Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Slide
SPECIFIC COMPLICATIONS DURING RETROPERITONEASCOPIC SURGERY FOR PHEOCHROMOCYTOMA
G. Todorov ,St.Toshev, B.Mioljevikj-Miserliovska, R.Miserliovski, Second Surgical Department Department of General Surgery, University Hospital „Alexandrovska”, Sofia, Bulgaria P. Tzaneva Second Surgical Department , Department of Anaesthesiology and Intensive Care, University Hospital „Alexandrovska”, Sofia, Bulgaria
CLINICAL CASE-2
A 52 years old female, who had a crisis increase in blood pressure to 170/100 in the past
Pheochromocytoma is a rare catecholamine producing tumor arising from chromaffin cells
year, accompanied by pallor, sweating, palpitations. Attacks have a duration of 10 minutes, 1-2
in the adrenal medulla or in other paraganglia of the sympathetic nervous system. Typical
times a week. Being under no attacks she had a normal to low blood pressure.
clinical findings include headache, palpitation, excessive sweating and paroxysmal hypertension. The best confirmatory test for diagnosis is to measure free catecholamines or
Ultrasonographic evidence of tumor formation with 65/40mm size in the right adrenal gland.
their degradable products in a 24 h urine collection.
Elevated levels of metanefrins in 24 hours urine, respectively metanefrin 1305ng (normal<350)
Laparoscopic removal of the tumor has gained wide popularity in recent years because of
and normetanefrin 2509 ng (normal<600) were found. After two weeks of preoperative
its clear advantages: lower consumption of analgesics, shorter hospital stay and quicker
preparation with Doxazosin 2x 0,5 mg / d she was hospitalized for surgery. During the
recovery. Adequate alfa blockade in preoperative period is of high importance in preventing
dissection of the tumor with laparoscopic technique the patient developed severe arrhythmia
life-threatening complications such as hypertensive crisis, arrhythmias, pulmonary edema,
and sudden desaturation to 80%. Cyanosis and venous stasis of the neck appeared. After the
myocardial ischemia provoked by released of high levels catecholamines while manipulating the tumor. In addition preoperative preparation may include beta-blocker with a short effect
operation in the background of persistent hypoxemia, the patient was removed in the intensive
(Esmolol) or calcium blocker (Nicardipin) .
care unit intubated , on spontaneous ventilation through a T-piece with the submission of O2, /
The operation poses serious challenges for the surgical team and especially the anesthetist
SatO2 92% /. Hemodynamic parameters were stabilized with volume expansiors and infusion
to ensure strict control and monitor maintenance of vital functions. The operation is
performed under general anesthesia with endotracheal intubation and generally takes place in two stages. In the first an hypertensive crisis and severe arrhythmias are observed due to uncontrollable levels of catecholamines released from handling the tumor. During this stage powerful, short acting vasodilators (Phentolamine, Naniprus) and antiarrhythmics are applied. After the clamping the v.centralis and the interruption of venous drainage of the tumor the operation enters into second stage of arterial hypotension. It is recommended fluid resuscitation and vasopressors. In the early postoperative period hemodynamic parameters and blood sugar are monitored. Catecholamine levels are restored to normal within a few days
Within the period of 2002 - 2012 46 pheochromocytomas were removed retroperitoneoscopically in our clinic. We present two cases, complicated with unilateral
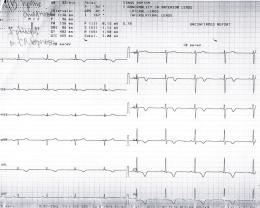
A working diagnosis of acute heart attack was made. From the X-ray - data for inhomogeneous
pulmonary edema and severe left ventical dyskinesis, described in literature as reversible
shadowing of the left lung half, with ECG evidence of negative T waves in lead I, aVL, V3-
V6. The echocardiography showed dyskinesia of the middle and top segments of the LV. EF-
35%. Laboratory evidence of elevated enzymes (CPK 543; MB 26; troponin-0, 408) was
found. In the backround of heparinoterapy and inotropic support pulmonary changes
underwent rapid reversal. The patient was extubated after seven hours the operation. The left
We performed total adrenalectomy in all of the patients.Mean operative time was 63 min
ventriculography found hypokynesis of the apex and hyper contractility of the basal segments.
(range 30-240 min). The estimated blood loss was 30 ml (range 0-550 ml). We have not
Coronary angiography excluded obstructive coronary disease. On the six day after the
established a significant dependence of the operative time on the gender (p=0.787), localization
operation after resolution of ECG changes, enzyme abnormalities and fully stabilized
of the pathological process (left or right adrenal) (p=0.615), size of the tumor lesion (p=0.460), even on BMI.Perioperative major complications for the whole series of pheochromocytoma
cases were 8.6 %,with mortality rate – 0%.
Major - 8,6%
This two clinical cases demonstrate the same complications occurred during laparoscopic
– conversion to open procedure due to intraoperative
cardiovascular instability in pheochromocytoma
Acute unilateral pulmonary edema- Possible mechanisms of occurrence are: - unilateral pulmonary edema and severe left ventrical
-Cardiogenic-based transient acute cardiac dysfunction. Ultrasonography in patients revealed
evidence of impaired contractility and reduced LVEF.
Minor – peritoneal tear, pneumoperitoneum Postoperative complications, 4.35 %
-Due to severe cardiogenic postcapilar venous spasm, abnormal alveolocapilar permeability and
- Postoperative hemorrhagia, no hemotransfusion required
severely elevated pulmocapilar hydrostatic pressure induced by high levels of catecholamines.
The position on the operating table - left lateral position in “Jackson “ position probably is an
We present two cases, complicated with unilateral pulmonary edema and severe left ventical
additional component that contributes to significant changes in pulmonary vascular pressures.
dyskinesis, described in literature as reversible Takotsubo cardiomyopathy.
Transient cardiomyopathy type Takotsubo. This syndrome is first reported in the Japanese CLINICAL CASE-1
population by Hikaru Sato et al (1) described in 1991. Clinically resembles acute miocardial
infarction(AMI), serum enzymes are mild to moderately elevated, and coronary angiography is
A 37 years old man, who in the last six years complained about a crisis increases in blood
normal. Ultrasound showed severe left ventricular dyskinesia (apical ballooning and hyper
pressure 230/105, palpitations, headache, sweating. He observed lost of weight (10kg in one
contractility of the basal segments).The image resembles a trap for octopus-"takotsubo". Within
year). Treatment with antidepressants and antihypertensive had no effect. Metanefrines in 24h
a few days to weeks changes undergo reversal with a favorable outcome. It is a rare finding,
urine were measured ten times above normal values, respectively metanefrin 3350ng (normal
although in the past decade, however, the number of published reports of patients presenting
<350) and normetanefrin 4325ng (normal <600). On CT a heterogeneous formation was found in
with this syndrome has steadily increased. Several investigations assessed the prevalence of
the right adrenal -29/36mm in size. After a 14 days preoperative preparation with Doxazosin
tako-tsubo cardiomyopathy. Serial studies reported a prevalence of 1.0–2.0% among patients
8mg / d he was admitted for elective laparoscopic adrenalectomy.
with acute coronary syndrome.There is a strong predominance of postmenopausal women.
The first part of the operation until the interruption of the venous drainage of the tumor occured
The accurate pathogenetic mechanisms has not been clearly established. Several theories have
with large variations in blood pressure and severe arrhythmias requiring discontinuation of the
been proposed: excessive sympathetic stimulation (7-13) , metabolic impairment and stunning
manipulation on the formation. To maintain hemodynamics Naniprus infusion of 3-8mg / h and
(4-6). microvascular dysfunction (14) , and low estrogen levels (15). Catecholamine surge
Lidocain 1,5 mg / min was applied. After the ligation of v centralis ,desaturation / SatO2 89-90%
definitely plays a role, but the way it affects myocardial function has not been clarified. The
/ occured, accompanied by severe hypotension in the absence of peripheral pulses, progressive
decrease of the pulse rate, strongly deformed ventricular complexes and dilated unresponsive
pupils. Despite the forced fluid resuscitation and infusion of Dopamine 8-20 g/kg/min ,the
condition progressively deteriorated The operation was aborted and cardiopulmonary
resuscitation was carried out to stabilize the hemodynamics. Pupils remain dilated and
Perioperative management of patients with pheochromocytoma is a great challenge for the
surgical team and the anaestesiologist, requiring a
After the operation the patient was transferred in intensive care unit intubated , (IPPV, FiO2 =
functions. Operative treatment should be done only in highly specialized clinics with
100%) with persistent volume substitutuion and infusion of Dopamine 15-20 g / kg / min.
experienced teams in both endocrine and laparoscopic surgery.
Cerebroprotectives , stimulation of diuresis and antithrombotic therapy were applied . 30 minutes
after admitting the patient recovered consciousness and began to execute commands.
Desaturation persisted. The left lung was completely overshadowed with decompensated
1. Sato H, Tateishi H, Uchida T, et al. Takotsubo type 1. cardiomyopathy due to multivessel spasm. In: Kodama K, Haze K, Hon M, ds. Clinical aspect of myocardial injury: fromischaemia to heart failure. Tokyo: Kagakuhyouronsya, 1990;56-64. Japanese. 2 Stollberger C, Finsterer J, Schneider B. Tako-tsubo-like left ventriculardysfunction: clinical presentation, instrumental findings, additional cardiac and non-cardiac diseases and potential pathomechanisms. Minerva Cardioangiol
acidosis and severe hypoxemia(PH 7,17; PaO2 9,14; PaCO2 6,48; BE -11,2; Sat 89%).
2005;53:139–45. 3 Ito K, Sugihara H, Kawasaki T, et al. Assessment of ampulla (takotsubo) cardiomyopathy with coronary angiography, two-dimensional echocardiography and 99mTc-tetrofosmin myocardial single photon emission computed
Ultrasonography, performed several hours later found reduced ejection fraction of 40% (baseline
tomography. Ann Nucl Med 2001;15:351–5 4. Bybee KA, Murphy J, Prasad A, Wright RS, Lerman A, Rihal CS,et al. Acute impairment of regional myocardial glucose uptake in the apical ballooning (takotsubo) syndrome. J Nucl Cardiol 2006;13:244-50. 5. Dorfman T, Aqel R, Allred J, Woodham R, Iskandrian AE. Takotsubo cardiomyopathy induced by treadmill exercise testing: An insight into the pathophysiology of transient left ventricular apical (or midventricular) ballooning in
58%), expanded volumes and dimensions of cardiac ventricle with diffuse hypokinesia. There
the absence of obstructive coronary artery disease. J Am Coll Cardiol 2007;49:1223-5 6. Ito K, Sugihara H, Kinoshita N, Azuma A, Matsubara H. Assessment of Takotsubo cardiomyopathy (transient left ventricular apical ballooning) using 99mTc-tetrofosmin, 123I-BMIPP,123I-MIBG and 99mTc-PYP myocardial SPECT. Ann Nucl Med 2005;19:435-45.
was a laboratory evidence of elevated enzymes (CPK 542; MB 35; Troponin 0,955).
7. Ueyama T, Kasamatsu K, Hano T, Yamamoto K, Tsuruo Y, Nishio I.Emotional stress induces transient left ventricular hypocontraction in the rat via activation of cardiac adrenoceptors: A possible animal model of „tako-tsubo‟ cardiomyopathy. Circ J 2002;66:712- 8. Ueyama T, Hano T, Kasamatsu K, Yamamoto K, Tsuruo Y, Nishio I. Estrogen attenuates the emotional stress-induced cardiac responses in the animal model of Tako-tsubo (Ampulla) cardiomyopathy. J Cardiovasc Pharmacol
18 hours after surgery, after the control X-ray control on which spotted shadow in the lower and
2003;42:S117-9. 9. Villareal RP, Achari A, Wilansky S, Wilson JM. Anteroapical stunning and left ventricular outflow tract obstruction. Mayo Clin Proc 2001;76:79-83. 10. Burgdorf C, von Hof K, Schunkert H, Kurowski V. Regional alterations in myocardial sympathetic innervation in patients with transient left-ventricular apical ballooning (Tako-Tsubo cardiomyopathy).J Nucl Cardiol
a smoller one in the middle lung in the left lung were establishes, and with normalized values
2008;15:65-72. 11. Akashi YJ, Barbaro G, Sakurai T, Nakazawa K, Miyake F. Cardiac autonomic imbalance in patients with reversible ventricular dysfunction takotsubo cardiomyopathy. QJM 2007;100:335-43. 12. Pavin D, Le Breton H, Daubert C. Human stress cardiomyopathy mimicking acute myocardial syndrome. Heart (Brit Cardiac Soc)1997;78:509-11.
arterial blood gas analysis with hemodynamic parameters stabilized, the patient was extubated .
13. Sato M, Fujita S, Saito A, Ikeda Y, Kitazawa H, Takahashi M, et al. Increased incidence of transient left ventricular apical ballooning(so-called „Takotsubo‟ cardiomyopathy) after the mid- Niigata Prefecture earthquake. Circ J 2006;70:947-53. 14. Kurisu S, Sato H, Kawagoe T, Ishihara M, Shimatani Y, Nishioka K, et al. Tako-tsubo-like left ventricular dysfunction with STsegment elevation: A novel cardiac syndrome mimicking acute myocardial infarction. Am Heart J
Permanent improvement of the situation in the following days was established . The patient was
2002;143:448-55. 15. Dorfman TA, Iskandrian AE, Aqel R. An unusual manifestation of Tako-tsubo cardiomyopathy. Clin Cardiol 2008;31:194-200. 16.Gautam PL, Kaul TK. Pheochromocytoma-anaesthetic considerations. J Anaesth Clin Pharmacol 2002; 18(3): 232-247.
dismissed on the fifth postoperative day after a normal X-ray control.
17. Hessel EA, London MJ. Takotsubo (stress) cardiomyopathy and the anesthesiologist: enough case reports. Let‟s try to answer some specific questions! Anesthesia-analgesia 2010; 110(3): 674-679. 18. Miyazawa I, Wada A, Sugimoto T, Nitta N, Horie M. Emerging acute unilateral pulmonary edema in a patient with pheochromocytoma. Int
Die Herzwurm-Erkrankung Eine Ursache für Herzinsuffizienz und Tachyarrhythmien? Dr. med. Manfred Doepp Der Name klingt zunächst kurios und wenig ernstzunehmend. Viele Menschen und vor allem Kardiologen haben noch nie etwas davon gehört. Daher schauen wir einmal bei Wikipedia nach. Wir finden: „Dirofilaria immitis, deutsch auch Herzwurm, ein /Nematode aus der Überf
Clarithromycin Actavis 250 mg Film-coated Tablets V007 – Safety Update (CSP Update) SUMMARY OF PRODUCT CHARACTERISTICS NAME OF THE MEDICINAL PRODUCT Clarithromcyin Actavis 250 mg Film-coated Tablets 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each film-coated tablet contains Clarithromycin 250 mg. Excipients: Contains 0.11 mg glucose per tablet For a full list of excip
 SPECIFIC COMPLICATIONS DURING
SPECIFIC COMPLICATIONS DURING