Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Jgs49258
LETTERS TO THE EDITOR UNDERTREATMENT OF CARDIOVASCULAR DISEASE IN ETHNICALLY DIVERSE OLDER ADULTS: WHO SHOULD RECEIVE AN ELECTROCARDIOGRAM? To the Editor: There is an increased prevalence of cardio-vascular disease and its associated risk factors such as hy-pertension in older African Americans and probably otherethnic groups as well.1,2 Several factors likely contribute tothis increased prevalence, including genetics, environment,culture, education, socioeconomic status, and access to healthcare. However, the explanation remains incomplete.3–7 Whilescreening ethnically diverse seniors for an exercise study, weinadvertently discovered that many subjects and their doctorswere not aware of a large number of cardiovascular prob-
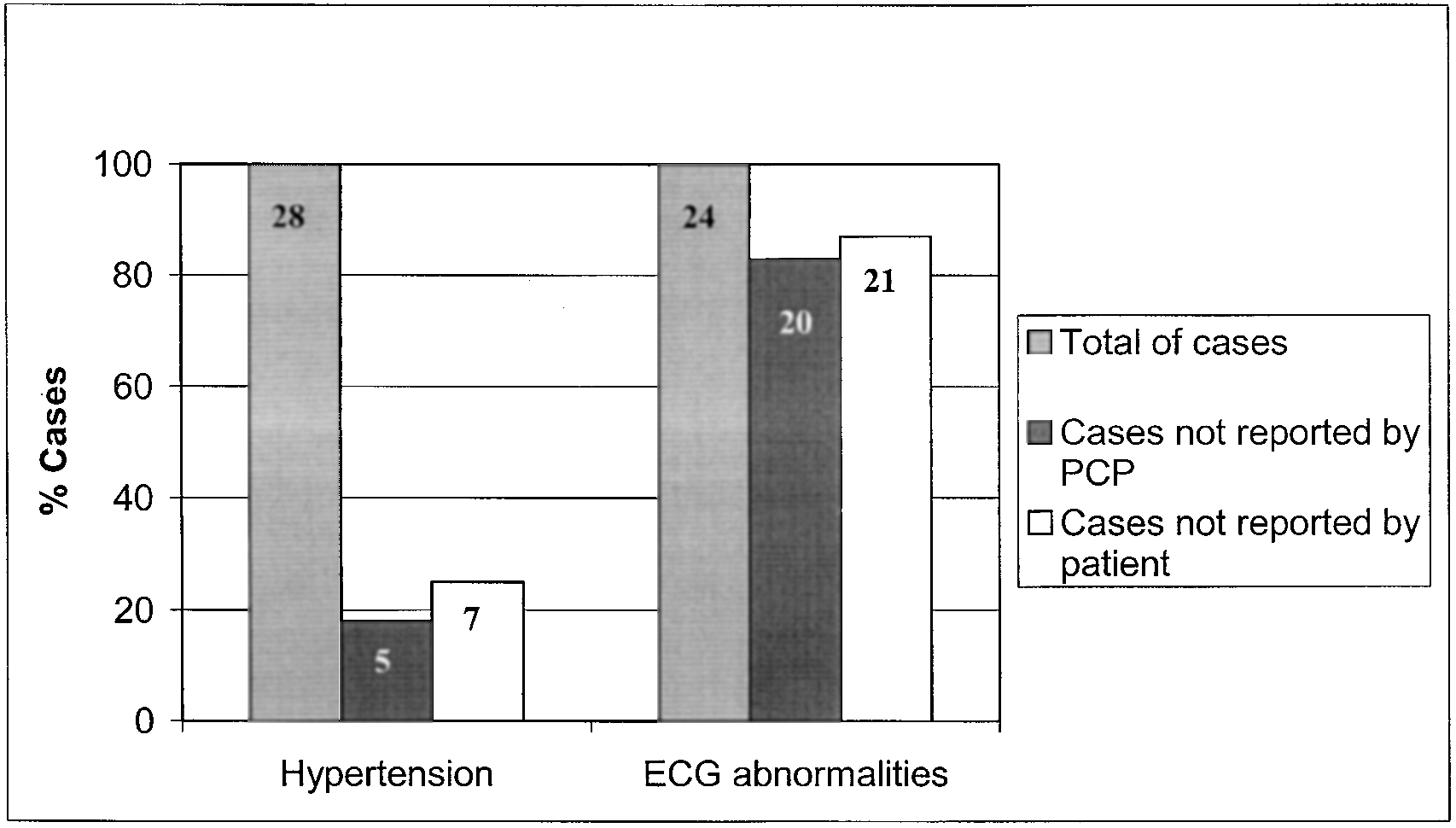
Figure 1. Undetected and unreported cardiovascular abnormali-
lems. Perhaps this finding can help to shed light on the high
ties. The subjects did not report more than 80% of the cases of
rate of cardiovascular morbidity and mortality in older mi-
electrocardiogram (ECG) abnormalities. This appears to have
been largely a result of the physicians’ failure to test for the
More specifically, we studied 36 older adults (mean
presence of ECG changes. Note that all subjects received writ-
age Ϯ standard deviation: 71.1 Ϯ 6.6 years; 21 women)
ten clearance by their PCP to participate in an aggressive exer-
who received written permission from their primary care
physician (PCP) to participate in an “aggressive” exerciseprogram at a multicultural senior center in Dorchester,Massachusetts. Center participants typically have a lower
The subjects or their PCP did not report more than 80% of
socioeconomic status and are predominately of non-Euro-
the cases of ECG abnormalities. This appears to have been
pean ancestry. Thirty of the 36 the subjects we studied did
largely a result of the physician’s failure to test for (or at
not speak English and 28 could not read or write. Thirty-
least report) the presence of ECG changes. In contrast to
three were not European American. Interpreters were used
the recommendations of the PCPs, based on our measures,
to communicate with the participants.
the study physician permitted only 19 of the 36 subjects to
The PCP of each eligible subject was asked, in writing,
whether their patient was an appropriate candidate for a
The benefits of an ECG are well known, yet our find-
vigorous exercise program and to report on their patient’s
ings raise a potentially important question: why does it
medical history and whether they had any cardiac con-
appear that the ECG is underutilized in older minorities?
cerns. We acquired a medical history, performed an electro-
There are no firm guidelines recommending when older
cardiogram (ECG), and measured blood pressure. A cardiol-
adults should have an ECG performed even though the yield
ogist who had no knowledge of the PCP’s report reviewed
of irregular ECGs is very high, the cost is relatively low, and,
the ECG. ECG abnormalities noted included ischemia, atrial
often, proven therapeutic interventions are at hand. Among
fibrillation, left ventricular hypertrophy, and atrioventricular-
this group, high-cost cardiac interventions are also underuti-
lized.4,5 This situation contrasts dramatically with the recom-
Of the 36 subjects, 24 had an ECG abnormality. In
mendation for other age-associated diseases. For example,
the 24 subjects with ECG abnormalities, the primary care
for osteoporosis screening, bone densitometry scans are
physician or the patients themselves reported cardiac prob-
recommended for all persons age 65 and older. Although
lems in four instances (16%). Twenty-eight subjects had
very important to the health of older people, these tests are
hypertension, but only 23 had received a prescription for
relatively costly, and, when an abnormality is detected, the
antihypertensive medication. Of the 23 subjects on antihy-
treatment is expensive and requires long-term therapy to
pertensive drugs, 13 still did not have controlled hyperten-
achieve only modest gains. Perhaps similar guidelines for
sion. Hypertension and ECG abnormalities are summarized
ECG evaluation in older adults, especially those who are
in Table 1 and Figure 1. By definition, all subjects had a PCP.
not fluent in English, would help to reduce the relatively high
Table 1. Undertreated and Undetected Cardiovascular Abnormalities
Total cardiovascular abnormalities detected
CAD ϭ coronary artery disease; MI ϭ myocardial infarction; ECG ϭ electrocardiogram. LETTERS TO THE EDITOR
degree of cardiovascular morbidity and mortality among
tients are especially at risk, presumably because of impaired
adaptive and autoregulation functions. To prevent FDH, it
These preliminary findings highlight the problem of
is advised to stop diuretics for 24 to 48 hours and to give a
the underdiagnosis and undertreatment of hypertension
low dose of 6.25 mg captopril or 2.5 mg enalapril. How-
and ECG abnormalities in older minorities. Future studies
ever, in older people, a delicate treatment equilibrium often
are needed to further assess the role of education, accultur-
exists, and discontinuation of diuretics is not always possi-
ation, and socioeconomic status as they affect the care of
ble. In general practice, the advice to stop diuretics is not
older minorities. Further examination of the efficacy, util-
always followed up.4 Clinically relevant differences be-
ity, and cost-effectiveness of more widespread testing of
tween ACE inhibitors in the magnitude of FDH might ex-
the ECG is needed in older adults, especially among ethni-
ist. Studies showed that perindopril caused less FDH than
cally diverse seniors, where the barriers of language and
did captopril, enalapril, or lisinopril.5–7
culture may also exacerbate the difficulty of obtaining ac-
We studied 10 patients age 70 and older with chronic sta-
curate self-reporting. It would appear that the ECG is an
ble heart failure and proven severe FDH, defined as a decrease
invaluable but underutilized tool for assessing cardiovas-
of mean arterial blood pressure (MAP) Ͼ25 mmHg, after
cular risk among older minorities, many of whom may not
6.25 mg captopril. A consent was obtained from each patient.
speak fluent English and may be illiterate. To help reduce
Blood pressure was measured supine with an automatic
cardiac morbidity and mortality, perhaps it would be ap-
ambulatory device (Spacelab®, SpaceLabs, Inc., Working-
propriate to enact a national guideline that calls for yearly
ham, Beckshire, England) every 15 minutes from 8 a.m. on
for 5 hours and in sitting position every hour for the next 8hours. During the whole study period, patients were closely
monitored for clinical signs of FDH. Blood pressure was
measured on 3 different days: at baseline; the following day,
receiving 6.25 mg captopril at 9 a.m.; and, in the case of se-
vere FDH, receiving 2 mg perindopril at 9 a.m. after a 3-day
washout period. All other drugs, including diuretics, were
Gerontology Division and Department of Medicine
not changed from 72 hours before the study until the end
Beth Israel Deaconess Medical Center
of the study period. The difference between the lowest MAP
Division on Aging, Harvard Medical School
measured in the hour before captopril or perindopril and the
lowest of 24 MAPs measured within 12 hours after captoprilor perindopril was calculated. The differences in blood pres-
REFERENCES
sure reduction after captopril and perindopril were tested
1. Scirica BM, Moliterno DJ, Every NR et al. Racial differences in the manage-
with Wilcoxon signed rank test. Effects with a P-value Ͻ
ment of unstable angina: Results from the multicenter GUARANTEE registry. Am Heart J 1999;138:1065–1072.
2. Bone LR, Hill MN, Stallings R et al. Community health survey in an urban Af-
Of 25 patients, 10 (mean Ϯ standard deviation (SD)
rican-American neighborhood: Distribution and correlates of elevated blood
age 84 Ϯ 6 years) suffered a blood pressure reduction of
Ͼ25 mmHg MAP after 6.25 mg captopril. No differences
3. Ontiveros JA, Black SA, Jakobi PL et al. Ethnic variation in attitudes toward
hypertension in adults ages 75 and older. Prev Med 1999;29:443–449.
were found for age, gender, serum creatinine level, or New
4. Carlisle DM, Leake BD, Shapiro MF. Racial and ethnic differences in the use of
York Heart Association class between patients with and
invasive cardiac procedures among cardiac patients in Los Angeles County,
without severe FDH. The 10 patients with severe FDH
1986 through 1988. Am J Public Health 1995;85:352–356.
used at mean a lower dose of furosemide (44 Ϯ 13 mg)
5. Schulman KA, Berlin JA, Harless W et al. The effect of race and sex on physi-
cians’ recommendations for cardiac catheterization. N Engl J Med 1999;340:
than did the 15 patients without severe FDH (77 Ϯ 53 mg).
The mean Ϯ SD maximum fall of MAP in these 10 pa-
6. Aronow WS, Ahn C. Risk factors for new coronary events in older African-
tients was 31.3 Ϯ 4.5 mmHg (range 27–40). Two patients
American men and women. Am J Cardiol 1998;82:902–904.
became drowsy for a short period. No intervention was
7. Gregory PM, Rhoads GG, Wilson AC et al. Impact of availability of hospital-
based invasive cardiac services on racial differences in the use of these services.
needed. After the first dose of perindopril, mean Ϯ SD max-
imum fall of MAP was 18.5 Ϯ 10.6 mmHg (range 5–38)
8. Hayward MD, Heron M. Racial inequality in active life among adult Ameri-
in the 10 patients. Two patients had a fall of Ͼ25mmHg
MAP. None of the patients had symptomatic FDH. The dif-ference in blood pressure reduction after the first dose ofcaptopril and perindopril was statistically significant (P ϭ
BLOOD PRESSURE REDUCTION AFTER THE FIRST DOSE OF CAPTOPRIL AND PERINDOPRIL
Figure 1 shows the course of the MAP at baseline, af-
To the Editor: Initiation of treatment with angiotensin-con-
ter captopril, and after perindopril. On all 3 days, a marked
verting enzyme (ACE) inhibitors is frequently complicated
and comparable blood pressure reduction was present be-
by the occurrence of (sometimes severe) hypotension after
tween 8:00 a.m. and 9:00 a.m. A further blood pressure re-
the first dose. Profound hypotension, requiring termination
duction was found 1 hour after use of captopril, between
of the treatment, was present in about 5% of the patients
10:00 and 11:00 a.m. After 12:00 noon, the blood pressure–
after the first dose of 6.25 mg captopril and of 10 mg enala-
lowering effect of captopril disappeared again. Captopril
pril.1,2 First-dose hypotension (FDH) increases the risk of
was not continued after the first dose. The blood pressure re-
falls, myocardial infarction, and stroke. A positive correla-
duction caused by perindopril started gradually, 4 to 5 hours
tion between FDH and mortality was found.3 Older pa-
after the dose, and persisted until the last measurements. The
C h i r u r g i e - h e e l k u n d i g e i n g r e e p Afhankelijk van de uitgebreidheid van de weg te nemen letsels, kan dit in het kabinet tijdens een consultatie onder lokale verdoving gebeuren of in AZ ALMA (onder lokale of algemene verdoving) VERDOVING : De betreffende huidafwijking wordt eerst plaatselijk verdoofd met een injectie. Hierbij voelt u eerst een klein prikje van de i
Neue Pille für die Potenz Dem Manne kann geholfen werden Noch immer wird die erektile Dysfunktion im Volksmund derb als Impotenz bezeichnet und als Tabuthema behandelt. Die Selbstinjektion von vasoaktiven Substanzen in den Schwellkörper brachte 1982 den ersten Ansatz für eine gezielte Therapie. 1998 hat sich mit Viagra® eine kleine Revolution vollzogen. Mit Ixense® is
 LETTERS TO THE EDITOR
LETTERS TO THE EDITOR