Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Valosun3.data.quonia.cz
The effects of phytoestrogen isoflavones on bone density in women:a double-blind, randomized, placebo-controlled trial1–3
Charlotte Atkinson, Juliet E Compston, Nicholas E Day, Mitch Dowsett, and Sheila A BinghamABSTRACT
for their potential bone-sparing properties. Rates of hip fracture
Background: Isoflavone phytoestrogen therapy has been pro-
in Asian populations, whose traditional diets are rich in soy, are
posed as a natural alternative to hormone replacement therapy
substantially lower than those in whites residing in the United
(HRT). HRT has a beneficial effect on bone, but few trials in
States (8). However, bone mineral density (BMD) in Asian
humans have investigated the effects of isoflavones on bone.
populations is comparable to that in white populations after
Objective: The objective of the study was to determine the effect
adjustment for height and weight (9). Nevertheless, data from
on bone density of a red clover–derived isoflavone supplement that
animal experiments provided evidence that soy protein can
provided a daily dose of 26 mg biochanin A, 16 mg formononetin,
attenuate menopausal bone loss (10, 11), and it was suggested
1 mg genistein, and 0.5 mg daidzein for 1 y. Effects on biochem-
that isoflavones in soy might be responsible for protective
ical markers of bone turnover and body composition were also
effects on bone (12). In humans, some (13–17) but not all (18)
cross-sectional studies in Asian populations reported signifi-
Design: Women aged 49–65 y (n ϭ 205) were enrolled in a
cant positive associations between soy protein or isoflavone
double-blind, randomized, placebo-controlled trial; 177 completed
intakes and BMD. Furthermore, intervention trials in humans
the trial. Bone density, body composition, bone turnover markers,
using either soy protein or isoflavone extracts generally re-
and diet were measured at baseline and after 12 mo.
ported protective effects on bone, although sample sizes were
Results: Loss of lumbar spine bone mineral content and bone
small and trials often were relatively short. In postmenopausal
mineral density was significantly (P ϭ 0.04 and P ϭ 0.03, respec-
women, consumption of soy protein providing 90 mg isofla-
tively) lower in the women taking the isoflavone supplement than
vones/d for 24 wk resulted in a significant increase in lumbar
in those taking the placebo. There were no significant treatment
spine bone mineral content (BMC) and BMD (19), and a red
effects on hip bone mineral content or bone mineral density,
clover isoflavone supplement providing 57 or 85.5 mg isofla-
markers of bone resorption, or body composition, but bone forma-
vones/d for 6 mo resulted in an increase in BMD of the
tion markers were significantly increased (P ϭ 0.04 and P ϭ 0.01
proximal radius and ulna (20). In perimenopausal women, soy
for bone-specific alkaline phosphatase and N-propeptide of colla-gen type I, respectively) in the intervention group compared with
protein that provided 80.4 mg isoflavones/d for 24 wk did not
placebo in postmenopausal women. Interactions between treatment
increase lumbar spine BMC or BMD, but it did lower the
group and menopausal status with respect to changes in other
extent of bone loss compared with that in the control group
(21). Several intervention studies reported the effects of soy
Conclusion: These data suggest that, through attenuation of bone
protein or isoflavone extracts on markers of bone turnover. In
loss, isoflavones have a potentially protective effect on the lumbar
postmenopausal women, diets rich in soyfoods resulted in
Am J Clin Nutr 2004;79:326–33.
significant increases in serum osteocalcin concentrations (22,23) and decreases in urinary N-telopeptide excretion (22). In
KEY WORDS
Isoflavones, phytoestrogens, bone density,
perimenopausal women, a 4-wk intervention with an isofla-
randomized controlled trial, body composition, estrogen and vita-
vone extract resulted in a significant reduction in the bone
1 From the MRC Biostatistics Unit, Institute of Public Health, Robinson
Way, Cambridge, United Kingdom (CA and NED); the Metabolic BoneUnit, Addenbrooke’s Hospital, Cambridge, United Kingdom (JEC); the
INTRODUCTION
Department of Biochemistry, Royal Marsden Hospital, London (MD); and
Estrogens play an important role in skeletal homeostasis, and
the MRC Dunn Human Nutrition Unit, Cambridge, United Kingdom
ovarian hormone deficiency is one of the most important risk
factors for osteoporosis. There are clear bone-related benefits
2 Supported by grants from the Food Standards Agency and the Medical
of hormone replacement therapy (HRT; 1), but compliance
Research Council; Novogen Ltd (Australia) provided the Promensil tablets
with such regimens is generally very poor (2, 3), partly as a
and provided research support (to SAB).
3 Address reprint requests to SA Bingham, Dunn Human Nutrition Unit,
result of fears about the risks of cancer (3).
Wellcome Trust/MRC Building, Hills Road, Cambridge CB2 2XY, United
Isoflavones are compounds in plant foods, particularly soy-
Kingdom. E-mail: sab@mrc-dunn.cam.ac.uk.
beans (4, 5), that are structurally similar to the mammalian
estrogens (6, 7) and that have received considerable attention
Accepted for publication August 8, 2003. Am J Clin Nutr 2004;79:326 –33. Printed in USA. 2004 American Society for Clinical Nutrition
FIGURE 1. Flow chart describing the progress of the volunteers during the trial. HRT, hormone replacement therapy. *Includes 2 women who completed
the trial but were excluded from all analyses because they had taken oral contraceptives or had been treated for alcoholism. **Includes 1 woman whocompleted the trial but was excluded from all analyses because she had taken oral contraceptives.
resorption marker pyridinoline (24), but other studies reported
response to the letter was 68% (n ϭ 781); of the responders,
little or no effect of soy protein or isoflavone supplements on
205 (18% of the women who received letters) were eligible and
markers of bone turnover in humans (25–27).
were randomly assigned to receive an isoflavone or placebo
We aimed to determine the effects of consuming a red
tablet (Figure 1). Women were not eligible to participate if
clover–derived isoflavone supplement (in a daily dose provid-
they had a personal history of breast cancer or major breast
ing 26 mg biochanin A, 16 mg formononetin, 1 mg genistein,
surgery or if they were currently taking HRT. Women who
and 0.5 mg daidzein) for 1 y on the BMC and BMD of the
expressed an interest in taking part were visited at home.
lumbar spine and hip, on biochemical markers of bone turn-
During this initial home visit, the study was explained in detail,
and all women who wished to participate were asked forwritten informed consent. A total of 205 women were ran-domly assigned to receive isoflavone or placebo tablets (Figure
SUBJECTS AND METHODS
1). Additional home visits were made after Ϸ5.5 and 11 mo on
Subjects
the study. All study procedures were approved by the Dunn
Between November 1997 and May 1999, women aged
Human Nutrition Unit Ethics Committee and the Cambridge
49–65 y were recruited from the Breast Screening Unit of
Addenbrooke’s Hospital (Cambridge, United Kingdom). The
Participants were randomly assigned to receive daily either a
primary outcome measure was breast density, and women were
red clover–derived isoflavone tablet that provided 26 mg bio-
selected for the study according to the extent of dense tissue
chanin A, 16 mg formononetin, 1 mg genistein, and 0.5 mg
seen on their most recent mammogram; mammograms from
daidzein (Promensil; Novogen Ltd, Sydney, Australia) or a
1908 women were classified according to their Wolfe pattern
placebo of identical appearance. We did not measure the isofla-
(28), and women with P2 or DY Wolfe breast patterns (ie,
vone content of the Promensil tablets in our laboratory, but an
dense breast patterns; n ϭ 1149, 60% of all mammograms
independent study showed that the manufacturer’s statements
classified) were sent a recruitment letter, which contained a
as to the quantity and type of isoflavones in the tablets were
short description of the study and a reply slip. The rate of
correct (29). Randomization was performed by using random
number generation in MICROSOFT EXCEL (version 2.2; Mi-
content (Kone autoanalyser; Jaffe method), and excretion of
crosoft Corp, Redmond, WA), and researchers and study par-
pyridinoline and deoxypyridinoline was corrected for creati-
ticipants remained blinded to the tablet allocation throughout
the study. Participants were asked to take 1 tablet/d. The codeidentifying those who had been taking the isoflavone tablets
Blood samples
and those who had been taking the placebo was broken when
Fasting blood samples were taken at baseline and 12 mo.
all participants had completed all stages of the study.
Participants were asked to refrain from eating or drinking
Urine samples
(except water) from midnight until after the sample had beentaken the following morning. A total of 35.5 mL blood was
Women were asked to make 24-h urine collections at base-
drawn at each visit, including 9.0 mL blood that was drawn into
line and 12 mo. To check compliance, women also were asked
a lithium heparin tube and 9.0 mL that was drawn into a serum
to make a 24-h urine collection at 6 mo. The completeness of
tube. The serum tube was left at room temperature for Ն1 h
all urine collections was assessed by using the p-aminobenzoic
before centrifugation to allow clotting. After centrifugation for
acid (PABA)–check test (30). Samples containing 85–110% of
10 min at 2000 rpm and 5 °C, aliquots of plasma and serum
the ingested PABA were designated satisfactory. For samples
were stored at Ϫ20 °C. Before centrifugation, Ϸ1 mL whole
with PABA recoveries of between 70% and 85%, which indi-
blood was removed from the lithium heparin tube, and DNA
cated that all tablets had been taken but that the urine collection
was extracted by using a Qiagen kit (Qiagen Ltd, Crawley,
was incomplete, the urinary excretion of isoflavones was ad-
United Kingdom) and was used for genotyping of estrogen
justed to 93% PABA recovery (31). Samples with Ͻ70%
receptor and vitamin D receptor gene polymorphisms (PvuII
recovery were designated incomplete. Samples with Ͼ110%
PABA recovery were considered unsatisfactory, because addi-
Plasma bone-specific alkaline phosphatase (bone ALP), a
tional sources of PABA (eg, a multivitamin) may have been
marker of bone formation, was measured by using the Metra kit
consumed, and an accurate determination of sample complete-
(Quidel Ltd, Oxford, United Kingdom; 35). The intraassay and
interassay CVs were 3.9% and 10.9%, respectively. Plasma
Urinary excretion of genistein, daidzein, formononetin, and
concentrations of the N-propeptide of collagen type I (PINP),
biochanin A was measured by using HPLC and a modification
also a marker of bone formation, were measured by using the
of the method of Setchell et al (32) and Franke et al (33).
Orion Diagnostica radioimmunoassay kit (Espoo, Finland; 36),
Briefly, samples were incubated with -glucuronidase for
for which the intraassay and interassay CVs were 9.3% and
20–72 h at 37 °C. Phenolic components were extracted into an
12.5%, respectively. For both assays, baseline and 12-mo sam-
ethyl:acetate (6:4 by vol) solvent mixture. After vortex mixing
ples from each participant were run together on the same plate
for 30 s and subsequent 10-min centrifugation at 2320 ϫ g and
20 °C, the organic phase was transferred to a 2-mL vial and
Serum estradiol was measured by using a previously de-
evaporated to dryness under vacuum at 43 °C. Extraction res-
scribed method (37), and serum follicle-stimulating hormone
idues were reconstituted in 100 L 50% isopropanol solution
(FSH) was measured by using an enzyme immunoassay on an
and centrifuged for 10 min at 2320 ϫ g and 20 °C. A 5-L
Abbott AxSYM automated analyzer (Abbott Diagnostics,
aliquot was then injected directly onto the HPLC column,
Maidenhead, United Kingdom). Menopausal status was deter-
which consisted of an Alltima 250 ϫ 2.1-mm, 5 mol/L, C-18
mined by using baseline concentrations of estradiol and FSH as
stationary phase (Alltech Associates, New South Wales, Aus-
follows; women were classified as premenopausal if they had
tralia), and a mobile phase (acetonitrile and water) containing
Ͻ30 IU FSH/L and Ͼ100 pmol estradiol/L, as postmenopausal
0.05% trifluoroacetic acid with a gradient of acetonitrile from
if they had Ͼ30 IU FSH/L and Ͻ100 pmol estradiol/L, and as
25–100%. Detection and quantification were performed via
perimenopausal if they had Ͼ30 IU FSH/L and Ͼ100 pmol
photo diode array detector. Flavone was used as the internal
estradiol/L or Ͻ30 IU FSH/L and Ͻ100 pmol estradiol/L.
standard; the limit of detection (LOD) was 0.05 g/mL, and the
However, if a woman had noted on the questionnaire com-
limit of quantitation (LOQ) was 0.1 g/mL.
pleted at the initial home visit that she was currently menstru-
Total and free pyridinoline and deoxypyridinoline, markers
ating, but her baseline hormone profile was that of a postmeno-
of bone resorption, were measured in urine samples collected at
pausal woman (ie, Ͼ30 IU FSH/L and Ͻ100 pmol estradiol/L),
baseline and when nearing completion at 12 mo with the use of
she was classified as perimenopausal.
a rapid automated assay technique according to the method ofPratt et al (34). Briefly, for total pyridinoline and deoxypyr-idinoline, 0.5 mL urine was hydrolyzed with an equal volume
Bone density, body composition, and calcium and vitamin
of 12 mmol/L HCl for 18 h at 107 °C. Hydrolysates were
D intakes
centrifuged for 2 min at 13 500 ϫ g and room temperature, and
Bone density and body composition were assessed by dual-
hydroxypyridinium cross-links were extracted from 0.5 mL of
energy X-ray absorptiometry (DXA) at baseline and after Ϸ12
the supernatant by solid-phase extraction (employing cellu-
mo with the use of an Hologic QDR-4500A scanner (Hologic
lose). Pyridinoline and deoxypyridinoline were separated and
Inc, Waltham, MA). The precision of the in vivo measurement
quantified by using HPLC. Free pyridinoline and deoxypyr-
of BMC by DXA in the Metabolic Bone Unit at Addenbrooke’s
idinoline were measured without the hydrolysis step. The with-
Hospital is 1% in the spine and 2–3% in the proximal femur.
in-batch CV was Ͻ3% for pyridinoline and Ͻ5% for deoxy-
Individual scans of the lumbar spine (L1–L4), hip (femoral
pyridinoline measurements; baseline and 12-mo urine samples
neck, trochanter, and intertrochanteric region), and whole body
from individual participants were analyzed together in the same
were taken. If a scan revealed signs of osteoporosis (ie, a BMD
batch. All urine samples were analyzed for their creatinine
T-score ϽϪ2.5), the participant was notified in writing and
TABLE 1 Baseline characteristics and time between measurements in subjects receiving isoflavone or placebo tablets1
Total pyridinoline (nmol/mmol creatinine)
Total deoxypyridinoline (nmol/mmol creatinine)
1 DXA, dual-energy X-ray absorptiometry; BMC, bone mineral content; BMD, bone mineral density; ALP,
alkaline phosphatase; PINP, N-propeptide of collagen type I. Differences between treatment groups werenonsignificant (P Ͼ 0.05). 3 Menopausal status unknown for 3 women in the isoflavone group; percentages may not add to 100%
4 Isoflavone group, n ϭ 78; Placebo group, n ϭ 81. 5 Isoflavone group, n ϭ 81; Placebo group, n ϭ 88. 6 Isoflavone group, n ϭ 77; Placebo group, n ϭ 81.
advised to visit her general practitioner. Follow-up spine data
Windows operating system. A P value of Ͻ0.05 was consid-
were not available for one woman in the isoflavone group, and
ered significant. Changes in BMC, BMD, markers of bone
follow-up bone density and body-composition data were not
turnover, body composition, and intakes of calcium and vita-
available for one woman in the placebo group. Six women
min D were calculated as 12-mo data minus baseline data. We
from the isoflavone group and 8 women from the placebo
used Student’s t tests to test for differences between treatment
group were excluded from all analyses regarding bone, because
groups for changes in BMC, BMD, markers of bone turnover,
they had taken medications during the study that can affect
and body composition. Data on changes in calcium and vitamin
bone density (eg, bisphosphonates, statins, or calcium and
D intakes were skewed, and therefore the nonparametric Wil-
vitamin D supplements). Participants’ height and weight were
coxon’s rank-sum test was used to test for differences between
measured at the time of the DXA scans, and body mass index
(BMI) was calculated as [weight (kg)/height (m2)]; baselineheight was unavailable for one woman in the isoflavone group.
Participants were asked to complete a food-frequency ques-
tionnaire (FFQ) at baseline and after 12 mo on the study.
Baseline characteristics are shown in Table 1. Differences
Participants were given verbal and written instructions on how
between treatment groups were nonsignificant (P Ͼ 0.05).
to complete the FFQ, and calculation of calcium and vitamin D
Sixteen women withdrew from the isoflavone group and 12
intakes was based on published food-composition tables (38).
withdrew from the placebo group (Figure 1). The principalreasons for withdrawal were commencement of HRT and work
Sample size and data analysis
commitments or family problems that prevented completion of
A sample of 100 in each treatment group gave 80% power to
study activities. Other reasons included feeling no beneficial
detect a Ն1.3% difference between groups with respect to the
effects of the intervention or having no interest in continuing
change in BMC over 1 y, assuming an SD of 3.2% and setting
on the trial, heavy menstrual bleeding, or illnesses preventing
␣ at 0.05. Interactions between treatment group and polymor-
completion of study activities (eg, severe hip pain, skin irrita-
phisms in the estrogen receptor and vitamin D receptor genes
tion and sores, vomiting, and diarrhea). One woman in the
are not reported because of a lack of power to detect significant
isoflavone group was diagnosed with an interval cancer of the
associations. Results are available from the authors on request.
breast (ie, a cancer detected in the interval after a negative
Statistical analyses were performed by using SAS statistical
mammographic result) 2 mo after the start of the intervention
software (version 6.12; SAS Institute, Cary, NC) under the
and was withdrawn from the study. The difference between
FIGURE 2. Mean (ϮSEM) urinary isoflavone excretion (sum of daid-
zein, genistein, formononetin, and biochanin A) by treatment group atbaseline, 6 mo, and 12 mo, excluding samples with Ͻ70% or Ͼ110%p-aminobenzoic acid recovery. At baseline: isoflavone group, n ϭ 66;placebo group, n ϭ 72. At 6 mo: isoflavone group, n ϭ 70; placebo group,
n ϭ 73. At 12 mo: isoflavone group, n ϭ 76; placebo group, n ϭ 79. Thedifference in isoflavone excretion between treatment groups was nonsig-nificant at baseline (P ϭ 0.23), but differences between treatment groupsat 6 and 12 mo were highly significant (both: P Ͻ 0.001).
treatment groups in the number of withdrawals was not signif-
icant (2 ϭ 1.123, P ϭ 0.29).
According to the PABA-check method, 58%, 72%, and 77%
of the women had complete urine collections at baseline, 6 mo,and 12 mo, respectively. A further 22%, 11%, and 13% hadPABA recoveries between 70% and 85% at baseline, 6 mo, and
12 mo, respectively. Differences between treatment groups in sum isoflavone excretion (sum of daidzein, genistein, for- mononetin, and biochanin A) were nonsignificant at baseline, but differences were highly significant at 6 and 12 mo (Figure 2). The data shown do not include women with Ͻ70% or FIGURE 3. Mean (ϮSEM) changes in spine and hip bone mineral
Ͼ110% PABA recovery. Inclusion of these women did not
content (BMC) and bone mineral density (BMD) at 1 y by treatment group. Isoflavone group, n ϭ 77 (n ϭ 78 for hip); placebo group, n ϭ 81.
alter the results. Among women in the placebo group, isofla-
Interactions between menopausal status and treatment group for changes in
vone excretion did not change significantly from baseline to 6
BMC or BMD were nonsignificant. Differences between treatment groups
mo (P ϭ 0.80) or from baseline to 12 mo (P ϭ 0.15; Figure 2).
with respect to changes in spine BMC and BMD were significant (P ϭ 0.04
There were no significant differences between treatment
and P ϭ 0.03, respectively); differences between treatment groups with
groups with respect to changes in dietary intakes of calcium
respect to changes in hip BMC and BMD were nonsignificant (P ϭ 0.48and P ϭ 0.30, respectively).
and vitamin D from baseline to 12 mo; mean (ϮSD) changesin calcium intakes for women in the isoflavone and placebogroups, respectively, were – 43 Ϯ 224 and – 54 Ϯ165 mg/d
ences between treatment groups were not significant (Figure
(P ϭ 0.32), and changes in vitamin D intakes for women in the
3). Similar results were found when considering percentage
isoflavone and placebo groups, respectively, were – 0.24 Ϯ 1.6
changes (data not shown). In an analysis of covariance on
and – 0.19 Ϯ 2.3 g/d (P ϭ 0.52).
changes from baseline to 12 mo, with baseline data (BMC or
Changes in spine and hip BMC and BMD at 1 y by treatment
BMD) as a covariate, the effect of treatment group on the
group are shown in Figure 3. Interactions between treatment
changes in spine BMC and BMD remained significant (P ϭ
group and menopausal status for the changes in spine or hip
0.05, and P ϭ 0.03, respectively). Similarly, for changes in hip
BMC and BMD were not significant (P Ͼ 0.05). Differences
BMC and BMD, the effect of treatment group remained non-
between treatment groups for losses of spine BMC and BMD
significant (P ϭ 0.38 and P ϭ 0.85, respectively).
were significant. Percentage change in spine BMC and BMD
Markers of bone turnover at baseline and 12 mo by treatment
among women in the isoflavone and placebo groups, respec-
group are shown in Table 2. The difference between treatment
tively, showed similar trends: mean (ϮSEM) BMC: Ϫ1.42 Ϯ
groups with respect to the change in PINP was of borderline
0.36% and Ϫ2.35 Ϯ 0.37% (P ϭ 0.07); BMD: Ϫ1.08 Ϯ 0.27%
significance. The interaction between treatment group and
and Ϫ1.86 Ϯ 0.29% (P ϭ 0.05). Decreases in BMC and BMD
menopausal status was significant for the changes in bone ALP
of the hip were generally greater among women in the placebo
and PINP (P ϭ 0.05 and P ϭ 0.03, respectively). When
group than among women in the isoflavone group, but differ-
grouped by menopausal status, differences between treatment
TABLE 2 Markers of bone turnover at baseline and at 12 mo according to treatment group1 1 x Ϯ SD. ALP, alkaline phosphatase; PINP, N-propeptide of collagen type I. 2 n ϭ 80 for pyridinoline and deoxypyridinoline.
groups were significant among postmenopausal women; mean
than the trabecular bone of which the spine is primarily com-
(ϮSD) changes in bone ALP among postmenopausal women in
posed (39, 40). Furthermore, precision of the measurement of
the isoflavone and placebo groups, respectively, were 5.65 Ϯ
hip BMC is lower than that of the measurement of spine BMC
5.92 and 3.71 Ϯ 2.92 U/L (P ϭ 0.04), and changes in PINP
(Ϸ2–3% for the proximal femur compared with 1% for the
among postmenopausal women in the isoflavone and placebo
spine; JE Compston, personal communications, 1997 and
groups, respectively, were 9.72 Ϯ 25.19 and Ϫ1.40 Ϯ 19.12
2002), and therefore the power to detect significant differences
mg/L (P ϭ 0.01). No other changes differed significantly
between treatment groups was lower as a result of slow bone
between treatment groups. Results similar to those for total
turnover and lower measurement precision.
pyridinoline and deoxypyridinoline were obtained for free pyr-
Potter et al (19) previously reported an increase in lumbar
idinoline and deoxypyridinoline (data not shown). There were
spine BMC and BMD among postmenopausal women whose
no significant differences between treatment groups with re-
diets were supplemented daily for 24 wk with soy protein
spect to the changes in whole-body BMC or BMD or body-
isolate providing 90 mg, but not 56 mg, isoflavones/d. In our
composition measures (Table 3), and interactions between
study, we did not see an increase in BMC or BMD with the
treatment group and menopausal status were not significant
isoflavone supplement, but the daily dose of isoflavones was
lower than that used by Potter et al (19). However, in a studyof perimenopausal women, Alekel et al (20) did not see an
DISCUSSION
increase in lumbar spine BMC or BMD with a daily dose of
This is one of the longest and largest studies to date to
80.4 mg isoflavones (as soy protein) for 24 wk, but, similar to
examine the effects of an isoflavone supplement derived from
our study, they saw a reduction in the extent of bone loss. In a
red clover on spine and hip BMC and BMD, biochemical
recent study of 28 premenopausal women (mean age: 24 y)
markers of bone turnover, and body composition. We observed
there were no significant effects of a soy protein supplement
an attenuation of lumbar spine bone loss among women taking
that provided either 0 or 90 mg isoflavones/d for 12 mo (41).
the isoflavone supplement compared with that among women
This suggests that isoflavones may be beneficial in attenuating
taking the placebo. Trends for losses of hip BMC and BMD
age-associated bone loss rather than in enhancing peak bone
were similar to those seen in the lumbar spine, but differences
mass in younger premenopausal women.
between treatments were not significant. However, this was not
Promensil tablets contain isoflavones derived from red clo-
entirely surprising, given that the hip contains a relatively large
ver and, unlike soy protein, relatively large proportions of
proportion of cortical bone, which is metabolically less active
biochanin A and formononetin, in addition to daidzein and
TABLE 3 BMI, body composition, and total-body bone mineral content (BMC) and bone mineral density (BMD) at baseline and at 12 mo by treatment group1 1 x Ϯ SD. Differences between treatment groups with respect to changes from baseline to 12 mo were
2 Placebo group, n ϭ 90. 3 Isoflavone group, n ϭ 78; placebo group, n ϭ 80.
genistein (29). It has been observed that the use of isoflavone
All authors participated fully in the preparation of the manuscript. CA
extracts does not always result in lipid-lowering effects (42,
was responsible for subject recruitment and day-to-day running of the trial,
43) that are the same as those seen with intact soy protein (44),
sample analyses, and statistical analyses; JEC was responsible for bone
and it has been suggested that the isoflavone extraction process
densitometry; NED was responsible for the data analysis; MD was respon-sible for the hormone assays; and SAB was responsible for the design of
may remove some component of the food that has synergistic
the experiment, sample analysis, and significant advice and consultation
effects in combination with isoflavones or that isoflavones may
regarding all aspects of the trial. None of the authors had conflicts of
become inactivated during the isolation and purification pro-
cess (45, 46). However, the combination of isoflavones in afood or dietary supplement also may be important in terms oftheir potential beneficial health effects. It was suggested that
REFERENCES
daidzein may be more important than other isoflavones in
1. Castelo-Branco C, Figueras F, Sanjuan A, Pons F, Vicente JJ, Vanrell
terms of relieving menopausal symptoms (47), and the tablets
JA. Long-term postmenopausal hormone replacement therapy effects
used in the present study were previously shown to produce
on bone mass: differences between surgical and spontaneous patients.
beneficial effects on bone (20), but conflicting data have been
Eur J Obstet Gynecol Reprod Biol 1999;83:207–11.
2. Pilon D, Castilloux AM, LeLorier J. Estrogen replacement therapy:
presented with respect to blood lipid concentrations (42, 43).
determinants of persistence with treatment. Obstet Gynecol 2001;97:
Because of both the structural similarity of isoflavones to
mammalian estrogens and their ability to bind to estrogen
3. Castelo-Branco C, Figueras F, Sanjuan A, et al. Long-term compliance
receptors (7), it is widely hypothesized that the actions of
with estrogen replacement therapy in surgical postmenopausal women:
isoflavones are mediated via the estrogen receptors. However,
benefits to bone and analysis of factors associated with discontinua-tion. Menopause 1999;6:307–11.
the exact mechanism of action of isoflavones on bone remains
4. Reinli K, Block G. Phytoestrogen content of foods—a compendium of
to be fully elucidated. In our study, the 2 bone formation
literature values. Nutr Cancer 1996;26:123– 48.
markers increased in postmenopausal women taking the isofla-
5. Liggins J, Bluck LJ, Runswick S, Atkinson C, Coward WA, Bingham
vone supplement. This is somewhat in agreement with studies
SA. Daidzein and genistein contents of vegetables. Br J Nutr 2000;84:717–25.
in ovariectomized rats suggesting that soy or isoflavones stim-
6. Setchell KDR, Adlercreutz H. Mammalian lignans and phyto-oestro-
ulate bone formation (10, 48). However, we did not see overall
gens: recent studies on their formation, metabolism and biological role
increases in BMC or BMD, but such discord between markers
in health and disease. In: Rowland I, ed. Role of the gut flora in
of bone turnover and BMD adds to the ongoing controversy
toxicity and cancer. London: Academic Press, 1988:315– 45.
surrounding the use of biochemical markers as predictors of
7. Setchell KD, Cassidy A. Dietary isoflavones: biological effects and
relevance to human health. J Nutr 1999;129:758S– 67S.
8. Ling X, Lu A, Zhao X, Chen X, Cummings SR. Very low rates of hip
Prospective and case-control studies showed positive asso-
fracture in Beijing, People’s Republic of China: the Beijing Osteopo-
ciations between weight and the risk of breast cancer among
rosis Project. Am J Epidemiol 1996;144:901–7.
postmenopausal women and negative associations among pre-
9. Lau EM, Cooper C. The epidemiology of osteoporosis. The oriental
menopausal women (reviewed in 50). Furthermore, increased
perspective in a world context. Clin Orthop 1996;323:65–74.
10. Arjmandi BH, Alekel L, Hollis BW, et al. Dietary soybean protein
abdominal fat has consistently been associated with increased
prevents bone loss in an ovariectomized rat model of osteoporosis. J
mortality and with the incidence of cardiovascular disease,
hypertension, and diabetes (51, 52). The menopause is associ-
11. Harrison E, Adjei A, Ameho C, Yamamoto S, Kono S. The effect of
ated with a potentially detrimental shift in the distribution of fat
soybean protein on bone loss in a rat model of postmenopausalosteoporosis. J Nutr Sci Vitaminol (Tokyo) 1998;44:257– 68.
toward a more central location (53–55), but in users of HRT,
12. Arjmandi BH, Getlinger MJ, Goyal NV, et al. Role of soy protein with
this shift is minimized, and HRT users are more likely to have
normal or reduced isoflavone content in reversing bone loss induced
less abdominal fat than do nonusers (56–58). In the present
by ovarian hormone deficiency in rats. Am J Clin Nutr 1998;68(suppl):
study, we did not see a significant effect of the isoflavone
supplement on the distributions of fat and lean tissue within the
13. Greendale GA, FitzGerald G, Huang MH, et al. Dietary soy isofla-
vones and bone mineral density: results from the study of women’s
health across the nation. Am J Epidemiol 2002;155:746 –54.
Despite being one of the longest intervention studies with an
14. Mei J, Yeung SS, Kung AW. High dietary phytoestrogen intake is
isoflavone supplement to date, a potential limitation of this
associated with higher bone mineral density in postmenopausal but not
study is that it was relatively short-term with respect to the
premenopausal women. J Clin Endocrinol Metab 2001;86:5217–21.
15. Horiuchi T, Onouchi T, Takahashi M, Ito H, Orimo H. Effect of soy
outcome measures; longer-term studies are needed to deter-
protein on bone metabolism in postmenopausal Japanese women.
mine the effects of isoflavones (both as intact soy protein and
as dietary supplements) on hip BMC and BMD and also on
16. Ho SC, Chan SG, Yi Q, Wong E, Leung PC. Soy intake and the
longer-term outcome measures such as fracture rates. Never-
maintenance of peak bone mass in Hong Kong Chinese women.
theless, our findings suggest that, through attenuation of bone
17. Somekawa Y, Chiguchi M, Ishibashi T, Aso T. Soy intake related to
loss, the isoflavone supplement has a potentially protective
menopausal symptoms, serum lipids, and bone mineral density in
postmenopausal Japanese women. Obstet Gynecol 2001;97:109 –15.
We thank Sue Gardner, Nicola Duffy, Nasima Siddiqui, Jane Bettany,
18. Nagata C, Shimizu H, Takami R, Hayashi M, Takeda N, Yasuda K.
and Jayne Girvan for their assistance with the day-to-day running of the
Soy product intake and serum isoflavonoid and estradiol concentra-tions in relation to bone mineral density in postmenopausal Japanese
trial; Shirley Love for the measurement of bone density and body
women. Osteoporos Int 2002;13:200 – 4.
composition; Simon P Robins, Phyllis Nicol, and Alexander Duncan for
19. Potter SM, Baum JA, Teng H, Stillman RJ, Shay NF, Erdman JW Jr.
the bone marker assays; Alison Dunning, Catherine Healey, and Alex
Soy protein and isoflavones: their effects on blood lipids and bone
Loktionov for the genotyping; and Addenbrooke’s Hospital Pharmacy
density in postmenopausal women. Am J Clin Nutr 1998;68(suppl):
for administering the tablets. Novogen Ltd performed the urinary isofla-
20. Clifton-Bligh PB, Baber RJ, Fulcher GR, Nery ML, Moreton T. The
effect of isoflavones extracted from red clover (Rimostil) on lipid and
39. Cooper C. Bone mass throughout life: bone growth and involution. In:
bone metabolism. Menopause 2001;8:259 – 65.
Francis RM, Dick WC, eds. Osteoporosis: pathogenesis and management.
21. Alekel DL, Germain AS, Peterson CT, Hanson KB, Stewart JW, Toda
Dordrecht, Netherlands: Kluwer Academic Publishers, 1990:1–26.
T. Isoflavone-rich soy protein isolate attenuates bone loss in the
40. Reeve J. Clinical assessment of the physical properties of bone. In:
lumbar spine of perimenopausal women. Am J Clin Nutr 2000;72:
Compston JE, ed. Osteoporosis: new perspectives on causes, preven-
tion and treatment. London: Royal College of Physicians of London,
22. Scheiber MD, Liu JH, Subbiah MT, Rebar RW, Setchell KD. Dietary
inclusion of whole soy foods results in significant reductions in clinical
41. Anderson JJ, Chen X, Boass A, et al. Soy isoflavones: no effects on bone
risk factors for osteoporosis and cardiovascular disease in normal
mineral content and bone mineral density in healthy, menstruating young
postmenopausal women. Menopause 2001;8:384 –92.
adult women after one year. J Am Coll Nutr 2002;21:388 –93.
23. Chiechi LM, Secreto G, D’Amore M, et al. Efficacy of a soy rich diet
42. Nestel PJ, Yamashita T, Sasahara T, et al. Soy isoflavones improve
in preventing postmenopausal osteoporosis: the Menfis randomized
systemic arterial compliance but not plasma lipids in menopausal and
perimenopausal women. Arterioscler Thromb Vasc Biol 1997;17:3392– 8.
24. Uesugi T, Fukui Y, Yamori Y. Beneficial effects of soybean isofla-
43. Hodgson JM, Puddey IB, Beilin LJ, Mori TA, Croft KD. Supplemen-
vone supplementation on bone metabolism and serum lipids in post-
tation with isoflavonoid phytoestrogens does not alter serum lipid
menopausal Japanese women: a four-week study. J Am Coll Nutr
concentrations: a randomized controlled trial in humans. J Nutr 1998;
25. Upmalis DH, Lobo R, Bradley L, Warren M, Cone FL, Lamia CA.
44. Anderson JW, Johnstone BM, Cook-Newell ME. Meta-analysis of the
Vasomotor symptom relief by soy isoflavone extract tablets in post-
effects of soy protein intake on serum lipids. N Engl J Med 1995;333:
menopausal women: a multicenter, double-blind, randomized, placebo-
controlled study. Menopause 2000;7:236 – 42.
26. Knight DC, Howes JB, Eden JA, Howes LG. Effects on menopausal
45. Barnes S. Phytoestrogens and breast cancer. Baillieres Clin Endocrinol
symptoms and acceptability of isoflavone-containing soy powder di-
etary supplementation. Climacteric 2001;4:13– 8.
46. Clarkson TB, Anthony MS. Phytoestrogens and coronary heart dis-
27. Hale GE, Hughes CL, Robboy SJ, Agarwal SK, Bievre M. A double-
ease. Baillieres Clin Endocrinol Metab 1998;12:589 – 604.
blind randomized study on the effects of red clover isoflavones on the
47. Eden J. Phytoestrogens and the menopause. Baillieres Clin Endocrinol
endometrium. Menopause 2001;8:338 – 46.
28. Wolfe JN. Breast patterns as an index of risk for developing breast
48. Fanti O, Faugere MC, Gang Z, Schmidt J, Cohen D, Malluche HH.
cancer. AJR Am J Roentgenol 1976;126:1130 –7.
Systematic administration of genistein partially prevents bone loss in
29. Setchell KD, Brown NM, Desai P, et al. Bioavailability of pure
ovariectomized rats in a nonestrogen-like mechanism. Am J Clin Nutr
isoflavones in healthy humans and analysis of commercial soy isofla-
vone supplements. J Nutr 2001;131:1362S–75S.
49. Looker AC, Bauer DC, Chesnut CH III, et al. Clinical use of biochem-
30. Bingham S, Cummings JH. The use of 4-aminobenzoic acid as a
ical markers of bone remodeling: current status and future directions.
marker to validate the completeness of 24 h urine collections in man.
50. Cleary MP, Maihle NJ. The role of body mass index in the relative risk
31. Johansson G, Bingham S, Vahter M. A method to compensate for
of developing premenopausal versus postmenopausal breast cancer.
incomplete 24-hour urine collections in nutritional epidemiology stud-
Proc Soc Exp Biol Med 1997;216:28 – 43.
ies. Public Health Nutr 1999;2:587–91.
51. Bjorntorp P. Abdominal fat distribution and disease: an overview of
32. Setchell KD, Welsh MB, Lim CK. High-performance liquid chromato-
epidemiological data. Ann Med 1992;24:15– 8.
graphic analysis of phytoestrogens in soy protein preparations with
52. Pi-Sunyer FX. Health implications of obesity. Am J Clin Nutr 1991;
ultraviolet, electrochemical and thermospray mass spectrometric de-
tection. J Chromatogr 1987;386:315–23.
53. Poehlman ET, Toth MJ, Gardner AW. Changes in energy balance and
33. Franke AA, Custer LJ, Cerna CM, Narala K. Rapid HPLC analysis of
body composition at menopause: a controlled longitudinal study. Ann
dietary phytoestrogens from legumes and from human urine. Proc Soc
54. Svendsen OL, Hassager C, Christiansen C. Age- and menopause-
34. Pratt DA, Daniloff Y, Duncan A, Robins SP. Automated analysis of
associated variations in body composition and fat distribution in
the pyridinium crosslinks of collagen in tissue and urine using solid-
healthy women as measured by dual-energy X-ray absorptiometry.
phase extraction and reversed-phase high-performance liquid chroma-
tography. Anal Biochem 1992;207:168 –75.
35. Gomez B Jr, Ardakani S, Ju J, et al. Monoclonal antibody assay for
55. Tremollieres FA, Pouilles JM, Ribot CA. Relative influence of age and
measuring bone-specific alkaline phosphatase activity in serum. Clin
menopause on total and regional body composition changes in post-
menopausal women. Am J Obstet Gynecol 1996;175:1594 – 600.
36. Melkko J, Kauppila S, Niemi S, et al. Immunoassay for intact amino-
56. Perrone G, Liu Y, Capri O, et al. Evaluation of the body composition
terminal propeptide of human type I procollagen. Clin Chem 1996;42:
and fat distribution in long-term users of hormone replacement ther-
apy. Gynecol Obstet Invest 1999;48:52–5.
37. Dowsett M, Goss PE, Powles TJ, et al. Use of the aromatase inhibitor
57. Reubinoff BE, Wurtman J, Rojansky N, et al. Effects of hormone
4-hydroxyandrostenedione in postmenopausal breast cancer: optimi-
replacement therapy on weight, body composition, fat distribution, and
zation of therapeutic dose and route. Cancer Res 1987;47:1957– 61.
food intake in early postmenopausal women: a prospective study.
38. Bingham SA, Welch AA, McTaggart A, et al. Nutritional methods in
the European Prospective Investigation of Cancer in Norfolk. Public
58. Sites CK. Hormone replacement therapy: cardiovascular benefits for
aging women. Coron Artery Dis 1998;9:789 –93.
Erläuterungen zu einzelnen Methoden der Lungenfunktionsdiagnostik Bodyplethysmographie, Spirometrie, kapilläre Blutgasanalyse Standardverfahren. Ermittelt werden Basisdaten wie Atemwegswiderstand, alle statischen und dynamischen Lungenvolumina und die Gasaustauschfunktion. Indikationen: • Nachweis/Verlaufskontrolle obstruktiver Atemwegserkrankungen (z.B. COPD, Asthma bronchi
 The effects of phytoestrogen isoflavones on bone density in women:a double-blind, randomized, placebo-controlled trial1–3
Charlotte Atkinson, Juliet E Compston, Nicholas E Day, Mitch Dowsett, and Sheila A Bingham
ABSTRACT
The effects of phytoestrogen isoflavones on bone density in women:a double-blind, randomized, placebo-controlled trial1–3
Charlotte Atkinson, Juliet E Compston, Nicholas E Day, Mitch Dowsett, and Sheila A Bingham
ABSTRACT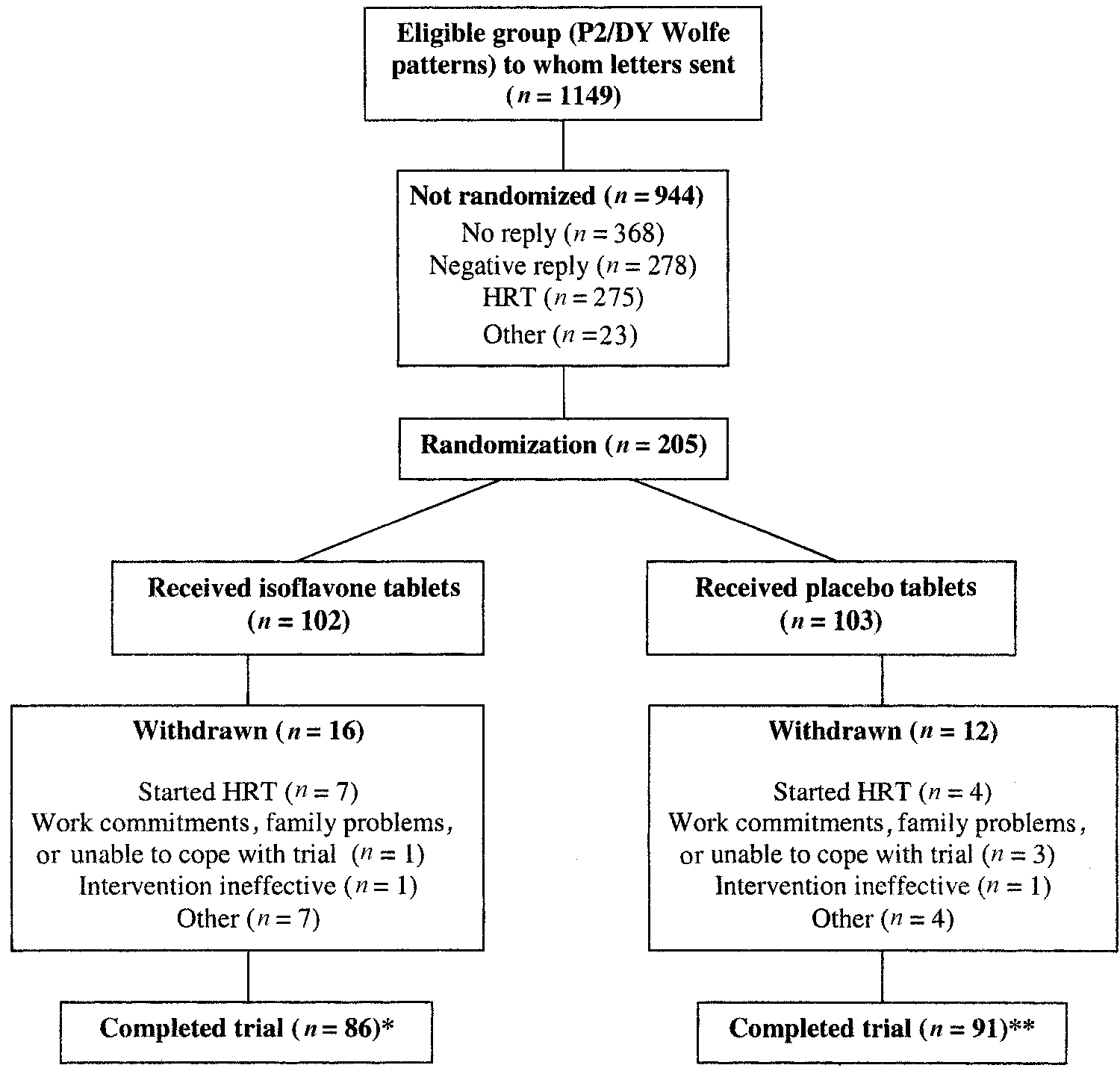
 FIGURE 1. Flow chart describing the progress of the volunteers during the trial. HRT, hormone replacement therapy. *Includes 2 women who completed
FIGURE 1. Flow chart describing the progress of the volunteers during the trial. HRT, hormone replacement therapy. *Includes 2 women who completed number generation in MICROSOFT EXCEL (version 2.2; Mi-
content (Kone autoanalyser; Jaffe method), and excretion of
crosoft Corp, Redmond, WA), and researchers and study par-
pyridinoline and deoxypyridinoline was corrected for creati-
ticipants remained blinded to the tablet allocation throughout
the study. Participants were asked to take 1 tablet/d. The codeidentifying those who had been taking the isoflavone tablets
Blood samples
number generation in MICROSOFT EXCEL (version 2.2; Mi-
content (Kone autoanalyser; Jaffe method), and excretion of
crosoft Corp, Redmond, WA), and researchers and study par-
pyridinoline and deoxypyridinoline was corrected for creati-
ticipants remained blinded to the tablet allocation throughout
the study. Participants were asked to take 1 tablet/d. The codeidentifying those who had been taking the isoflavone tablets
Blood samples TABLE 1
TABLE 1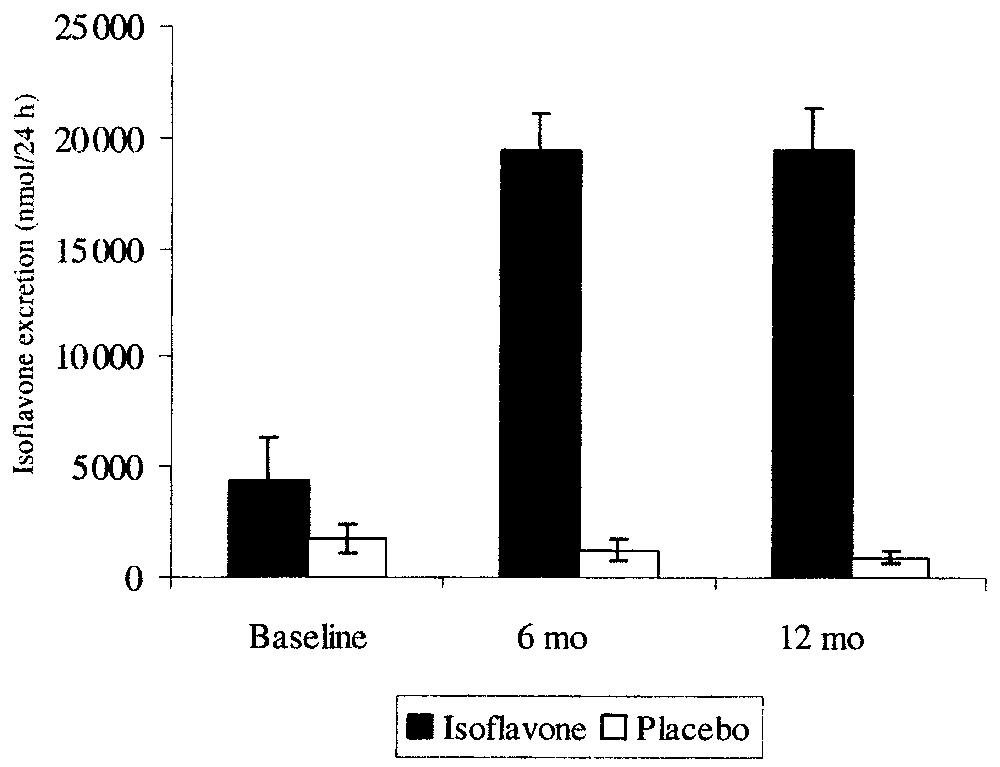
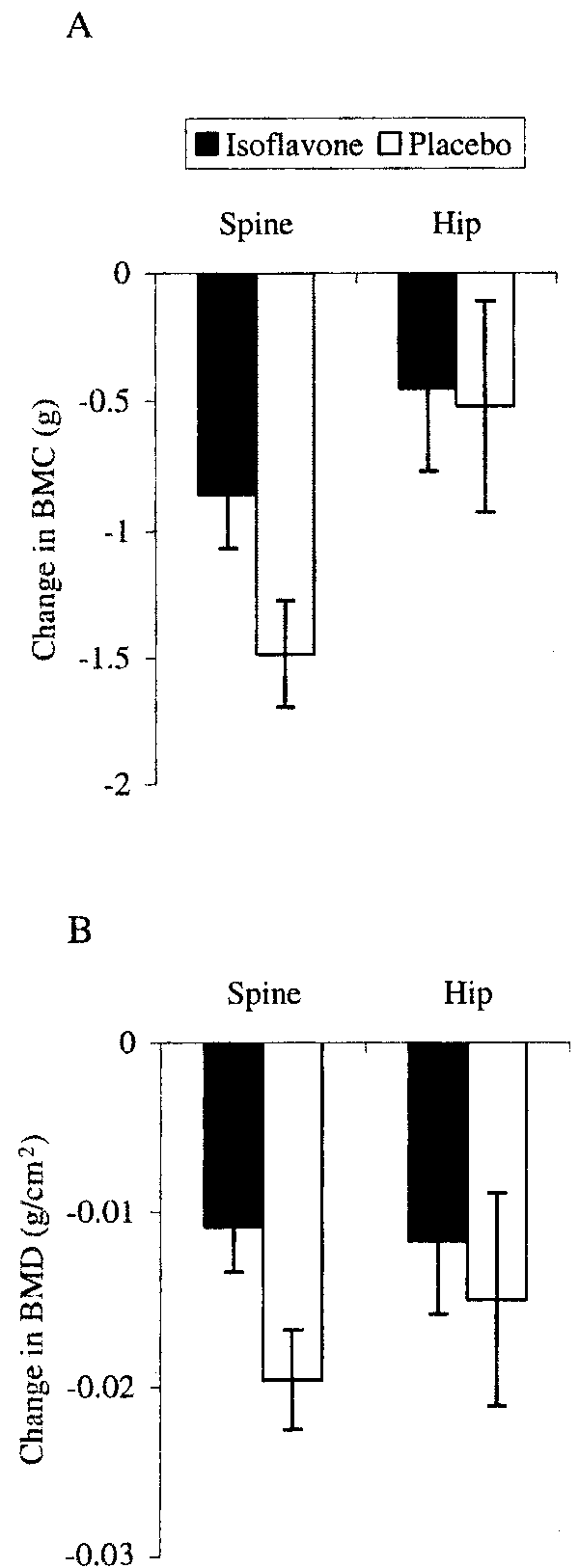
 FIGURE 2. Mean (ϮSEM) urinary isoflavone excretion (sum of daid-
FIGURE 2. Mean (ϮSEM) urinary isoflavone excretion (sum of daid- TABLE 2
TABLE 2
 genistein (29). It has been observed that the use of isoflavone
All authors participated fully in the preparation of the manuscript. CA
extracts does not always result in lipid-lowering effects (42,
was responsible for subject recruitment and day-to-day running of the trial,
43) that are the same as those seen with intact soy protein (44),
sample analyses, and statistical analyses; JEC was responsible for bone
and it has been suggested that the isoflavone extraction process
densitometry; NED was responsible for the data analysis; MD was respon-sible for the hormone assays; and SAB was responsible for the design of
may remove some component of the food that has synergistic
the experiment, sample analysis, and significant advice and consultation
effects in combination with isoflavones or that isoflavones may
regarding all aspects of the trial. None of the authors had conflicts of
become inactivated during the isolation and purification pro-
cess (45, 46). However, the combination of isoflavones in afood or dietary supplement also may be important in terms oftheir potential beneficial health effects. It was suggested that
REFERENCES
genistein (29). It has been observed that the use of isoflavone
All authors participated fully in the preparation of the manuscript. CA
extracts does not always result in lipid-lowering effects (42,
was responsible for subject recruitment and day-to-day running of the trial,
43) that are the same as those seen with intact soy protein (44),
sample analyses, and statistical analyses; JEC was responsible for bone
and it has been suggested that the isoflavone extraction process
densitometry; NED was responsible for the data analysis; MD was respon-sible for the hormone assays; and SAB was responsible for the design of
may remove some component of the food that has synergistic
the experiment, sample analysis, and significant advice and consultation
effects in combination with isoflavones or that isoflavones may
regarding all aspects of the trial. None of the authors had conflicts of
become inactivated during the isolation and purification pro-
cess (45, 46). However, the combination of isoflavones in afood or dietary supplement also may be important in terms oftheir potential beneficial health effects. It was suggested that
REFERENCES effect of isoflavones extracted from red clover (Rimostil) on lipid and
39. Cooper C. Bone mass throughout life: bone growth and involution. In:
bone metabolism. Menopause 2001;8:259 – 65.
effect of isoflavones extracted from red clover (Rimostil) on lipid and
39. Cooper C. Bone mass throughout life: bone growth and involution. In:
bone metabolism. Menopause 2001;8:259 – 65.