Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Bruxismo.eu
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder: a pilot study Ghadah A. Malki* / Khalid H. Zawawi** / Marcello Melis*** / Christopher V. Hughes**** The objective of this study was to evaluate reported bruxism among children affected by attentiondeficit hyperactivity disorder (ADHD). Thirty children diagnosed with ADHD and 30 healthy age andgender matched controls participated in the study. All subjects were examined for dental attrition, andthe parents were asked for signs and symptoms of bruxism in their children using a questionnaire. Prevalence of oral parafunction was evaluated comparing ADHD children taking medications,ADHD children not taking medications, and controls. Subjects affected by ADHD and pharmaco-logically treated showed higher occurrence of bruxism compared to subjects affected by ADHD nottaking medicines and controls; and within the ADHD group taking medications, CNS-stimulants havebeen associated with such side effect more frequently than the other drugs.INTRODUCTION
4. Non-rapid eye movement (NREM) parasomnias
Attention-deficit-hyperactivity disorder (ADHD) e.g. sleep walking and sleep terrors. Most of the
sleep research in ADHD has focused on dys-
characterized by developmentally inappropriate
somnias and sleep related involuntary movements.
hyperactivity, impulsivity, and inattention. Prevalence in
However, as it was concluded that the association
the population has been reported to range from 1.7% to
between ADHD and sleep problems is intricate,
17.8%. Substantial clinical evidence shows an association
and treatment with stimulant medications can be a
between sleep problems and ADHD in children. Sleep
disorders in children are not a unitary clinical problem. They are commonly classified in the following groups:
Psychostimulant drugs are the treatment of choice
for children with ADHD. There is often an immediate
1. Dyssomnias e.g. insomnia and circadian rhythm
and dramatic improvement in the conduct and acad-
emic performance of children with behavioral distur-
2. Sleep-related involuntary movements e.g. bruxism,
bances after administration of the medication. These
periodic limb movement disorder and sleep talking,
findings have been long-established by many
3. Sleep-related breathing disorders e.g. obstructive
controlled short-term clinical studies of children,
adolescents, and adults; an estimated 70% of thesubjects responded to methylphenidate, dextro-amphetamine, and pemoline, eliminating mostdebate over at least the short-term efficacy andsafety of these drugs. Gillberg et al.9 reported similar
* Ghadah A. Malki, BDS, DScD, Pediatric Dentist, Dental
Center, King Fahad Hospital. Jeddah, Saudi Arabia.
findings in a recent long-term study, although in a
** Khalid H. Zawawi, BDS, Postdoctoral Resident, Department of
Oral Biology, Goldman School of Dental Medicine, Boston
Bruxism has been associated with sleep disorders and
has been reported to be aggravated by the consumption
*** Marcello Melis, DMD, Rpharm, Private Practice, Cagliari, Italy.
of alcohol and some types of medications, it has also
**** Christopher V. Hughes, DMD, PhD, Department of Pediatric
Dentistry, Goldman School of Dental Medicine, Boston
been observed in individuals with disturbances of the
central nervous system. Bruxism is defined by theAmerican Academy of Orofacial Pain as: “A diurnal or
Send all correspondence to Khalid H. Zawawi, BDS, Department ofOral Biology, Goldman School of Dental Medicine, Boston
nocturnal parafunctional activity including clenching,
University, 100 East Newton Street, Room # G-05, Boston, MA 02118.
bracing, gnashing and grinding of the teeth”. TheAmerican Sleep Disorders Association defines bruxism
as: “Tooth grinding or clenching during sleep plus one of
the following: tooth wear, sounds or jaw muscle
The Journal of Clinical Pediatric Dentistry
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
discomfort in the absence of a medical disorder”.
7. Does you child experience morning headaches?
Bruxism affects 15% to 100% of the population andseems to be related to local/mechanical factors,
Subjects were also examined for signs of dental wear
systemic/neurological factors and psychological factors.
(i.e. attrition, erosions and occlusal wear facets) and the
The role of stress in the pathophysiology of bruxism
severity and number of worn teeth was recorded. To
is anecdotal, yet it is probably the factor to which most
control for intra/inter examiner consistency, one exam-
often the etiology of oral parafunctions is attributed.
iner performed the dental examinations.
Some investigators have suggested that bruxing is infact a type of sleep disorder and is linked to dreaming
STATISTICAL ANALYSES
during sleep cycles, daytime emotional expression,
For nominal data Chi square (2) analysis was per-
anxiety induced responses, or the anticipation of stress-
formed to evaluate whether a statistical relationship
exists between the groups. ANOVA was used to com-
Bruxism can result in excessive tooth wear, muscular
pare significant differences among the three groups for
pain, degenerative temporomandibular joint disease,
the number of worn teeth, followed by pair wise com-
muscular hypertrophy, headache and periodontal tissue
parisons. Dunnett-T3 correction method was used to
injury. While tooth wear is visible to the dentist, the
correct for type-I error. Regression analysis was used to
effects of bruxism on the orofacial muscles, ligaments
assess the relationship between the use of medications
and joints are not easily recognized; nonetheless, they
and tooth attrition. Fisher’s exact test and Student’s
are often painful for the patient and have serious long
t-test were used where appropriate. Data are presented
as mean ± standard error of the mean (SEM). Analyseswere conducted using the Statistical Package for the
STUDY OBJECTIVES
Social Sciences (SPSS Inc, Chicago, IL).
The objective of this study was to investigate bruxismin subjects diagnosed with ADHD, and evaluate the
relationship between bruxism and the medications
A total of 60 subjects (48 males and 12 females) were
enrolled in the study, 30 diagnosed with ADHD (meanage 10.6±0.5) and 30 controls (mean age 10±0.4). MATERIALS AND METHODS
The results of the questionnaire showed that ADHD
Patients seeking dental treatment attending the
subjects reported more grinding during the day (2 = 10.4,
outpatient dental clinic at Franciscan Children’s
p=0.002), more clenching or grinding during sleep
Hospital were asked to participate in the study. All
(2 = 6.2, p=0.025) and the parent/guardian felt that the
young patients between the age of 5 years to 15 years,
subject’s teeth are getting worn down more frequently
and diagnosed with ADHD were recruited. Thirty
when compared to the control group (2 = 11.9, p=0.001).
patients were diagnosed with ADHD, 24 subjects were
No significant differences were observed for the remaining
receiving medications for ADHD and 6 were not
questions investigating morning headaches, face pain, jaw
receiving medications at the time of the interview and
clicking and face pain during the night (p>0.05) (Table 1).
examination. The diagnosis of ADHD was based on
When evaluating the number of teeth with attrition/
medical history. Thirty age and gender matched healthy
wear facets between the groups, independent Student’s
children attending the dental office for regular treat-
t-test showed that ADHD subjects had more teeth with
attrition/wear facets than controls, mean = 6.1±1.2 and
The study was reviewed and approved by the
Institutional Review Board at Franciscan Children’s
Since 6 subjects in the ADHD group were not on
Hospital. After an informed consent was obtained,
medication, the ADHD group was further divided into
parents/guardians were asked to answer “Yes or No”
two groups, ADHD receiving medications and ADHD
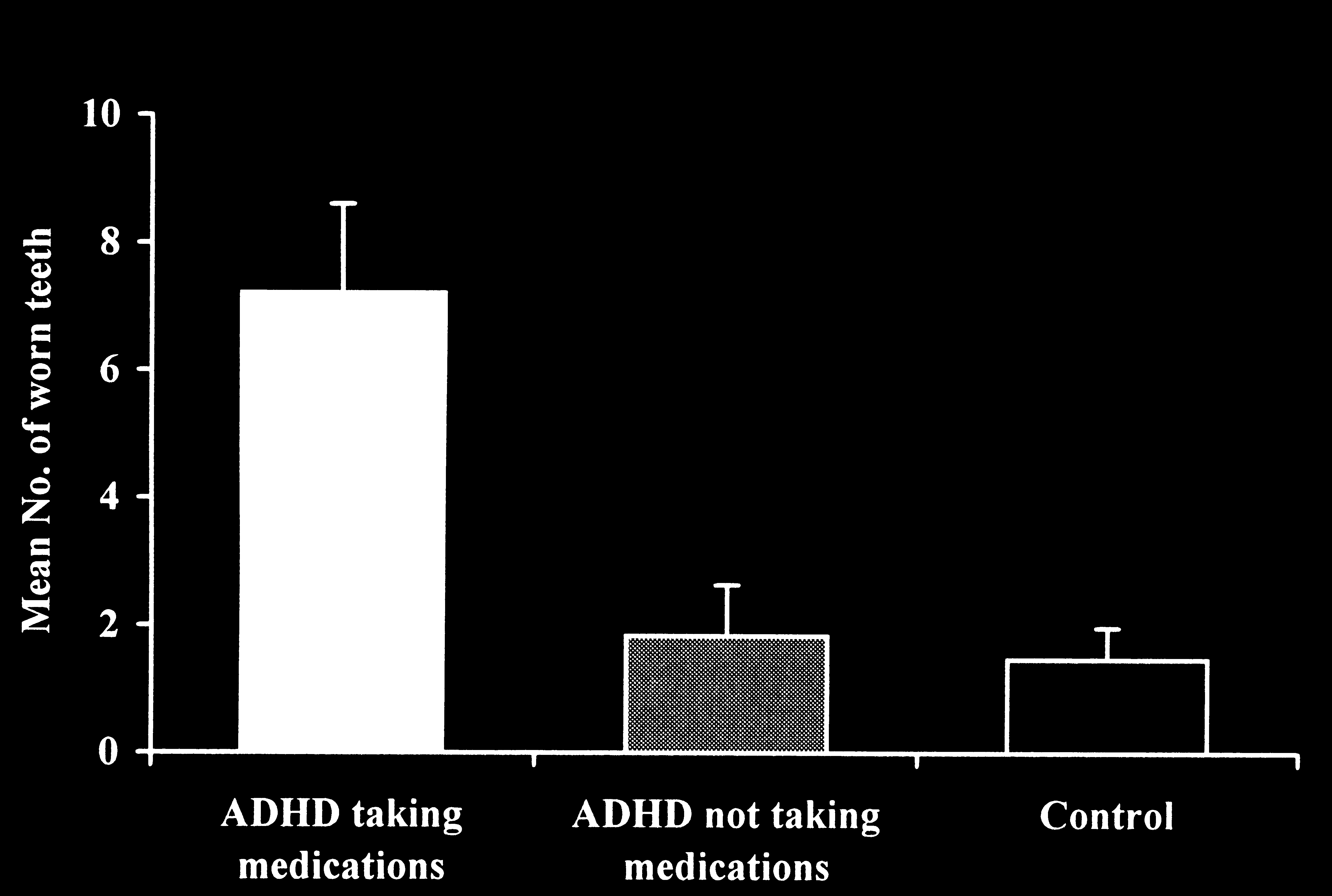
ANOVA was conducted to evaluate significant dif-
1. Does your child clench or grind his/her teeth during
ferences between the numbers of worn teeth (teeth
with attrition/wear facets) among the three groups
2. Does your child clench or grind his/her teeth during
(ADHD receiving medications, ADHD not receiving
medications and controls). There was a significant dif-
3. Do you feel that his/her teeth are getting worn
ference between the groups (Fdf = 2, 56, = 10.0,
p<0.0001). Follow-up tests were conducted to evaluate
4. Does he/she experience jaw clicking while eating,
pair wise differences among the means. ADHD chil-
dren receiving medications had a significant higher
number of worn teeth (mean=7.2±1.4) compared to
6. Does your child wake up in the middle of the night
ADHD children not receiving medications (mean =
1.8±0.8) and controls (mean=1.5±0.5), p=0.008 and
The Journal of Clinical Pediatric Dentistry
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
Table 1. Results of the chi-square tests (2) for the answers to the questionnaire given to the Parents/guardians. Does your child clench or grind his/her teeth during the day? Does your child clench or grind his/her teeth during sleep? Do you feel that his/her teeth are getting worn down? Does he/she experience jaw clicking while eating, yawing or any other movements? Does he/she complain of facial pain? Does your child wake up in the middle of the night complaining of facial pain? Does you child experience morning headaches?
Values are number of subjects who answered yes and percentage. NS indicates not significant
Table 2. Summary of the medications used by the ADHD subjects during the interview. Medication Class No. of Subjects (percentage) Total percentage
Selective Serotonin Reuptake Inhibitors (SSRI’s)
␣ Adrenergic Blockers
p=0.002, respectively. The difference between the
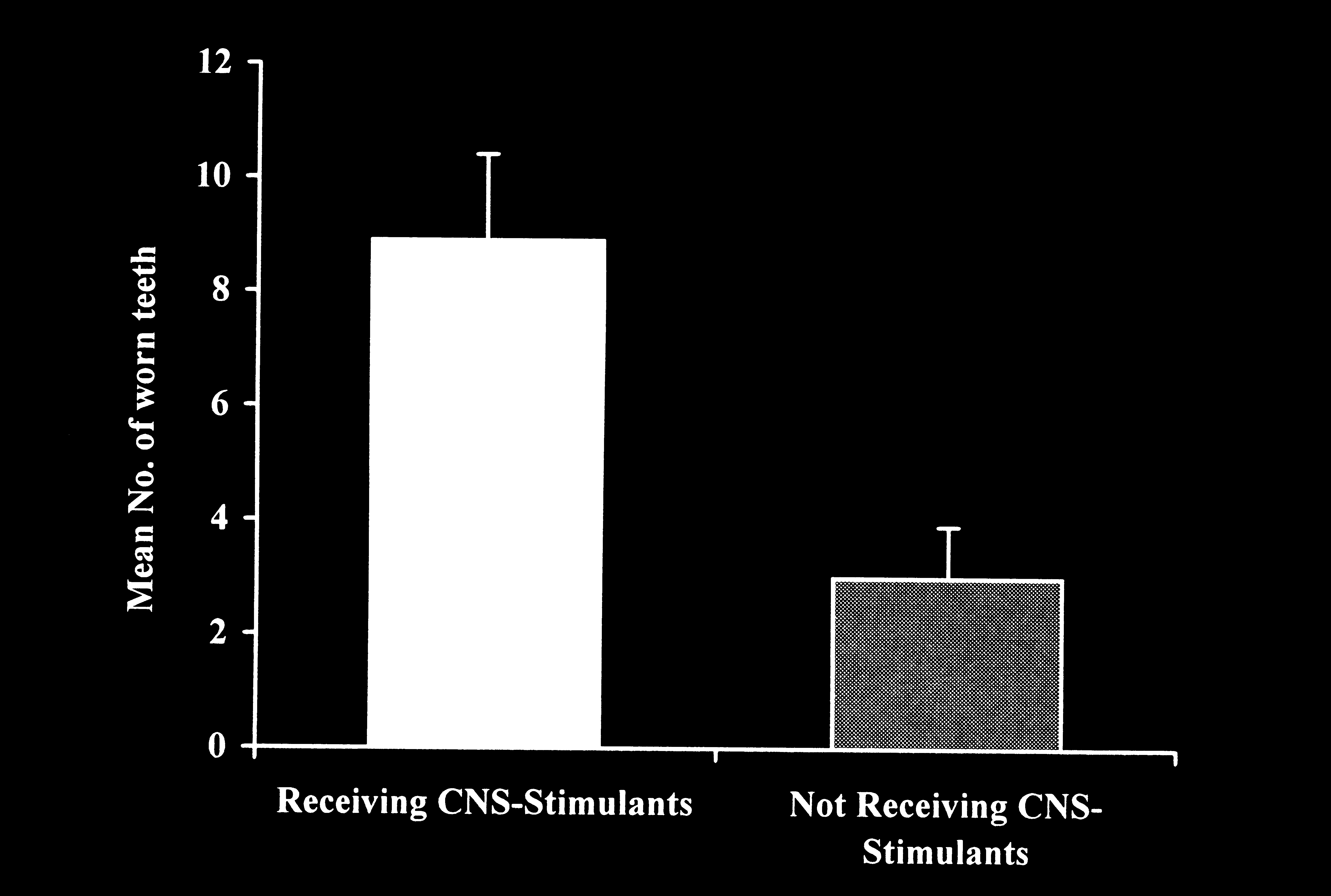
Regression analysis was conducted using the num-
number of worn teeth for the ADHD children not
ber of worn teeth as the dependant variable. The results
receiving medications was not significantly different
showed that there was a significant association between
from the controls (p>0.1) (Figure 1).
the use of CNS-stimulants (e.g. methylphenidate,
Since ADHD subjects receiving medications
amphetamines) and tooth wear (p<0.05). Moreover,
exhibited significantly higher number of worn teeth
subjects receiving CNS-Stimulants had more teeth with
compared to the other two groups, it was of interest
attrition (mean = 8.9±1.5) compared to subjects not
to find which medication could be associated with
using these medications (mean = 3.0 (0.9), t
The Journal of Clinical Pediatric Dentistry
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
Figure 1. Comparison between the number of worn teeth for the Figure 2. Comparisons between the mean number of worn teeth
ADHD children receiving medications, ADHD children not receiving
for Subjects receiving CNS-stimulants and subjects who do not in
the ADHD group receiving medications. DISCUSSION
ADHD children receiving medications had higher
In 1993, the number of prescriptions in the United
prevalence of tooth attrition and more daytime grind-
States for methylphenidate (a CNS-stimulant) for chil-
ing, we compared ADHD children using CNS-stimu-
dren with ADHD was 2.5 times higher than in 1990.
lants to children using other medications, and a signifi-
This increase aroused concern about abuse or over
cant difference was found: children using CNS-stimu-
prescribing. These stimulants cause muscular hyperac-
lants had a 2.5-fold higher number of worn teeth.
tivity and dyskinesia. Nonetheless, the value of stimu-
The results of this study seem to agree with the pre-
lant drugs in reducing symptoms of ADHD is widely
viously reported studies where occurrence of bruxism
accepted. The value in children with relatively mild
was noticed after administration of SSRIs and antipsy-
symptoms or with coexisting disorders is less clear. The
chotic drugs. Also another study showed the marked
drugs can be safely administered to children with
effect of methylphenidate on oral parafunctions,
ADHD and epilepsy and methylphenidate, but not
although associated to valproic acid for the treatment
dextroamphetamine, gives positive results in children
of ADHD and epilepsy, confirming what was observed
with ADHD and tic disorders decreasing disruptive
in the present study. On the other hand, whether the
behavior without necessarily worsening the tics.
use of ADHD medications is the cause of such symp-
Selective serotonin reuptake inhibitors (SSRIs) are
toms cannot be confirmed because of some limitations
also medicines used for the treatment of ADHD. They
of the study. One limitation is due to the fact that we
are widely prescribed anti-depressants that enhance
did not evaluate the effect of different dosages of each
serotonin neurotransmission. The use of SSRIs has
medication on bruxism. The use of higher or lower dose
been associated with the occurrence or worsening of
of the drug administered might have biased the results
several extra-pyramidal reactions such as dyskinesia,
of the comparison between methylphenidate and the
restless leg syndrome, dystonia and bruxism. Fitzgerald
other medicines. Table 2 summarizes the medications
and Healy observed diurnal bruxism secondary to
used by the ADHD subjects included in the study and
SSRI medication in 5 of 6 patients. Bruxism persisted in
the percentage of subjects using each drug.
2 of the patients after the drug was discontinued. Also
The second limitation consists in the small number
Amir et al.33 found acute bruxism and akathisia occur-
of ADHD children not receiving medications, only six
ring as an early side effect of antipsychotic drug for the
children, making a clear association between ADHD
children taking medications and bruxism difficult. This
The present study evaluated the possible parafunc-
limited number of ADHD children not treated with
tional habits among children diagnosed with ADHD
medicines could be attributed to the fact that these
especially the ones receiving medications for this disor-
children are put on medications as soon as they are
der. It was also found that there was a higher preva-
lence of day and night grinding among the ADHD chil-
The present report suggests that there could be an
dren treated with medication when compared to the
association between ADHD medications and parafunc-
other two groups. When evaluating the number of worn
tional activity, especially focusing on the use of CNS-
teeth it was found that the ADHD group receiving
stimulants (e.g. methylphenidate or amphetamines). This
medications had significantly more signs of attrition
association could be further established by increasing the
compared to the other two groups. After realizing that
sample size, especially in the ADHD group, who do not
The Journal of Clinical Pediatric Dentistry
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
receive medications, and controlling for the type of med-
14. Melis M, Abou-Atme YS. Prevalence of bruxism awareness in a
ication used and the different dosages. This would give a
Sardinian population. Cranio 21: 144-51, 2003.
15. Glaros AG, Rao SM. Bruxism: a critical review. Psychol Bull 84:
clearer picture of the eventual associations and improve
the discriminating power of the statistical analyses. How-
16. Okeson JP. Etiology of functional disturbances in the mastica-
ever, although oral parafunctional activities are common
tory system. In: Okeson JP, ed. Management of temporo-
occurrences and vary with each individual, in some
mandibular disorders and occlusion. 4th ed. St. Louis: Mosby
patients enrolled in the study they were extremely
17. Pierce CJ, Chrisman K, Bennett ME, Close JM. Stress, anticipa-
destructive and resulted in extremely frustrating prob-
tory stress, and psychologic measures related to sleep bruxism.
lems for the dentist. It is therefore appropriate not to
overlook the problem, regularly examining ADHD
18. Goulet JP, Lund JP, Montplaisir JY, Lavigne GJ. Daily clenching,
patients, especially those taking medications and in par-
nocturnal bruxism and stress and their association with TMD
ticular CNS-stimulants, and eventually intervening to
symptoms [abstract]. J Orofac Pain 75: 120, 1993.
19. Westrup DA, Keller SR, Nellis TA, Hicks RA. Arousability and
avoid damage to the oral structures.
bruxism in male and female college students. Percept Mot Skills75(3 Pt 1): 796-8, 1992. REFERENCES
20. Hicks RA, Conti P. Nocturnal bruxism and self reports of stress-
1. Diagnostic and statistical manual of mental disorders: DSM-IV
related symptoms. Percept Mot Skills 72(3 Pt 2): 1182, 1991.
Washington, D.C.: American Psychiatric Publishing, Incorporated;
21. Rugh JD, and Solberg WK. Psychological implications in tempo-
1994. (First MBa, Pincus HA, eds. Diagnostic and Statistical
romandibular pain and dysfunction. In: Zarb GA, and Carlsson
GE, eds. Temporomandibular joint function and dysfunction.
2. Taylor EA, et al. Hyperkinetic disorders: prevalence, definition
Copenhagen: Munksgaard, p. 255, 1979.
and association. In: Eric A. Taylor, et al. eds. The epidemiology of
22. Faulkner KD. Bruxism: a review of the literature. Part I [see
childhood hyperactivity. Oxford, England: Oxford university
comments]. Aust Dent J 35: 266-76, 1990.
23. Cannistraci AJ, Friedrich JA. A multidimensional approach to
3. Baumgaertel A, Wolraich ML, Dietrich M. Comparison of diag-
bruxism and TMD. N Y State Dent J 53: 31-4, 1987.
nostic criteria for attention deficit disorders in a German
24. Rugh JD, Ohrbach R. Occlusal parafunction. In: Mohl ND, Zarb
elementary school sample. J Am Acad Child Adolesc Psychiatry
GA, Carlsson GE, and Rugh JD, eds. A textbook of occlusion.
3rd ed. Chicago, Quintessence, 249-261, 1991.
4. Owens JA, Maxim R, Nobile C, McGuinn M, Msall M. Parental
25. Swanson JM, Lerner M, Williams L. More frequent diagnosis of
and self-report of sleep in children with attention- deficit/hyper-
attention deficit-hyperactivity disorder. N Engl J Med 333: 944,
activity disorder. Arch Pediatr Adolesc Med 154: 549-55, 2000.
5. Anders TF, Eiben LA. Pediatric sleep disorders: a review of the
26. Ellsworth AJ, Witt DM, Dugdale DC, Oliver LM. Mosby's
past 10 years. J Am Acad Child Adolesc Psychiatry 36: 9-20, 1997.
medical drug reference. St. Louis, Mosby, 1999.
6. Corkum P, Moldofsky H, Hogg-Johnson S, Humphries T,
27. Gross-Tsur V, Manor O, van der Meere J, Joseph A, Shalev RS.
Tannock R. Sleep problems in children with attention-
Epilepsy and attention deficit hyperactivity disorder: is
deficit/hyperactivity disorder: impact of subtype, comorbidity,
methylphenidate safe and effective? J Pediatr 130: 670-4, 1997.
and stimulant medication. J Am Acad Child Adolesc Psychiatry
28. Castellanos FX, Giedd JN, Elia J, et al. Controlled stimulant
treatment of ADHD and comorbid Tourette's syndrome: effects
7. Pliszka SR. The use of psychostimulants in the pediatric patient.
of stimulant and dose. J Am Acad Child Adolesc Psychiatry 36:
Pediatr Clin North Am 45: 1085-98, 1998.
8. Spencer T, Biederman J, Wilens T, Harding M, O'Donnell D,
29. Gadow KD, Sverd J, Sprafkin J, Nolan EE, Ezor SN. Efficacy of
Griffin S. Pharmacotherapy of attention-deficit hyperactivity
methylphenidate for attention-deficit hyperactivity disorder in
disorder across the life cycle. J Am Acad Child Adolesc
children with tic disorder. Arch Gen Psychiatry 52: 444-55, 1995.
30. Gadow KD, Nolan E, Sprafkin J, Sverd J. School observations of
9. Gillberg C, Melander H, von Knorring AL, et al. Long-term
children with attention-deficit hyperactivity disorder and comor-
stimulant treatment of children with attention-deficit hyper-
bid tic disorder: effects of methylphenidate treatment. J Dev
activity disorder symptoms. A randomized, double-blind,
placebo-controlled trial. Arch Gen Psychiatry 54: 857-64, 1997.
31. Lobbezoo F, van Denderen RJ, Verheij JG, Naeije M. Reports of
10. Attanasio R. An overview of bruxism and its management. Dent
SSRI-Associated Bruxism in the Family Physician's Office.
11. Okeson JP. Orofacial Pain: Guidelines for assessment, diagnosis
32. Fitzgerald K, Healy D. Dystonias and dyskinesias of the jaw asso-
and management Chicago, Quintessence Publishing, 1996.
ciated with the use of SSRis. Hum Psychopharmacol 10: 215-219,
12. Thorpy MJ. Diagnostic classification steering committee.
In: Association ASD, ed. The International Classification of
33. Amir I, Hermesh H, Gavish A. Bruxism secondary to antipsy-
Sleep Disorders: Diagnostic & Coding Manual. Rochester, MN,
chotic drug exposure: a positive response to propranolol. Clin
13. Seligman DA, Pullinger AG, Solberg WK. The prevalence of den-
34. Gara L, Roberts W. Adverse response to methylphenidate in com-
tal attrition and its association with factors of age, gender, occlu-
bination with valproic acid. J Child Adolesc Psychopharmacol 10:
sion, and TMJ symptomatology. J Dent Res 67: 1323-33, 1988.
The Journal of Clinical Pediatric Dentistry
The Journal of Clinical Pediatric Dentistry
LETTERS TO THE EDITOR UNDERTREATMENT OF CARDIOVASCULAR DISEASE IN ETHNICALLY DIVERSE OLDER ADULTS: WHO SHOULD RECEIVE AN ELECTROCARDIOGRAM? To the Editor: There is an increased prevalence of cardio-vascular disease and its associated risk factors such as hy-pertension in older African Americans and probably otherethnic groups as well.1,2 Several factors likely contribute tothis increas
School _________________________________ Grade_______ Teacher ___________________________ Birthdate _______________ SS# ____________ LAS CRUCES PUBLIC SCHOOLS – MEDICAL REFERRAL CARD __________________________________________________________________________________________________________________________________ Father’s Name ____________________________________________________________
 Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
Figure 1. Comparison between the number of worn teeth for the
Prevalence of bruxism in children receiving treatment for attention deficit hyperactivity disorder
Figure 1. Comparison between the number of worn teeth for the