Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Functionalneurology.com
FUNCTIONAL IMPROVEMENT IN PATIENTS WITH SEVERE SPINAL SPA S T I C I T Y TREATED WITH CHRONIC INTRATHECAL BACLOFEN INFUSION Alessandro Dario, Carlo Scamoni, Giorgio
In this retrospective study we evaluated the efficacy
Bono*, Angelo Ghezzi**, Mauro Zaffaroni**
and functional benefits of chronic intrathecal baclofeninfusion in severe spinal spasticity. Twenty patients with a diagnosis of severe intractable
Department of Neurosurgery, *Unit of Neurology,
spinal spasticity were evaluated prior to implantation
“Ospedale di Circolo”, Varese; **Multiple Sclero-
of a programmable pump for chronic intrathecal ba-
sis Center, Gallarate Hospital, Varese, Italy
clofen therapy and at follow up, which ranged from 12to 36 months (mean 22.4 months). The mean age of the patients was 39.1 years. The pre-
Reprint requests to: Dr Alessandro Dario, Via Torriani, 32
vailing pathology was multiple sclerosis. All were un-
Patient assessment was based on the Ashworth Scale,
the Spasms Frequency Scale, self-reported pain andFunctional Independence Measure (FIM) scores. TheWilcoxon test was used for statistical analysis. A statistically significant decrease in muscle tone, spasmsand pain was observed in all the patients. The Ashworthscore decreased from 4.4 to 1.8, the spasms frequencyscore from 2.5 to 0.5 and the self-reported pain score from5.5 to 2.3. The FIM score also showed a statistically sig-nificant change (increasing from a mean of 33.8 to 58.7). Two patients in employment were able to return to work. No severe side effects were observed. Chronic intrathecal baclofen infusion was seen to pro-duce a functional improvement in patients with severespinal spasticity, particularly as regards bathing, com-fortable wheelchair sitting and mobility.
KEY WORDS: Baclofen, intrathecal infusion, spinalspasticity.
sent, intrathecal infusion pump implantation isregarded as a safe surgical technique.
Chronic intrathecal baclofen infusion has
been shown to be particularly indicated for se-
functional improvement (3) or self-reported
vere spasticity of spinal origin, producing an
pain (4) after chronic intrathecal baclofen infu-
improvement in symptoms (1,2). The results
obtained by this treatment do not differ signifi-
cantly between patients with spinal cord injury
the possibility of obtaining a functional im-
and those with multiple sclerosis (2). At pre-
Functional Independence Measure (FIM) score(8).
Twenty patients (9 males, 11 females) all
These parameters were assessed before in-
a ffected by severe progressive spinal spasticity
trathecal therapy, 6 and 12 hours after bolus ad-
that was not responsive to medical therapy and
ministration of intrathecal baclofen and every 6
that interfered with their daily activities, were
evaluated for chronic intrathecal baclofen infu-
sion. Before beginning the study, all the patients
lumbar puncture performed at L3-L4 interspace.
signed the necessary informed consent form and
When a positive response was obtained (at least
approval was obtained from our institute’s ethics
one point reduction in AS and/or SFS score), a
continuous infusion pump (Synchromed Model
All the patients were in a stable neurologi-
8616-18, Medtronic Inc.,Minneapolis, USA)
cal spastic condition of at least 12 months’ dura-
tion and all were unable to walk. The spasticity
The statistical analysis was performed us-
was caused by multiple sclerosis in 13 patients,
ing the Wilcoxon sign rank test (8) to evaluate
by trauma in 4, by spinal tumors in 2 and by
d i fferences between baseline values and those
spinal myelitis in 1. All the patients but two had
observed at the last follow up. Surgical compli-
a spastic paraparesis; of these two patients, one
cations and the side effects of intrathecal ba-
was suffering from a cervical myelitis and the
other had cerebral and spinal plaques caused bymultiple sclerosis. Of the 13 patients with multi-ple sclerosis 7 had diffuse spinal plaques, 5 had
d i ffuse spinal and cerebral plaques and one hadonly cerebral plaques; three patients also had
tremors of the arms and one was suffering from
Their clinical history of spasticity had a
The presurgical treatment with oral anti-
duration of at least 12 months (mean: 36.5
spasmodic drugs included a combination of ba-
months); the patients were followed up for a
clofen, diazepam and tizanidine; this combina-
mean of 22.4 months (range: 12-36 months) af-
tion was progressively increased to a maximum
ter implantation. The AS and SFS scores were
dose of baclofen 50 mg, tizanidine 4 mg, and
seen to decrease by at least one point after the
diazepam 10 mg in order to obtain the thera-
peutic effect; reduced consciousness emerg e d
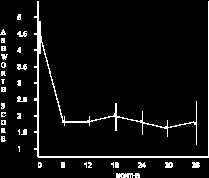
At the last follow up, the mean AS score was
as a side effect of this oral therapy in seven pa-
seen to have decreased from a preoperative value
tients. During the bolus screening prior to in-
of 4.4±0.5 to a postoperative value of 1.8±0.7
trathecal baclofen treatment (25, 50, 75, and
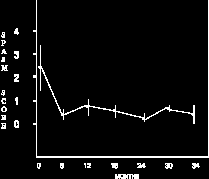
(Fig. 1). The SFS score in thirteen patients had de-
100 µgr at intervals of 48 hours) the adminis-
creased from a preoperative value of 2.5±0.8 to a
tration of this drug per os was interrupted.
postoperative value of 0.5±0.4 (Fig. 2); these dif-
The patients’ neurological conditions were
ferences between baseline and follow-up spasticity
evaluated using the original Ashworth Scale
were statistically significant (p < 0.01). The self-
(AS) to assess spasticity (5) and the four-point
reported pain score had decreased from a preoper-
ative score of 5.5±2.2 to a postoperative score of
spasms (6); the painful state was evaluated on
2.3±1.9 (p < 0.05) (Fig. 3, see p. 314). A statisti-
the basis of self-reported pain (7) while physi-
cally significant change in the FIM score was also
cal disability was evaluated on the basis of the
observed (an increase from a preoperative mean of
Functional improvement after intrathecal baclofen
t r a r y, the improvement seen in the patients withtetraparesis was only slight.
Two patients in employment were able to re-
sume work. No differences emerged between theresults of the patients with spinal cord injuriesand those with multiple sclerosis.
After implantation five patients needed a
progressive increase of the baclofen infusion. The mean daily dose of baclofen was 295 µg r(range: 90-830 µgr). Two patients with pain hadan infusion of a mixture of baclofen and mor-phine (respectively 200 µgr + 0.3 mgr/day and310 µgr + 0.5 mgr/day). Sedation provoked byprevious oral antispasmodic drug intake was seento improve in all patients. No side effects due to
Fig. 1 - Graph showing the average spasticity according
intrathecal baclofen administration were ob-
to the Ashworth Scale scores before treatment and at fol-
served; one patient had a cerebrospinal fluid leak
low ups (the vertical lines indicate standard deviation).
around the catheter that required surgical repair.
The chronic intrathecal infusion of baclofen
by implanted pump for the treatment of spastici-ty associated with spinal disorders (2) is today asafe and accepted therapeutic tool (1,2): im-provements in muscle tone and reductions ofspasms are well documented (1); however thedisappearance of spasticity does not necessarilyequate with functional improvement (6), andfew studies have focused on this aspect (3,7). In accordance with the literature (1), our datashow improvements as regards muscle toneand spasms (Fig.s 1 and 2).
Moreover, in our small sample this surgi-
cal technique also led in the long-term to a sig-
Fig. 2 - Graph showing the Spasm Frequency Scale sco-
nificant improvement of FIM as well as self-re-
res of extremities before treatment and at follow ups (the
horizontal lines indicate standard deviation).
Given their particularly severe clinical con-
ditions it was felt that the two patients in ourstudy who had tetraparesis could not be ade-
33.8±6.9 to a postoperative mean of 58.7±10.4 (p
quately assessed using disability scales such as
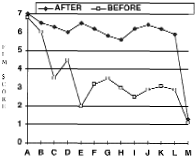
< 0.05) (Fig. 4). In particular the improvement re-
garded items C, E, I and J: bathing, dressing the
The benefit in our patients suffering from
lower body and transferring the body. On the con-
paraparesis was reflected in almost all the indi-
vidual FIM motor items but mainly in bathing,dressing the lower body and transferring thebody (Fig. 4). In this study the functional re-sults obtained did not differ between spinalcord injury and multiple sclerosis patients, butthese findings could be due to what was, in re-lation to the progressive worsening that occursin multiple sclerosis, a relatively short follow-up time (11).
Implantation is apparently more expensive
than other procedures (12), thus the amount offunctional improvement and quality of life (4)could be parameters useful for calculating thesocial cost-benefit ratio of this therapy.
Although expensive, chronic baclofen infu-
sion makes it possible to personalise drugdosages and infusion programmes: this flexibil-
Fig. 3 - Graph showing the Self Reported Pain score
ity can be exploited to improve walking ability
before treatment and at follow ups (the horizontal linesindicate standard deviation).
in ambulatory patients; moreover, in the pres-ence of somatic and neuropathic pain due tospinal lesions a mixture of drugs (baclofen andmorphine for example) can be intrathecally ad-ministered.
In fact, baclofen is an agonist of the GABA-
B receptor and reduction of neuropathic pain hasbeen reported (13).
In two of our patients suffering from a ver-
tebral fracture, a mixture of morphine and ba-clofen resolved the back pain completely, yetour results in cases of neuropathic pain werenot so satisfactory (14), showing wide diff e r-ences among patients (Fig. 3).
In conclusion, we believe that the positive
clinical results obtained following applicationof this technique should also be evaluatedthrough functional assessment and in terms oflife support tools in an attempt to determine theexact social cost-benefit ratio of this therapy.
Fig. 4 - Graph showing the average score of FIM motoritems before treatment and at last follow up.
Legend: A = eating; B = grooming; C = bathing; D =dressing upper body; E = dressing lower body; F = toile-
11. Penn RD. Intrathecal baclofen for spastici-
ting; G = bladder management; H = bowel management;
ty of spinal origin: seven years of experi-
I = bed, chair transfer; J = toilet transfer; K = tub, showertransfer; L = walking, wheelchair; M = stairs.
Functional improvement after intrathecal baclofen
12. C o ffey RJ, Cahill D, Steers W et al. Intrathe-
cal baclofen for intractable spasticity of
spinal origin: results of a long-term multi-
center study. J Neurosurg 1993;78:226-232
13. Middel B, Kuipers-Upmeijer H, Bouma J
19. Landau WM. Parables of palsy pills and
et al. Effect of intrathecal baclofen deliv-
PT pedagogy: a spastic dialectic. Neurolo-
on health related quality of life in patients
10. Parke B, Penn RD, Savoy SM, Corcos D.
with severe spasticity. J Neurol Neurosurg
14. Azouvi P, Mane M, Thiebaut JB, Denys P,
11. Lazorthes Y, Sallerin-Caute B, Verdie JC,
clofen administration for control of severe
Bastide R, Carillo JP. Chronic intrathecal
spinal spasticity: functional improvement
baclofen administration for control of severe
s p a s t i c i t y. J Neurosurg 1990;72:393-402
12. Gerszten PC, Albright AL, Barry MJ. Ef-
15. Ashworth B. Trial of carisoprodal in multi-
fect on ambulation of continuous intrathe-
ple sclerosis. Practioner 1964;192:540-542
16. Penn RD, Savoy SM, Corcos D et al. In-
trathecal baclofen for severe spinal spas-
13. Herman RM, D’Luzansky SC, Ippolito R.
17. Granger CV, Hamilton BB. UDS report. The
pain in patients with spinal lesions. A pilot
uniform data system for medical rehabilita-
tion report of first admissions for 1990. Am
14. Loubser PG, Akman NM. Effects of intrathe-
cal baclofen on chronic spinal cord injury
Physician and Pharmacist Reference Guide Preferred Choice The CVS Caremark Preferred Choice 3-Tier Formulary, formerly the PharmaCare Preferred Choice 3-Tier Formulary , is a guide within select therapeutic categories for clients, plan participants and health care providers. Generics should be considered the first line of prescribing. If there is no generic available, there may be more tha
Definitionen • Meningitis – (sub-)akute Infektion der Hirnhäute (Meningen) – meist durch Bakterien (selten Pilze oder Protozoen)– die im Rahmen einer allgemeinen Infektion mit dem – aus benachbarten Entzündungen (Sinusitis, Infektion nach Piercing am Kopf) fortgeleitet sind oder– von außen (Operation, Verletzung) ins ZNS gelangen• Herpesencephalitis – Entzündung d
 Functional improvement after intrathecal baclofen
t r a r y, the improvement seen in the patients withtetraparesis was only slight.
Functional improvement after intrathecal baclofen
t r a r y, the improvement seen in the patients withtetraparesis was only slight.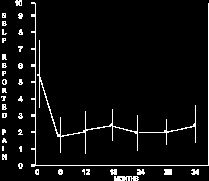
 vidual FIM motor items but mainly in bathing,dressing the lower body and transferring thebody (Fig. 4). In this study the functional re-sults obtained did not differ between spinalcord injury and multiple sclerosis patients, butthese findings could be due to what was, in re-lation to the progressive worsening that occursin multiple sclerosis, a relatively short follow-up time (11).
vidual FIM motor items but mainly in bathing,dressing the lower body and transferring thebody (Fig. 4). In this study the functional re-sults obtained did not differ between spinalcord injury and multiple sclerosis patients, butthese findings could be due to what was, in re-lation to the progressive worsening that occursin multiple sclerosis, a relatively short follow-up time (11).