Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
C:\documents and settings\bradym\desktop\4b9f3119-0e5a-01d8-427d8969c87b90bb.html
Wednesday, June 01 A Message from Cardiology Associates, LLC
Welcome to the June 2011 issue of our Cardiology Associates' Referring
Physician Newsletter. The newsletter will focus on pregnancy-related
cardiovascular disease, in particular hypertension (HTN) in pregnant and
post-partum women. As women are waiting until later in life to have
children, we are more often seeing patients with either chronic HTN,
which needs to be managed throughout pregnancy, or are called on to
help treat hypertension throughout and after pregnancy in women of
advanced maternal age (greater than 35 years old at the time of
conception). The risk of preeclampsia is typically higher in this age
group. The case described below will outline some management issues
related to HTN in pregnancy: definition of various hypertensive
conditions, risks of hypertension in pregnancy, and review the pharmacologic treatment options
that are safe in pregnancy and breastfeeding. About the Author
Dr. Stephanie Jacobs is a CALLC cardiologist who has been board-certified in internal medicine
and cardiovascular disease. Dr. Jacobs has a special interest in consultative cardiology, nuclear
cardiology, and pregnancy-related cardiovascular disease. Dr. Jacobs graduated from the
Georgetown University School of Medicine, and she is a member of the American Heart
Association, the American College of Cardiology, the American Society of Echocardiography, and
Dr. Jacobs sees patients at our Annapolis and Bowie offices. Cardiovascular Disease and Pregnancy PRESENTATION OF CASE
• Patient is a 41-year-old Caucasian female who
delivered a healthy baby boy on March 1, 2011.
• No cardiopulmonary issues or symptoms
• Prior to the last week of pregnancy, the patient's
blood pressure ran from 110/70 pre-partum to
• The patient's urine was negative for protein.
• At 39 weeks, the patient's blood pressure was
noted to be 135/88, but her urine remained negative for protein.
• The patient delivered at 40 weeks and 1 day without complications. Nine days
later, she presented to the Anne Arundel Medical Center ER with a severe
headache and was found to have a blood pressure of 211/108. DISCUSSION
There are 4 major hypertensive disorders that occur in pregnant woman.
Preeclampsia superimposed upon preexisting hypertension
The diagnosis of a hypertensive disorder in a pregnant woman depends, in part, upon the
gestational age at presentation. Preeclampsia refers to the syndrome of new onset of
hypertension and proteinuria after 20 weeks of gestation in a previously normotensive woman or
worsening hypertension with new onset proteinuria in a woman with preexisting hypertension
(superimposed preeclampsia). Preexisting hypertension(chronic HTN) is defined as having a
blood pressure reading higher than 140/90 mmHg that antedates pregnancy, is present before
the 20th week of pregnancy, or persists longer than 12 weeks postpartum(1). Gestational
hypertension refers to elevated blood pressure first detected after 20 weeks of gestation in the
absence of proteinuria. Over time, some patients with gestational hypertension will develop
proteinuria and be considered preeclamptic, while others will be diagnosed with chronic or
preexsisting hypertension because of persistent blood pressure elevation lasting longer than 12
Preeclampsia with proteinuria and blood pressure elevation higher than 140/90 is treated with
blood pressure control medication for as long as necessary to gain fetal maturity and delivery.
(Preeclampsia can result in maternal and fetal complications and was not present in our patient.
It will not be discussed in further detail here.) Eclampsia is the additional manifestation of
seizures and can be life-threatening to both mother and fetus. The treatment is emergent
The other two hypertensive states of pregnancy are not associated with proteinuria, and as such
not all pregnant women with elevations in their blood pressure need to be given medication. Mild
HTN in pregnancy without proteinuria, in general, has favorable maternal and fetal outcomes.
The decision to start medication must balance the risks of drug therapy to the fetus versus the
risk of no treatment to both mother and fetus. The major maternal indications for treatment of
HTN in pregnant women are similar to those of non-pregnant women and include prevention of
stroke and cardiovascular complications. Preexisting HTN increases the risk of adverse pregnancy
outcomes. Superimposed preeclampsia is 2-4 times more likely in hypertensive women (10-20%
risk) than in non-HTN women. Women with mild preexisting HTN have a .7-1.5% risk of
abruption, 12-34% risk of preterm birth less than 37 weeks, and 8-16% risk of fetal growth
restriction. For women with preexisting severe HTN, the risks were 2-to-5 fold higher. (2)
Certainly too, a woman with symptoms of end-organ involvement such as chest pain, headache,
or breathlessness should be considered for treatment.
Although there is very little maternal risk to lowering blood pressure, there is some data to
suggest that blood pressure lowering therapy may compromise fetal well-being as a result of
reduced placental perfusion. (3) This conclusion was further supported by a meta-analysis that
looked at maternal and fetal outcomes in randomized trials of treatment versus no treatment of
pregnant women with mild to moderate hypertension (defined as blood pressure of 140 to
Antihypertensive therapy of mild hypertension significantly decreased the incidence of
severe hypertension by one-half to two-thirds and the need for additional
antihypertensive drugs by almost two-thirds. (2)
Antihypertensive therapy of mild hypertension did not decrease fetal risks associated with
maternal HTN including: perinatal mortality rate or the frequency of prematurity,
preeclampsia, delivery of a small for gestational age infant, or abruptio placentae
Another meta-analysis showed that fetal growth was impaired by a reduction in maternal blood
pressure: a 10 mmHg decrease was associated with a 176 gram decrease in birth weight. This
was unrelated to the type of medication used. (3)
The definition of HTN in pregnancy does not follow that of non-pregnant individuals (pre, stage
1,2,3) but rather is either normal, mild (140-159/90-109mmHg), or severe (>160/110 mmHg).
Thus, the guidelines from an obstetrical standpoint (ACOG) state that "the only demonstrable
benefit of antihypertensive therapy in women with mild hypertension is a reduction in risk of
developing severe hypertension, which is considered insufficient to warrant exposing the fetus to
the potential adverse effects on its growth." Most experts do agree, however, that severe
hypertension should be treated to prevent maternal vascular complications. (1) One may initiate
treatment in younger women with lower baseline blood pressure (<90/75) before the 150/100
mmHg mark. Our patient had clear indication for treatment. The patient was started on IV labatelol, and HCT negative for bleed or CVA, and CXR and labs were normal. Her 12 lead EKG was normal. She was sent home on PO labetalol 400 mg TID. She returned to the ER three days later with continued blood pressure elevations of 170-180/90-110 and occasional controlled blood pressure readings of 120-135/80-95.
The choice of drug to treat anything other than mild HTN is based on general agreement,
historical use/safety reporting, and limited trial data. All anti-HTN drugs cross the placenta and
there are no large randomized trials upon which to recommend one drug over another. Drugs
that have been found to be safe include: methyldopa or labatelol as first line agents, nifedipine
as second or third line, and pindolol or metoprolol as acceptable alternatives. Verapamil and
diltiazem have been reported as safe, although studies were conducted with small numbers of
women. The dose ranges for the three most common drugs are:
It is generally agreed that ACE-I/ARB and direct renin inhibiters NOT be administered during
pregnancy, and some beta-blockers such as propranolol specifically have had reports of
premature labor, neonatal apnea, bradycardia, and hypoglycemia. Amlodipine is not often used
as there is sparse data to support it.
Initiation of treatment is for blood pressure higher than 150/100 mmHg, or signs of maternal
end-organ damage and the goal of pharmacologic therapy is a blood pressure target of 140-
150/90-100 mmHg. If the patient is breastfeeding or planning to, certain drugs are deemed safe
by AAP: propranolol, metoprolol, labatelol, diltiazem, nifedipine, and verapamil. Drugs to be
avoided in lactating women are acebutolol, atenolol and ACEI (due to higher rates of newborn
Procardia XL 60 mg qd was added. The following day the patient's blood pressure was 99/67 and she was lightheaded, diaphoretic, and felt weak. She presented to Cardiology Associates, LLC, two days later. Her blood pressure was 120/78, pulse 62, physical exam normal, and EKG normal. She was taking Labatelol 400 mg PO tid and Procardia XL 60mg PO qd.
Gestational hypertension, which by definition is what our patient experienced, occurs in about
6% of pregnancies and is a temporary diagnosis for women who do not meet criteria for
preeclampsia or chronic HTN (preexisting). The diagnosis is changed if proteniuria develops
(preeclampsia), if blood pressure elevation persists beyond 12 weeks postpartum (chronic HTN)
or is simply determined to be transient HTN given that blood pressure returns to normal by 12
weeks postpartum. Gestational HTN prior to delivery increases the risk of the development of
preeclampsia and therefore patients should be screened for signs or symptoms of preeclampsia
(severe H/A, n/v, RUQ pain or epigastric pain, dec urine output, visual changes). (6)
Over the next week in our office the patient's only complaint was fatigue and a feeling of "sluggishness with activity" with a resting heart rate of 50-60 bpm. An echocardiogram was performed (which showed nothing out of the ordinary), and the patient's blood pressure continued to steadily decline. Her labatelol was decreased to 200mg PO bid, and her procardia XL remained 60mg PO qd.
It is unclear if the patient will progress to chronic HTN at 5 weeks post partum. She has about a
15% risk of doing so. We will follow her out to 12 weeks, but if her blood pressure continues to
decline, we will stop the labatelol and wean the procardia. References:
1. Working group report on high blood pressure in pregnancy. National Institutes of Health,
2. Abalos, E, Duley, L, Steyn, DW, Henderson-Smart, DJ. Antihypertensive drug therapy for
mild to moderate hypertension during pregnancy. Cochrane Database Syst Rev 2007;
3. von Dadelszen, P, Magee, LA. Fall in mean arterial pressure and fetal growth restriction in
pregnancy hypertension: an updated metaregression analysis. J Obstet Gynaecol Can
4. Beardmore, KS, Morris, JM, Gallery, ED. Excretion of antihypertensive medication into
human breast milk: a systematic review. Hypertens Pregnancy 2002; 21:85.
5. Boutroy, MJ, Bianchetti, G, Dubruc, C, et al. To nurse when receiving acebutolol: is it
dangerous for the neonate? Eur J Clin Pharmacol 1986; 30:737.
6. ACOG Committee on Practice Bulletins--Obstetrics. ACOG practice bulletin. Diagnosis and
management of preeclampsia and eclampsia. Number 33, January 2002. Obstet Gynecol
Please Join Our Mailing List
We are offering you this monthly newsletter as a way to provide cardiovascular news and
update you on developments within our field. For your convenience, we are distributing our
newsletter via e-mail. Visit our site at ( click the Referring Physician
Newsletter link at the upper left corner of our home page. You will receive an e-Newsletter every
month featuring an article or a case report from one of our physicians and links to other sources
featuring new trends in the field of cardiology. Our focus will be on real questions and issues
that we encounter in our day-to-day medical practice. In fact, if there is a topic that is of
particular interest to you (or a question that is related to any of our articles) please e-mail your
inquiries to our Project Manager, Nazar Snihur at (Of course, we will
not share your e-mail address outside of our offices.)
Our Locations Annapolis Cardiology Office Annapolis Vascular Office Bowie Office Irving Street 4800N Kent Island Office K Street Office Olney Office
You have received this message because your email address is part of our electronic mailing list.
If you wish to be removed from our mailing list, please visit our page and enter
your email address for removal from our system.
Technical Data Sheet LT-04-06 10/06/2013 Technical data sheet PLUS 720 Polyester resin PROPERTIES PLUS 720 POLYESTER RESIN is a product for manual lamination. It contains a structural polyester resin with addition of appropriate catalysts. Use 50% of the benzoyl peroxide paste (NOVOL part no. 522) as the hardener. The product is intended for repairing large defects and
Epilepsy in Rett syndrome – notes for talk at ORSA meeting, September 2010 This talk was part of a three-person panel discussion and had two principal 1) to describe why and how epileptic seizures develop in the human brain 2) to review the main features of epilepsy in Rett syndrome (RTT) – what kinds of seizures occur and at what age; who is more likely to develop epileptic seizures; wh







 Wednesday, June 01
Wednesday, June 01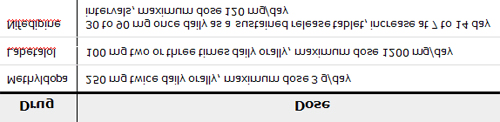 The choice of drug to treat anything other than mild HTN is based on general agreement,
historical use/safety reporting, and limited trial data. All anti-HTN drugs cross the placenta and
there are no large randomized trials upon which to recommend one drug over another. Drugs
that have been found to be safe include: methyldopa or labatelol as first line agents, nifedipine
as second or third line, and pindolol or metoprolol as acceptable alternatives. Verapamil and
diltiazem have been reported as safe, although studies were conducted with small numbers of
women. The dose ranges for the three most common drugs are:
It is generally agreed that ACE-I/ARB and direct renin inhibiters NOT be administered during
pregnancy, and some beta-blockers such as propranolol specifically have had reports of
premature labor, neonatal apnea, bradycardia, and hypoglycemia. Amlodipine is not often used
as there is sparse data to support it.
The choice of drug to treat anything other than mild HTN is based on general agreement,
historical use/safety reporting, and limited trial data. All anti-HTN drugs cross the placenta and
there are no large randomized trials upon which to recommend one drug over another. Drugs
that have been found to be safe include: methyldopa or labatelol as first line agents, nifedipine
as second or third line, and pindolol or metoprolol as acceptable alternatives. Verapamil and
diltiazem have been reported as safe, although studies were conducted with small numbers of
women. The dose ranges for the three most common drugs are:
It is generally agreed that ACE-I/ARB and direct renin inhibiters NOT be administered during
pregnancy, and some beta-blockers such as propranolol specifically have had reports of
premature labor, neonatal apnea, bradycardia, and hypoglycemia. Amlodipine is not often used
as there is sparse data to support it.
 5. Boutroy, MJ, Bianchetti, G, Dubruc, C, et al. To nurse when receiving acebutolol: is it
dangerous for the neonate? Eur J Clin Pharmacol 1986; 30:737.
5. Boutroy, MJ, Bianchetti, G, Dubruc, C, et al. To nurse when receiving acebutolol: is it
dangerous for the neonate? Eur J Clin Pharmacol 1986; 30:737.