagnosis had
The EFS was respectively 49.4% (95% confidence inter-
to be changed into indolent lymphoma or no lymphoma
val: 44.1:54.8) and 49.7 (95% confidence interval:
at all by a panel of expert hematopathologists who
43.0:56.4). Further clinical characteristics of the patients
conducted a blinded central pathology review. The
enrolled in the study are described in detail in
patients had mandatory baseline examinations that
Pfreundschuh et al.26,27 and Wojnowski et al.28
included clinical examination, laboratory tests, chest
We also assessed the allele frequencies in 193 ethni-
radiograph, abdominal sonography, computed tomogra-
cally matched healthy controls. The frequency of IL-10–
phy of chest and abdomen, and a bone marrow biopsy.
alleles and corresponding genotypes were not
significant different between patients and controls(0.285 vs 0.271% for À1087AA; P ¼ 0.516). The same
Genotype frequency of the IL10 promoter gene variation
was found when only DLBCL-patients were analysed
at À1087 in 409 NHL patients (including 256 patients with DLBCL)
(0.285 vs 0.305%; P ¼ 0.344) (see also Table 1). The
frequency of IL-10À1354, IL-10À824 and IL-10 IL-10À597
alleles and corresponding genotypes were not significantdifferent between patients and controls (P ¼ 0.273, 0.855
or 0.543, respectively) (Table 2). Analysing the IL-10À3538gene variation significant differences between healthy
controls and lymphoma patients can be visualized:
genotype and allele based analysis showed P-values of
0.008 and 0.015, respectively, suggesting a risk for
aggressive NHL for carriers of the A-allele as described
by Rothman et al.24 Using Fishers exact test the odds ratiois 1.62 (confidence interval: 1.12;2.38). However perform-
Abbreviations: DLBCL, diffuse large B-cell lymphoma; IL-10,
ing multivariate testing (Bonferoni, FDR-method) these
interleukin 10; NHL, non-Hodgkin’s lymphoma.
differences at IL-10À3538 were not longer significant. For
Analysis of the IL-10 gene variation was performed as described in
the DLBCL subgroup no significant differences for the
Mo¨rmann et al. or using an TaqMan-assay for the IL-10À1087 gene
analysed IL-10 loci were found. Overall our data did not
snp.cfm?both_snp_id ¼ IL10-03.21,26,27 Sixty-seven percent of the
show differences in allele frequencies between lympho-
patients were older than 60 years (median 64; range 23–75), whereas
in the DLBCL subgroup (n ¼ 256) 69% were older than 60 years
Thus, in our study allele frequencies of lymphoma
patients are comparable as in healthy controls. No
Genotype frequency of the IL10 promoter gene variations at À3538, À1354, À824 and À597 in NHL and control subjects
UNCORRECTED PROOF
Abbreviations: IL-10, interleukin 10; NHL, non-Hodgkin’s lymphoma. Analysis of the IL-10 gene variation was performed as described in Mo¨rmann et al.21 pCAT: P-value using the Freidlin test (genotype basedassociation); Chi allele: P-value of the respective allele-based comparison; PCHI: P-values when comparing one genotype against the otherstogether; 11 represents the minor genotype, 12 the respective heterozygous genotype and 22 the major genotype; N – number of individuals. Genes and Immunity
Interleukin-10, polymorphism, non-Hodgkin’s lymphomaD Kube et al
OS for the 409 patients with NHL in comparison to the IL-10 –1087 genotype. Inset presents the same data for the DLBCL group
increase of IL-10–1087G alleles was found. In addition, we
producer haplotype.16,18–21 The mechanism behind this
did not find any difference in OS (all P ¼ 0.704, DLBC
is still unkown, probably because of the close proximity
P ¼ 0.892) or EFS (all P ¼ 0.822, DLBC 0.86) between
of À1087AG to the IL-10.G microsatellite. The IL-10.R
patients with IL-10–1087AA genotype and the other
microsatellite in close proximity of À3538AT may also
genotypes, calculated in different ways as presented by
affect IL-10 expression levels. First reports on structural
Lech-Maranda et al. or Berglund et al. (Figure 1). No
changes of the chromatin within the IL10 gene in
significant differences in the clinical presentation were
differentiated Th1 and Th2 cells or macrophages empha-
detected between the genotype groups compared when
size the surprising diversity of mechanisms used to
sex, the factors of international prognostic index (IPI)
regulate cytokine gene expression at the chromatin level
(age460, LDH4N, ECOG41, stage III/IV, extranodal
and might be opening the chance to understand the
involvement 41) or the IPI score were taken into
mechanism of interindividual differences in IL-10 ex-
consideration. There were no differences according to
pression.29–34 DNase I-hypersensitive sites on a con-
the complete remission rate between the genotype
served 40-kb region between the IL-19 and IL-10 genes in
groups. No associations were found between the prog-
different murine T-cell populations revealed three
nostic variables, EFS, or OS intervals and alleles/
enhancer elements, which function in T cells in vitro.35
genotypes for the other analysed gene loci (OS: À3538
The role of inherited factors in the extend of IL-10
deregulation in malignant disorders is still controversy.
P ¼ 0.294; EFS: À3538 P ¼ 0.521; À1354 P ¼ 0.695; À824
The data obtained so far indicate that additional,
probably larger studies are required, also in order to
In our study, 67.0% of all patients were older than 60
confirm initial results. This will significantly contribute
years with a range between 23 and 75 years (69.5% 460
to the understanding of the role of IL-10 in lymphoma
years within the DLBCL-group). IPI low low intermedi-
development. Some studies revealed that the IL-10
ate, CS III/IV, extranodal sites, bulky disease and B
promoter region was associated with a poor prognosis
symptoms were comparable in our cohort to those
of aggressive NHL. However, as in our study in the
described by Lech-Maranda et al., percentage of LDH4N
majority of single SNP analysis this effect is not. This
was lower in our group. In addition after adjusting the
may suggest that additional not yet identified gene
analysis for the prognostic factors from the IPI no
variations within the chromosomal region 1q31/32
significant differences between the genotype groups
around the IL-10 gene are important for our under-
standing of the role of inherited factors in lymphomas. In
At this stage the precise role of IL-10 promoter gene
addition it is relevant to analyse the relation of respective
UNCORRECTED PROOF
variations, both individually or as part of defined
gene variations in this chromosomal area to intergenic
proximal or distal haplotypes in determining IL-10
RNAs and their role in regulating the expression of IL-10
expression is still a subject awaiting answers. The IL-10
family members 35. Follow-up analysis will need to
gene is highly polymorphic, and the IL-10À1087 gene
analyse additional gene variations across 1q31/32 and
variation is the most intensively studied variation in this
other immunological important cytokines as suggested
cytokine gene promoter. Furthermore in most studies
published so far the SNPs –1087, À824 and –597 or theso-called proximal haplotypes GCC/ATA/ACC werefound to be related to the IL-10 production capacity invitro, where GCC was described as an IL-10 high
Genes and Immunity
Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
19 Eskdale J, Gallagher G, Verweij C et al. Interleukin 10 secretion
in relation to human IL-10 locus haplotypes. Proc Natl Acad Sci
The authors are gratefull to the Deutsche Forschnugsge-
meinschaft (Graduiertenkolleg 1034), the BMBF (NGFN-
20 Crawley E, Kay R, Sillibourne J et al. Polymorphic haplotypes
1) and the Deutsche Krebshilfe/BMBF (NHL-B) for
of the IL-10 50 flanking region determine variable IL-10
transcription and are associated with particular phenotypesof juvenile rheumatoid arthritis. Arthr Rheum 1999; 42: 1101–1108.
21 Mormann M, Rieth H, Hua TD et al. Mosaics of gene
variations in the Interleukin-10 gene promoter affect inter-leukin-10 production depending on the stimulation used.
1 Moore KW, de Waal Malefyt R, Coffman RL et al. Interleukin-
10 and the interleukin-10 receptor. Annu Rev Immunol 2001; 19:
22 Lech-Maranda E, Baseggio L, Bienvenu J et al. Interleukin-10
gene promoter polymorphisms influence the clinical outcome
2 Cortes JE, Talpaz M, Cabanillas F et al. Serum levels of
of diffuse large B-cell lymphoma. Blood 2004; 103: 3529–3534.
interleukin-10 in patients with diffuse large cell lymphoma:
23 Berglund M, Thunberg U, Roos G et al. The interleukin-10
lack of correlation with prognosis. Blood 1995; 85: 2516–2520.
gene promoter polymorphism (À1082) does not correlate with
3 Stasi R, Zinzani PL, Galieni P et al. Prognostic value of serum
clinical outcome in diffuse large B-cell lymphoma. Blood 2005;
IL-10 and soluble IL-2 receptor levels in aggressive non-
105: 4894–4895 and author reply 4895.
Hodgkin’s lymphoma. Br J Haematol 1994; 88: 770–777.
24 Rothman N, Skibola CF, Wang SS et al. Genetic variation in
4 Blay JY, Burdin N, Rousset F et al. Serum interleukin-10 in non-
TNF and IL10 and risk of non-Hodgkin lymphoma: a report
Hodgkin’s lymphoma: a prognostic factor. Blood 1993; 82:
from the InterLymph Consortium. Lancet Oncol 2006; 7: 27–38.
25 Nieters A, Beckmann L, Deeg E et al. Gene polymorphisms in
5 Burdin N, Rousset F, Banchereau J. B-cell-derived IL-10:
Toll-like receptors, interleukin-10, and interleukin-10 receptor
production and function. Methods 1997; 11: 98–111.
alpha and lymphoma risk. Genes Immun 2006.
6 Keystone E, Wherry J, Grint P. IL-10 as a therapeutic strategy
26 Pfreundschuh M, Trumper L, Kloess M et al. Two-weekly or 3-
in the treatment of rheumatoid arthritis. Rheumatic Dis Clin
weekly CHOP chemotherapy with or without etoposide for
the treatment of elderly patients with aggressive lymphomas:
7 Ferraccioli G, Falleti E, DeVita S et al. Circulating levels of
results of the NHL-B2 trial of the DSHNHL. Blood 2004; 104:
interleukin 10 and other cytokines in rheumatoid arthritis
treated with cyclosporin A or combination therapy. J Rheum
27 Pfreundschuh M, Trumper L, Kloess M et al. Two-weekly or 3-
weekly CHOP chemotherapy with or without etoposide for
8 Ho M, Schollaardt T, Snape S et al. Endogenous interleukin-10
the treatment of young patients with good-prognosis (normal
modulates proinflammatory response in Plasmodium falci-
LDH) aggressive lymphomas: results of the NHL-B1 trial of
parum malaria. J Infect Dis 1998; 178: 520–525.
the DSHNHL. Blood 2004; 104: 626–633.
9 Sarris AH, Kliche KO, Pethambaram P et al. Interleukin-10
28 Wojnowski L, Kulle B, Schirmer M et al. NAD(P)H oxidase
levels are often elevated in serum of adults with Hodgkin’s
and multidrug resistance protein genetic polymorphisms are
disease and are associated with inferior failure-free survival.
associated with doxorubicin-induced cardiotoxicity. Circula-
10 Goldman M, Velu T, Pretolani M. Interleukin-10. Actions and
29 Im SH, Hueber A, Monticelli S et al. Chromatin-level
therapeutic potential. BioDrugs 1997; 7: 6–14.
regulation of the IL10 gene in T cells. J Biol Chem 2004; 279:
11 Lalani I, Bhol K, Ahmed A. Interleukin-10: biology, role in
inflammation and autoimmunity. Ann All Asth Immunol 1997;
30 Zhang X, Edwards JP, Mosser DM. Dynamic and transient
remodeling of the macrophage IL-10 promoter during
12 Narula SK, Cutler D, Grint P. Immunomodulation of Crohn’s
transcription. J Immunol 2006; 177: 1282–1288.
disease by Interleukin-10. Agents and Actions Suppl 1997.
31 Wang ZY, Sato H, Kusam S et al. Regulation of IL-10 gene
13 Van Deventer SJ. Immunotherapy of Crohn’s disease. Scand
expression in Th2 cells by Jun proteins. J Immunol 2005; 174:
14 Cavet J, Middleton P, Segall M et al. Recipient tumor necrosis
32 Shoemaker J, Saraiva M, O’Garra A. GATA-3 directly
factor-alpha and interleukin-10 gene polymorphisms associate
remodels the IL-10 locus independently of IL-4 in CD4+ T
with early mortality and acute graft-versus-host disease
cells. J Immunol 2006; 176: 3470–3479.
severity in HLA-matched sibling bone marrow transplants.
33 Saraiva M, Christensen JR, Tsytsykova AV et al. Identification
of a macrophage-specific chromatin signature in the IL-10
15 Hollegaard MV, Bidwell JL. Cytokine gene polymorphism in
locus. J Immunol 2005; 175: 1041–1046.
human disease: on-line databases, Supplement 3. Genes Immun
34 Lucas M, Zhang X, Prasanna V et al. ERK activation following
macrophage FcgammaR ligation leads to chromatin modifica-
16 Turner D, Williams D, Sankaran D et al. An investigation of
tions at the IL-10 locus. J Immunol 2005; 175: 469–477.
polymorphism in the interleukin-10 gene promoter. Eur J
35 Jones EA, Flavell RA. Distal enhancer elements transcribe
intergenic RNA in the IL-10 family gene cluster. J Immunol
17 Westendorp R, Langermans J, Huizinga T et al. Genetic
influence on cytokine production and fatal meningococcal
36 Lan Q, Zheng T, Rothman N et al. Cytokine polymorphisms in
UNCORRECTED PROOF
disease. Lancet 1997; 349: 170–173.
the Th1/Th2 pathway and susceptibility to non-Hodgkin
18 Gibson AW, Edberg JC, Wu J et al. Novel single nucleotide
lymphoma. Blood 2006; 107: 4101–4108.
polymorphisms in the distal IL-10 promoter affect IL-10production and enhance the risk of systemic lupus erythema-tosus. J Immunol 2001; 166: 3915–3922. Genes and Immunity
Pedemontana, famiglie al Tar - la tribuna di Treviso dal 2003.it » Ricerca ARCHIVIO la tribuna di Treviso dal 2003 Pedemontana, famiglie al Tar la tribuna di Treviso — 20 marzo 2010 pagina 39 sezione: PROVINCIA VOLPAGO. Tanto tuonò che piovve. Per quanti erano convinti che i comitati anti-Pedemontana si sarebbero rassegnati al loro destino dopo la conferenza dei servizi e l’imminent
 Genes and Immunity (2006) 00, 1–4& 2006 Nature Publishing Group All rights reserved 1466-4879/06 $30.00
SHORT COMMUNICATIONThe interleukin-10 gene promoter polymorphismÀ1087AG does not correlate with clinical outcome in non-Hodgkin’s lymphoma
D Kube1, T-D Hua1, M Klo¨ss2, B Kulle3,4, J Brockmo¨ller5, L Wojnowski5,6, M Lo¨ffler2, M Pfreundschuh7and L Tru¨mper11Department of Internal Medicine Hematology and Oncology, Georg-August Universita¨t Go¨ttingen, Mainz, Germany; 2University ofLeipzig, Mainz, Germany; 3Institute of Epidemiology, Mainz, Germany; 4Section of Statistics, Institute of Basic Medical Science,University of Oslo, Oslo, Norway; 5Department of Pharmacology and Toxicology, Mainz, Germany; 6University Mainz, Institute ofPharmacology, Mainz, Germany and 7Department of Internal Medicine I, Saarland University, Homburg/Saar for the DSHNHL(German High Grade NHL Study Group), Mainz, Germany
The Interleukin 10 (IL-10) gene is highly polymorphic, and the IL-10À
(rs1800896) gene variation is the only so far studied
intensively in association with certain diseases. Conflicting data have been published about an association of IL-10À
variation with lower rates of complete remission and lower overall survival (OS) in patients with diffuse large B-cell lymphoma.
Genes and Immunity (2006) 00, 1–4& 2006 Nature Publishing Group All rights reserved 1466-4879/06 $30.00
SHORT COMMUNICATIONThe interleukin-10 gene promoter polymorphismÀ1087AG does not correlate with clinical outcome in non-Hodgkin’s lymphoma
D Kube1, T-D Hua1, M Klo¨ss2, B Kulle3,4, J Brockmo¨ller5, L Wojnowski5,6, M Lo¨ffler2, M Pfreundschuh7and L Tru¨mper11Department of Internal Medicine Hematology and Oncology, Georg-August Universita¨t Go¨ttingen, Mainz, Germany; 2University ofLeipzig, Mainz, Germany; 3Institute of Epidemiology, Mainz, Germany; 4Section of Statistics, Institute of Basic Medical Science,University of Oslo, Oslo, Norway; 5Department of Pharmacology and Toxicology, Mainz, Germany; 6University Mainz, Institute ofPharmacology, Mainz, Germany and 7Department of Internal Medicine I, Saarland University, Homburg/Saar for the DSHNHL(German High Grade NHL Study Group), Mainz, Germany
The Interleukin 10 (IL-10) gene is highly polymorphic, and the IL-10À
(rs1800896) gene variation is the only so far studied
intensively in association with certain diseases. Conflicting data have been published about an association of IL-10À
variation with lower rates of complete remission and lower overall survival (OS) in patients with diffuse large B-cell lymphoma. Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
genotype, in comparison to IL-10À3538, IL-10À1354, IL-
All patients included in this study received anthracy-
10À824 and IL-10À597 genotypes (rs 1800893, 1800871 and
cline-containing regimens, consisting of CHOP/CHOEP
1800872, respectively) in patients from the NHL-B1/ B2
(cyclophosphamide, adriamycin, vincristine, etoposide,
studies from the German High-Grade Non-Hodgkin’s
prednisone).26,27 Complete remission (CR) was defined as
Lymphoma Study Group (DSHNHL) and compared it
the disappearance of all disease manifestations for at
with OS and event-free survival (EFS).26,27 We used for
least 2 months after the final restaging. EFS was
this analysis a homogeneous, equally treated cohort of
determined from the onset of treatment until either
patients with non-Hodgkin’s Lymphoma (NHL). Pa-
disease progression, initiation of salvage therapy; or
tients were eligible if they had previously untreated,
additional (off-protocol) treatment, relapse, death or in
biopsy-confirmed, aggressive NHL according to the
case of no event OS was determined from the onset of
Revised European-American Lymphoma Classification
treatment until the last follow-up evaluation or death
(translated into the World Health Organization (WHO)
from any cause. Within 5 years the OS was 60.2% (95%
classification). Patients were excluded if the diagnosis of
confidence interval: 54.8:65.5) for all and 61.8% (95%
aggressive lymphoma was not confirmed (i.e., no
confidence interval: 55.3:68.3) for the DLBCL subgroup.
Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
genotype, in comparison to IL-10À3538, IL-10À1354, IL-
All patients included in this study received anthracy-
10À824 and IL-10À597 genotypes (rs 1800893, 1800871 and
cline-containing regimens, consisting of CHOP/CHOEP
1800872, respectively) in patients from the NHL-B1/ B2
(cyclophosphamide, adriamycin, vincristine, etoposide,
studies from the German High-Grade Non-Hodgkin’s
prednisone).26,27 Complete remission (CR) was defined as
Lymphoma Study Group (DSHNHL) and compared it
the disappearance of all disease manifestations for at
with OS and event-free survival (EFS).26,27 We used for
least 2 months after the final restaging. EFS was
this analysis a homogeneous, equally treated cohort of
determined from the onset of treatment until either
patients with non-Hodgkin’s Lymphoma (NHL). Pa-
disease progression, initiation of salvage therapy; or
tients were eligible if they had previously untreated,
additional (off-protocol) treatment, relapse, death or in
biopsy-confirmed, aggressive NHL according to the
case of no event OS was determined from the onset of
Revised European-American Lymphoma Classification
treatment until the last follow-up evaluation or death
(translated into the World Health Organization (WHO)
from any cause. Within 5 years the OS was 60.2% (95%
classification). Patients were excluded if the diagnosis of
confidence interval: 54.8:65.5) for all and 61.8% (95%
aggressive lymphoma was not confirmed (i.e., no
confidence interval: 55.3:68.3) for the DLBCL subgroup.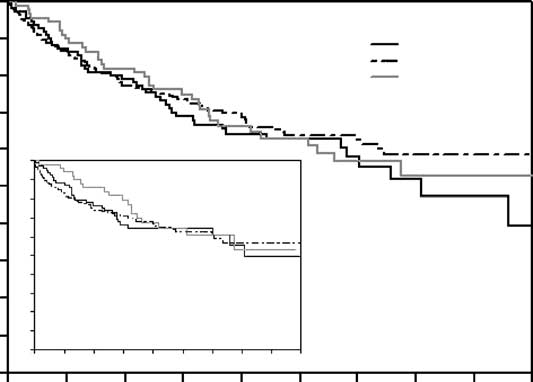
 Interleukin-10, polymorphism, non-Hodgkin’s lymphomaD Kube et al
OS for the 409 patients with NHL in comparison to the IL-10 –1087 genotype. Inset presents the same data for the DLBCL group
increase of IL-10–1087G alleles was found. In addition, we
producer haplotype.16,18–21 The mechanism behind this
did not find any difference in OS (all P ¼ 0.704, DLBC
is still unkown, probably because of the close proximity
P ¼ 0.892) or EFS (all P ¼ 0.822, DLBC 0.86) between
of À1087AG to the IL-10.G microsatellite. The IL-10.R
patients with IL-10–1087AA genotype and the other
microsatellite in close proximity of À3538AT may also
genotypes, calculated in different ways as presented by
affect IL-10 expression levels. First reports on structural
Lech-Maranda et al. or Berglund et al. (Figure 1). No
changes of the chromatin within the IL10 gene in
significant differences in the clinical presentation were
differentiated Th1 and Th2 cells or macrophages empha-
detected between the genotype groups compared when
size the surprising diversity of mechanisms used to
sex, the factors of international prognostic index (IPI)
regulate cytokine gene expression at the chromatin level
(age460, LDH4N, ECOG41, stage III/IV, extranodal
and might be opening the chance to understand the
involvement 41) or the IPI score were taken into
mechanism of interindividual differences in IL-10 ex-
consideration. There were no differences according to
pression.29–34 DNase I-hypersensitive sites on a con-
the complete remission rate between the genotype
served 40-kb region between the IL-19 and IL-10 genes in
groups. No associations were found between the prog-
different murine T-cell populations revealed three
nostic variables, EFS, or OS intervals and alleles/
enhancer elements, which function in T cells in vitro.35
genotypes for the other analysed gene loci (OS: À3538
The role of inherited factors in the extend of IL-10
deregulation in malignant disorders is still controversy.
Interleukin-10, polymorphism, non-Hodgkin’s lymphomaD Kube et al
OS for the 409 patients with NHL in comparison to the IL-10 –1087 genotype. Inset presents the same data for the DLBCL group
increase of IL-10–1087G alleles was found. In addition, we
producer haplotype.16,18–21 The mechanism behind this
did not find any difference in OS (all P ¼ 0.704, DLBC
is still unkown, probably because of the close proximity
P ¼ 0.892) or EFS (all P ¼ 0.822, DLBC 0.86) between
of À1087AG to the IL-10.G microsatellite. The IL-10.R
patients with IL-10–1087AA genotype and the other
microsatellite in close proximity of À3538AT may also
genotypes, calculated in different ways as presented by
affect IL-10 expression levels. First reports on structural
Lech-Maranda et al. or Berglund et al. (Figure 1). No
changes of the chromatin within the IL10 gene in
significant differences in the clinical presentation were
differentiated Th1 and Th2 cells or macrophages empha-
detected between the genotype groups compared when
size the surprising diversity of mechanisms used to
sex, the factors of international prognostic index (IPI)
regulate cytokine gene expression at the chromatin level
(age460, LDH4N, ECOG41, stage III/IV, extranodal
and might be opening the chance to understand the
involvement 41) or the IPI score were taken into
mechanism of interindividual differences in IL-10 ex-
consideration. There were no differences according to
pression.29–34 DNase I-hypersensitive sites on a con-
the complete remission rate between the genotype
served 40-kb region between the IL-19 and IL-10 genes in
groups. No associations were found between the prog-
different murine T-cell populations revealed three
nostic variables, EFS, or OS intervals and alleles/
enhancer elements, which function in T cells in vitro.35
genotypes for the other analysed gene loci (OS: À3538
The role of inherited factors in the extend of IL-10
deregulation in malignant disorders is still controversy. Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
19 Eskdale J, Gallagher G, Verweij C et al. Interleukin 10 secretion
in relation to human IL-10 locus haplotypes. Proc Natl Acad Sci
The authors are gratefull to the Deutsche Forschnugsge-
meinschaft (Graduiertenkolleg 1034), the BMBF (NGFN-
20 Crawley E, Kay R, Sillibourne J et al. Polymorphic haplotypes
1) and the Deutsche Krebshilfe/BMBF (NHL-B) for
of the IL-10 50 flanking region determine variable IL-10
transcription and are associated with particular phenotypesof juvenile rheumatoid arthritis. Arthr Rheum 1999; 42: 1101–1108.
Interleukin-10, polymorphism, non-Hodgkin’s lymphoma
19 Eskdale J, Gallagher G, Verweij C et al. Interleukin 10 secretion
in relation to human IL-10 locus haplotypes. Proc Natl Acad Sci
The authors are gratefull to the Deutsche Forschnugsge-
meinschaft (Graduiertenkolleg 1034), the BMBF (NGFN-
20 Crawley E, Kay R, Sillibourne J et al. Polymorphic haplotypes
1) and the Deutsche Krebshilfe/BMBF (NHL-B) for
of the IL-10 50 flanking region determine variable IL-10
transcription and are associated with particular phenotypesof juvenile rheumatoid arthritis. Arthr Rheum 1999; 42: 1101–1108.