Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Doi:10.1016/j.chiabu.2004.04.005
Child Abuse & Neglect 28 (2004) 925–937
Disciplinary choices of mothers of deaf children
and mothers of normally hearing childrenଝ
John F. Knutson, Christina R. Johnson, Patricia M. Sullivan
a Department of Psychology, The University of Iowa, E-11 Seashore Hall, Iowa City, IA 52240, USA
b Boys Town National Research Hospital, Omaha, NE, USA
Received 18 March 2003; received in revised form 6 April 2004; accepted 7 April 2004
Abstract Objective: To assess the disciplinary preferences of mothers of profoundly deaf children and normally hearing children in a test of the hypothesized link between child disabilities and punitive parenting. Method: Disciplinary preferences of mothers seeking a cochlear implant for their profoundly deaf child (n = 57), mothers not seeking an implant for their deaf child (n = 22), and mothers of normally hearing children (n = 27) were assessed using an analog task in which subjects select discipline in response to slide images of children engaging in normative or frankly deviant behaviors that are potentially irritating. Results: Results indicated that mothers of children with profound hearing impairments were more likely to select physical discipline in response to depicted child transgressions and more likely to escalate to physical discipline when the depicted child was described as persisting in the transgression. Additionally, escalation was more probable in response to scenes depicting children engaged in dangerous and destructive acts than in rule-violating acts. Conclusions: Findings were consistent with the hypothesized link between childhood disabilities and child mal- treatment as well as the hypothesis that children with disabilities associated with communication problems could be at risk of physical abuse. 2004 Elsevier Ltd. All rights reserved. Keywords: Discipline; Analog Parenting Task; Disabilities; Deafness
ଝ The development of this paper was supported, in part, by research grant MH61731 funded by NIMH and ACYF, John F. Knutson, Principal
Investigator, and, in part, by a research grant awarded to Department of Otolaryngology—Head and Neck Surgery, University of Iowa, (Number2 P50 DC 00242) from the National Institute of Deafness and Other Communication Disorders, National Institutes of Health; grant RR00059from the General Clinical Research Centers Program, Division of Research Resources, NCRR, NIH; the Lions Clubs International Foundation;and the Iowa Lions Foundation.
1 Present address: Department of Neurology, Creighton University Medical School, Omaha, NE, USA.
0145-2134/$ – see front matter 2004 Elsevier Ltd. All rights reserved. J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937Introduction
Because children with disabilities can occasion some unique parenting challenges, some have hypothe-
sized a link between childhood disabilities and physical maltreatment (cf., Although advocates for this hypothesis have been able tomarshal considerable theoretical support for their position, limited empirical evidence has caused othersto question the notion of a simple link between child maltreatment and childhood disabilities (e.g., ithin the last decade, however,a growing body of research has provided empirical evidence of the association between childhood dis-abilities and maltreatment. For example, using the methodology of the Second National Incidence Study(), provided evidence that children withdisabilities were approximately 1.7 times more likely to be maltreated than children without disabilities. In a hospital-based epidemiological study of maltreatment, established adisability rate among maltreated children that was approximately twice the disability rate among nonmal-treated children. Extending those findings to a school-based population study that was not compromisedby possible sampling biases, reported that the relative risk for physicalabuse varied as a function of the disability classification of the children. For example, although risk forphysical abuse among persons with a physical disability was approximately 1.2 times that of nondisabledchildren, risk for physical abuse among children with other disabilities ranged from 2 to 7.3 times that ofnondisabled children.
The methodology of the studies did not permit an
unequivocal determination as to whether the disabilities contributed to maltreatment or whether maltreat-ment contributed to the disabilities. Within the , however, a subgroup ofsubjects could be identified where there was unequivocal medical evidence that the disability was presentprior to maltreatment. Based on analyses of that subgroup, there was support for the hypothesis thatsome disabilities (e.g., hearing impairment, speech and language disorders, health-related disabilities,developmental disabilities) were more likely to be risk factors than consequences of maltreatment. Forthose disabilities that seemed to be risk factors, the question remained as to why children with a disabilityare at greater risk of maltreatment than are children without a disability.
One hypothesis that has been advanced to account for the putative disability-maltreatment link
is that rearing a disabled child may occasion more parental stress than rearing a nondisabled child(; ; There are, however, at least two lines of evidence that cast doubt on the hypothesisthat stress can be used to account for a disability-abuse link. First, there is some evidence that rear-ing children with disabilities does not necessarily occasion unique stress (It is also the case that the level of reported stress associated with rearing a child with a disabilitydoes not necessarily covary with the severity of the disability (e.g., ). Perhaps more importantly, based on a com-prehensive review of the physical abuse literature published across two decades, concluded that support for the link between parental stress and abuse was not particularlystrong. An alternative hypothesis to account for the disability-physical abuse connection can be de-rived from a discipline-mediated model of physical abuse (cf.,
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Discipline-mediated models of physical abuse have suggested that physical child abuse in the form
of injurious physical discipline might not be qualitatively different from normative physical discipline. Rather, some abusive discipline can be conceptualized as normative discipline that has escalated to aninjurious level. In this theoretical model the escalation in discipline can be due to either the ineffectivedisciplinary strategies of the parents (cf., r some unique interactions between thechild and the caretaker that compromise parental efforts to influence the child’s behavior (cf., In both models, physically abusive parenting is seen as a reflection of the characteris-tics of the parent (e.g., selecting ineffective disciplinary strategies), the characteristics of the child (e.g.,communicative limitations), and the confluence of those child and parental factors in a dynamic disci-plinary context. Thus, in a discipline-mediated model, the occurrence of abuse is placed in a microsocialcontext where a parent’s attempt to influence the child’s behavior in a specific context is ineffective and,as a result, the parent adopts more intensive strategies and more punitive strategies. Such a model couldaccount for the association between some childhood disabilities, such as communication disorders, andmaltreatment.
Consistent with the discipline-mediated model of physical abuse, it has been suggested that communi-
cation difficulties could play a central role in the physical abuse of children with disabilities (e.g., Because the vastmajority of prelingually and perilingually deaf children have normally hearing parents, most prelinguallyand perilingually deaf children have parents who are not fully prepared to communicate effectively withtheir child. Because of the likely communicative difficulties between a deaf child and his or her parents,it has been suggested that deaf children are at particular risk for physical abuse Consistent with that hypothesis are data indicating that parents ofdeaf children are more likely to report the use of physical discipline (e.g., and that deaf children are at increased risk of physical abuse relative to their normally hearing peers (e.g.,
Although the presence of the disability per se has been hypothesized to influence discipline and abuse
by parents of deaf children, it is also possible that the association between disability and abuse reflectssomething about the habilitative or rehabilitative efforts that parents adopt to meet the needs of theirchild. Often parents of disabled children are confronted with difficult choices when attempting to meetthe special needs of their child. How they respond to those choices could reflect something about parentingand the manner with which the parents attempt to influence their child’s development. In recent years,pediatric cochlear implantation for deaf children has moved from being an experimental procedure to aclinically accepted intervention (Yet, because of the highly variableoutcome of cochlear implants, there continues to be considerable controversy regarding implantation ofchildren (cf., Thus, parents of deaf children are oftenconfronted by that controversy as well as the challenge of meeting the needs of their child. Thus, it ispossible that parents who seek an implant might approach child discipline differently than parents whoelect not to seek an implant for their deaf child.
Recent work using Analog Parenting Tasks (APT) (e.g., ;
suggests thatit should be possible to assess the disciplinary preferences of parents of disabled and nondisabled chil-dren to determine whether the presence of a disabled child in the household influences disciplinarypreferences of the parent. Thus, the present study used an analog test of disciplinary preferences todetermine whether rearing a deaf child would influence the disciplinary preferences of parents. Addi-
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
tionally, the study was designed to determine whether disciplinary preferences differed between par-ents seeking an implant for their deaf child and parents who elected not to seek an implant for a deafchild.
Three samples of mothers participated in the study. The first sample consisted of 57 mothers of prelin-
gually deaf children who had been consecutively evaluated for cochlear implantation at The Universityof Iowa Department of Otolaryngology—Head and Neck Surgery. To be eligible for an implant in thisprotocol, the child had to be at least 24 months of age at the time of referral and had to be either con-genitally deafened or had to have incurred a profound bilateral hearing loss prior to 18 months of age. Additionally, the child could receive no appreciable benefit from amplification. The mothers participatedin the tasks of the present study at the time of preimplant evaluations of the children. Parents seeking acochlear implant for their child at The University of Iowa were largely drawn from states in the upperMidwest of the US, but a few families from other areas of the US participated; most resided in urbanand suburban settings, but rural families were included in the sample. Because of the grant-supportednature of the clinical trial, families enrolled in the Iowa Cochlear Implant Clinical Research Center wouldnot incur any out-of-pocket costs for the cochlear implant, the surgery, and the associated hospital andclinic services. Thus, the group of families seeking an implant was essentially unrestricted with respect tosocio-economic status. Two families in the Implant Candidate Group had more than one hearing-impairedchild. The demographic characteristics of the implant seeking sample and the other samples are shownin
The second sample consisted of 22 mothers of prelingually or perilingually deaf children who were
recipients of services at Boys Town National Research Hospital (BTNRH), in Omaha, NE. The mothershad volunteered to participate in psychological research related to the social and cognitive developmentof children with hearing impairments as a “control group” for children receiving a cochlear implant. These BTNRH subjects were mothers who had not sought a cochlear implant for their child prior toenrolling in the study. Additionally, these were mothers who did not seek an implant for their child for atleast 48 months following enrollment in the study. (At the inception of the project in which the present
Table 1Demographic characteristics of the samples
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
study was embedded BTNRH did not offer cochlear implantation; however, implantation was offeredat BTNRH before the project ended. Subsequent to participating in the research protocol, some parentselected to seek an implant for their child, either at BTNRH or another site. If they sought an implant atThe University of Iowa, they were included in the implant-seeking sample described above (n = 2). Ifthey sought an implant at another site, those children and their parents would have been dropped from theresearch protocol; data from such mothers (n = 3) are not included in the current report.) Although mostof the children in the second sample were in the profound range of hearing impairment, six of the childrenrealized some auditory benefit from acoustic amplification (i.e., hearing aids; FM receivers) and wouldnot have been eligible for implantation under the eligibility criteria in place at the time of enrollment inthe research; they would have been eligible under the more relaxed standards that were in place later. Allof the mothers were from the urban or suburban areas of Omaha, Nebraska or Council Bluffs, Iowa.
The third group consisted of 27 mothers of normally hearing children. The Department of Psychology at
The University of Iowa contacts parents of all live-births in Johnson and Linn Counties, Iowa and informsthem about ongoing developmental research in the Department. The Department occasionally recruitsfamilies for the registry using public service announcements, advertisements, and flyers distributed to theschools. Families who are willing to participate in psychological research are placed in the registry forlater recruitment; the mothers in this third research group had recently volunteered to enroll their childrenin studies of spatial reasoning, motor skills, or decision-making. The mothers in the present study wererecruited when their child was in the laboratory participating in the cognitive and motor research. Allof the mothers in this group indicated there were no children living in their households with severe orprofound hearing impairments or any other severe sensory deficits or significant disabilities. At the timeof testing the mothers resided in the small-urban/suburban area of Iowa City, IA.
Mothers of children enrolled in research at BTNRH and the mothers of normally hearing children
were compensated for their participation in the study. Families who were enrolled in the clinical trialof the Iowa Cochlear Implant Clinical Research Center were not compensated for participation in thestudy. However, because of the grant-supported nature of the clinical trial, families enrolled in the IowaCochlear Implant Clinical Research Center could realize significant financial benefit (i.e., free implant,no surgical fees, free clinical service) if their child were to receive an implant. None of the mothers in anyof the groups were deaf. All of the procedures were conducted under informed consent and all procedureshad been approved by the appropriate IRBs. Because the grant supporting the research with deaf childrenwas located at The University of Iowa, The University of Iowa IRB-01 approved the protocol for testingthe two groups of mothers of deaf children; the BTNRH IRB also approved the protocol for the grouprecruited and tested at BTNRH; The University of Iowa IRB-02 approved the protocol for the groupof mothers of normally hearing children. Some of the mothers of deaf children, or their children, havebeen included in samples described in published studies pertaining to pediatric cochlear implantation(e.g.,
To assess disciplinary preferences of the mothers, an Analog Parenting Task first described by
as administered. The APT consists of 28 slides, each depicting a child engaging in a develop-mentally appropriate or developmentally inappropriate activity that could be irritating or concerning to a
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
child’s caretaker. Seven scenes depict a child engaged in destructive acts (e.g., stepping on a calculator,tearing pages from a book), seven scenes depict dangerous activities (e.g., loading a revolver, hanging outthe window of a moving car, sitting on the edge of a roof), and seven depict rule-violating behaviors (e.g.,theft, drinking an alcoholic beverage, smoking). The remaining scenes include age-appropriate acts (e.g.,spilling a jar of salsa, messy play with toys). In response to each scene, the subject was asked to imaginethat she is charged with the responsibility of caring for the depicted child, to indicate her emotionalreaction to the depicted child (e.g., anger, worry, annoyance, amusement), and to classify the depictedbehavior (e.g., sloppy, destructive, dangerous, fine). After rating and classifying the depicted behaviorthe subject was asked to select the disciplinary response she would use if she were attempting to alter thechild’s behavior. Disciplinary choices included such acts as: ignoring, verbal reprimands, restriction ofprivileges, spanking, striking other than spanking, and striking with objects. Although the more severeacts were potentially injurious, the possible injurious consequences of the acts were not specified in thetask. After selecting a disciplinary strategy the subject was asked to indicate how many times she wouldpermit the child to engage in the depicted behavior before changing her disciplinary response. If thesubject indicated that she would change her disciplinary tactic, she was asked to indicate what that nextdisciplinary alternative would be.
For the present study there were two dependent measures. The first was the frequency with which the
subject’s initial disciplinary choice involved the use of physical discipline. The second dependent measurewas the use of “escalated” discipline as described by Escalated discipline isa circumstance where the subject shifts from a nonphysical form of discipline to physical discipline ifthe depicted child were to persist in the displayed behavior. Escalated discipline can also occur whenthe subject shifts from minor physical discipline (e.g., spanking) to potentially injurious discipline (e.g.,striking with an object) if the depicted child were to persist in the prohibited behavior.
Parents seeking a cochlear implant for their child completed an extensive behavioral and psychological
evaluation as part of a presurgical evaluation. This evaluation included a number of questionnaires,standardized tests, and interviews that were included in the implant team’s determination of acceptabilityfor implantation. In most instances this test battery was administered in a single day. If the child wasto be implanted, this evaluation typically occurred within 90 days of surgery. Among the instrumentsadministered to the parents was the APT.
Parents and their deaf children who were recruited at BTNRH completed the same protocol as implant
candidates and parents evaluated at The University of Iowa. Although the test protocol was the same, thecircumstances of the evaluation were somewhat different. While both the implant candidate families andthe parents of deaf children at BTNRH had volunteered to participate in research, the parents seekingan implant were likely to be motivated to educe a favorable evaluation from the implant team. Thatis, the psychological evaluation for implant candidate families was part of a screening protocol. TheBTNRH subjects had no extraneous motivation to achieve an outcome from the evaluation. Of the mothersof eligible children who were informed of the project and invited to participate, approximately 65%participated. Disinterest or scheduling difficulties were the reasons for nonparticipation.
Mothers of the normally hearing children were approached while their child was participating in a
laboratory task designed to measure perceptual and motor skills or decision-making. These mothers wereinvited to participate in “a study of parental perceptions of child behavior” that could be completed while
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
their child completed the cognitive or motor tasks in the adjacent laboratory. Approximately 87% of themothers who were invited agreed to participate. Following the informed consent procedure, the motherswho agreed to participate immediately completed a brief questionnaire about the demographics of theirfamily followed by the APT. Virtually all of the mothers of the normally hearing children who declinedto participate indicated they had a specific conflict at that time. Typically these mothers had planned otheractivities in the community (e.g., shopping, transporting a sibling to an after school activity) during thetime their child was participating in the laboratory task. Although a full complement of demographicinformation was not available from those who declined to participate, based on available information andextensive experience with families recruited from the registry, there is no reason to believe that those whodeclined to participate in the current study were distinguishable from those who volunteered to participate. Moreover, the specifics of the task itself seemed irrelevant to the decision not to participate. That is, anindication of an unavailability to participate usually preceded a description of the actual procedure.
Prior to the conduct of the planned analyses of the APT using one-way ANOVAs, the three groups
of mothers were contrasted with respect to the demographic characteristics of their households. Thesepreliminary analyses used one-way ANOVA for continuous variables (e.g., number of children in thehousehold) and Chi Square tests of association for categorical variables (e.g., single parenthood; socialclass; No group differences approached statistical significance (all p’s > .27). Thus,although there were some apparent differences among groups (i.e., lower SES mothers in the two groupsof mothers of deaf children), those apparent group differences did not approach statistical significance,obviating any need to control for demographic variables in the planned analyses.
The first analysis was based on the mean number of scenes for which the groups of mothers selected
a form of physical discipline to alter the behavior of the depicted child. The mothers of the normallyhearing children rarely endorsed the use of physical discipline across the 28 scenes (Mean = .37, SD =.53) while the mothers seeking a cochlear implant and the mothers of the deaf children not seeking animplant only occasionally endorsed the use of physical discipline (Implant Group Mean = 2.72 [SD =1.26]; Deaf Child Group = 3.05 [SD = 1.31]). Because of the large number of zero scores among all groups,the physical discipline scores were transformed using logn(x + 1) to meet the assumptions of analysisof variance and reduce heterogeneity of variance. A one-way analysis of variance of thetransformed physical discipline scores indicated there was a statistically significant difference amonggroups of mothers, F(2/102) = 5.01, p < .01. Follow-up tests using the Tukey HSD (p < .05) indicated thatthe two groups of mothers of deaf children did not differ from each other, but that both groups of mothers ofdeaf children had higher physical discipline scores than the group of mothers of normally hearing children.
To determine whether the three groups differed with respect to how they reacted to various types of
child transgressions, based on the work of and because the “normative” scenes didnot evoke physical discipline in any of the groups, the physical discipline scores of the three groupswere contrasted with respect to the three type-of-transgression scenes (i.e., destructive, dangerous, ruleviolations) in a 3 × 3 mixed analysis of variance, with group membership as the between-subjects factorand scene type as the within-subjects factor As shown in main effects for group membership,F(2/103) = 4.97, p < .01 and scene type, F(2/206) = 13.08, p < .001 were obtained. Because theinteraction between scene type and group membership was not statistically significant, F(4/206) = 2.11,
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Figure 1. The mean number of scenes within scene-type that resulted in a physical disciplinary response by each group ofmothers.
simple effects tests were not conducted. Based on Tukey HSD follow-up tests, regardless of scene type,the two groups of mothers of deaf children endorsed more physical discipline in response to the slidedepictions of child transgressions than did the mothers of the normally hearing children (p < .05). Theendorsement of physical discipline in response to scenes of dangerous or destructive child behaviors didnot differ, but the endorsement of physical discipline in response to the destructive and dangerous sceneswas significantly greater than physical discipline in response to the rule violation scenes.
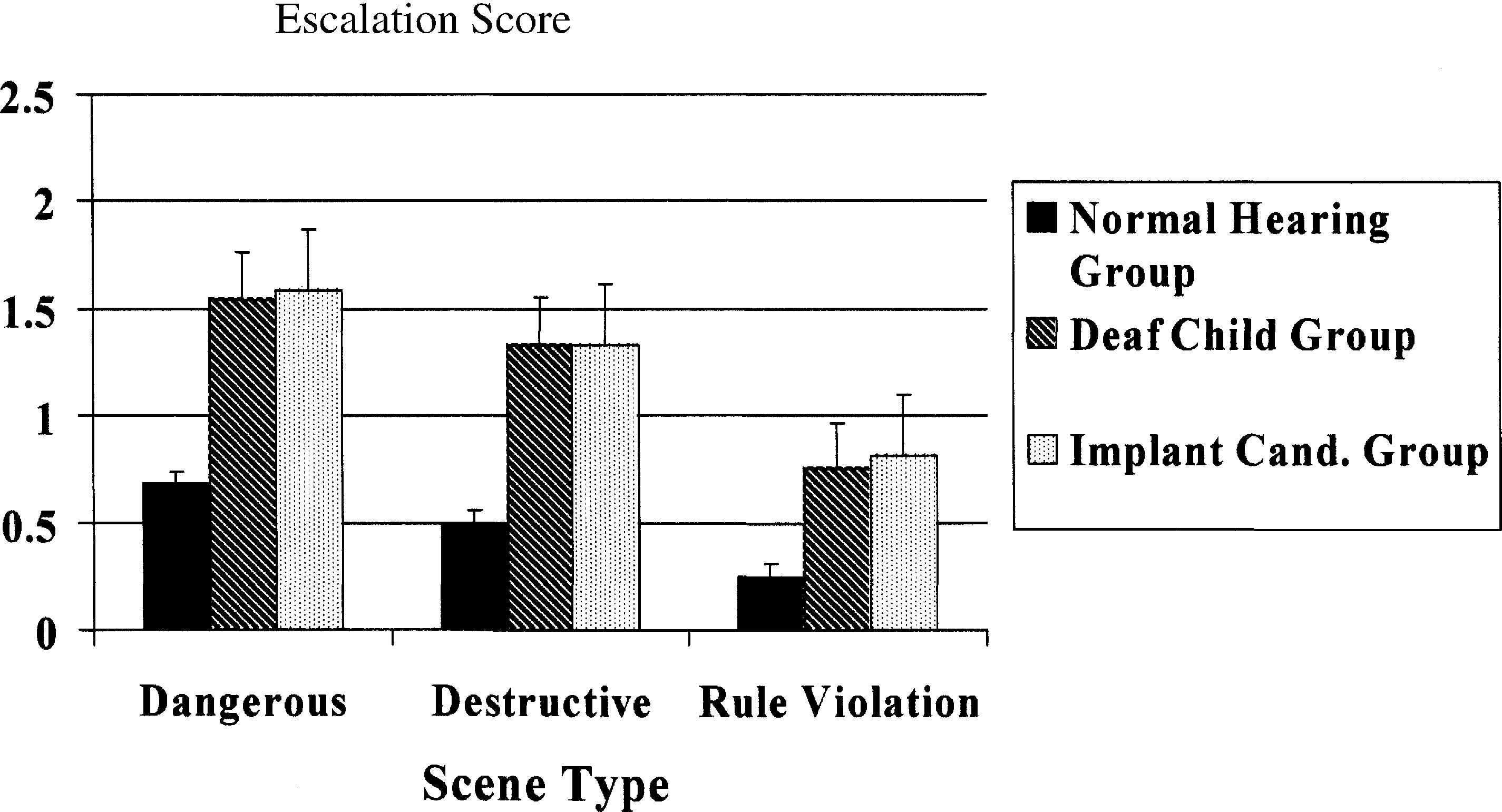
Figure 2. The mean number of scenes within scene-type that resulted in an escalated response by each group of mothers. Escalation entailed a shift from nonphysical to physical discipline, or from mild physical discipline to potentially injuriousphysical discipline. J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Based on the work of analysis of escalated discipline was completed
by computing an escalation score in response to the destructive, dangerous, and rule-violating scenes. Escalation was coded for a specific scene if the mother shifted from an initial response of nonphysi-cal discipline to a physical disciplinary choice in response to repetitions of the transgression, or if themother shifted from spanking to a more potentially injurious form of physical discipline. Again, thelogn(x + 1) transformation was used so the distributions met the assumptions for the statistical tests. As shown in although there was a statistically significant influence of parent group F(2/103)= 5.43, p < .01 on the escalation scores, the statistically significant interaction between parent groupand scene type F(4/206) = 7.87, p < .001 compromised the interpretability of that main effect. Follow-up tests using the Tukey HSD (p < .05) indicated that mothers of the hearing-impaired children weremore likely to escalate their disciplinary response to the dangerous and destructive scenes than the rule-violating scenes. Also, the mothers of deaf children were more likely to escalate in response to thosedangerous and destructive scenes than were the mothers of normally hearing children. The apparent dif-ference in escalation among scenes by the mothers of the normally hearing children was not statisticallysignificant. Discussion
The findings of the present study provide evidence that mothers who were rearing a child with a
profound hearing loss are more likely to endorse the use of physical discipline in response to depictedchild transgressions and more likely to escalate that discipline in response to destructive or dangerous actsthan were mothers of normally hearing children. Thus, the findings are consistent with the hypothesizedlink between rearing a communicatively-impaired child and risk of physical abuse (cf., Importantly, the APT does notindicate the hearing status of the depicted child. Thus, the greater endorsement of physical discipline bythe mothers of deaf children, while somewhat sensitive to the scenes that were depicted, does not requirethat the depicted children present with a hearing impairment. Thus, the data strongly support the notionthat rearing the deaf child influences the general disciplinary preferences of the parent. These findingsare consistent with the conclusion that parents of deaf children aremore reliant on physical discipline. More importantly, the data are consistent with ecological models ofchild development (e.g., and the notion that child attributes can influence the disciplinary strategies of the parent The escalated disciplinary choices of the mothers of the deaf children are also consistentwith the discipline-mediated model of physical abuse advanced by
Although the dependent variable in this research is an analog of some disciplinary contexts confronted
by parents, the use of analog tasks in the study of clinical problems has a long tradition and has provideduseful information about clinical problems that are not readily studied in the natural habitat (see Moreover, the use of laboratory analogs to study discipline and parental affect has been productivein studies of clinical and nonclinical populations (e.g., Although a direct observational approach to studying discipline would provide moreinformation about both parent behavior and evocative child attributes, such a research strategy would beneither practical nor feasible in most research contexts. Within the context of the limitations of the analog
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
test, the current findings strongly support the notion that deaf children are at increased risk of severephysical discipline. Additionally, because discipline tends to be family specific rather than child specific(cf., the present findings also suggest that siblings of hearing-impaired children could be at increased risk of severe physical discipline. In that context it is important tonote that the vast majority of the mothers of deaf children in the present study also had a normally hearingchild in the household. There was not sufficient power to contrast mothers of a single child with mothersof multiple children, nor to determine the possible role of the presence of an older or younger sibling. Thus, with the power available in the present study, it is impossible to determine whether the presence ofnormal hearing siblings play a buffering role in the discipline patterns of parents of a deaf child.
The generalizability of the present findings depends, in part, on the representativeness of the samples
recruited. The sample of mothers of cochlear implant candidates is based on consecutive referrals andis unselected. Thus, although the sample is somewhat geographically constrained, that sample can beseen as representative of mothers of deaf children who sought an implant for their child. The sample ofmothers of deaf children recruited at BTNRH represents a sample that has volunteered to participate inpsychological research, but not necessarily research on child behavior problems or discipline. Althoughreceiving modest compensation, they did not receive any clinical service from their participation. Thus,from the standpoint of the present findings, the mothers who enrolled in this project at BTNRH canbe considered to be representative of the population of mothers of profoundly deaf children receivingservices at that site, they are mothers who evidence a high degree of volunteerism and an interest in theirchildren’s experiences. The sample of mothers of normally hearing children are drawn from a populationof families who had enrolled their children in a psychological research registry. Children recruited fromthat registry for research in the Department of Psychology are typically compensated, but their parentsare rarely compensated. Thus, the mothers in that group are clearly characterized by a high degree ofvolunteerism and probably a high degree of interest in the experiences of their children. If “volunteerism”and an interest in child experiences influences disciplinary preferences, both the BTNRH sample and thecommunity sample share that high degree of volunteerism and an interest in their children’s experiences. The absence of a difference between the two groups of mothers of deaf children and the magnitude ofthe difference between the BTNRH sample and the control sample suggests that volunteerism per se isnot likely to have influenced the outcome of the study. Additionally, although lower class families wereincluded in the two samples of mothers of deaf children but not in the families of hearing children, thesmall number of lower class families in the two samples of mothers of deaf children cannot accountfor the difference between the mothers of deaf children and the mothers of normally hearing children. Because the mothers of implant candidates completed the APT in a presurgical screening protocol, thosemothers could have been motivated to place themselves in the best possible light. The fact that there wereno differences between the two groups of mothers of deaf children suggests that such motivation did notoperate to influence the responding to the APT. The lack of difference between the two groups of mothersof deaf children is consistent with other data showing comparability of parents of deaf children regardlessof their implant-seeking status (e.g., Certainly the data do notsuggest that implant seeking parents approached discipline differently than parents who elect not to seekan implant for their deaf child.
Although the informed consent procedure assured that all mothers knew about the tasks in which
they would be participating, their initial motivation to participate in research was neither child behaviorproblems nor disciplinary concerns. Thus, there is reason to believe that the obtained results are notattributable to a subject selection bias or a sampling bias, or a difference in volunteerism between the
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
mothers of hearing children and the mothers of deaf children. Assuming the samples are representativeof mothers of deaf children, the findings that mothers who were rearing a child with a profound hearingloss are more likely to endorse the use of physical discipline and more likely to escalate that disciplinecan be used to argue for efforts to reduce the use of physical discipline by parents of deaf children andchildren with serious communication difficulties. Acknowledgement
The assistance of Steve Berthoff, Rhonda C. Boyd, Shawna Ehlers, Kathleen Murray, Mary Bower
Russa, Mary Beth Selner-O’Hagen and Rebecca Wald is gratefully acknowledged. References
Ammerman, R. T. (1991). The role of the child in physical abuse: A reappraisal. Violence and Victims, 6(2), 87–101. Ammerman, R. T., & Patz, R. J. (1996). Determinants of child abuse potential: Contribution of parent and child factors. Journalof Clinical Child Psychology, 25, 300–307.
Ammerman, R. T., Van Hasselt, V. B., & Hersen, M. (1988). Maltreatment of handicapped children: A critical review. Journalof Family Violence, 3, 53–72.
Benedict, M. I., Wulff, L. M., & White, R. B. (1992). Current parental stress in maltreating and nonmaltreating families of
children with multiple disabilities. Child Abuse & Neglect, 15, 155–163.
Balkany, T. (1996). Ethics of cochlear implantation in young children. Otolaryngology—Head and Neck Surgery, 114, 748–755. Benson, B. A., Gross, A. M., Messer, S. C., Kellum, G., & Passmore, L. A. (1991). Social support networks among families of
children with craniofacial anomalies. Health Psychology, 10, 252–258.
Boyd, R. C., Knutson, J. F., & Dahlstrom, A. (2000). The social interaction of pediatric cochlear implant recipients with age-
matched peers. Annals of Otology, Rhinology and Laryngology, 109(12, Part 2), 105–109.
Bronfenbrenner, U., & Ceci, S. (1994). Nature-nurture re-conceptualized in developmental perspective: A bio-ecological model. Psychologoical Review, 101, 568–586.
Coon, K. B., Beck, F. W., & Coon, R. C. (1980). Implications for evaluating abused children: An independent study of the
frequency of abused children referred to and enrolled in special education classes in a major Southeastern United Statesmetropolitan area. Child Abuse & Neglect, 4, 153–156.
Dadds, M. R., Mullins, M. J., McAllister, R. A., & Atkinson, E. (2003). Attributions, affect, and behavior in abuse-risk mothers:
A laboratory study. Child Abuse & Neglect, 27, 21–45.
Embry, L. H. (1980). Family support for handicapped preschool children at risk for abuse. In J. J. Gallagher (Ed.), Parents andfamilies of handicapped children (pp. 29–58). San Francisco: Jossey-Bass.
Fagot, B. I. (1992). Assessment of coercive parent discipline. Behavioral Assessment, 14, 387–406. Greenwald, R. L., Bank, L., Reid, J. B., & Knutson, J. F. (1997). A discipline-mediated model of excessively punitive parenting. Aggressive Behavior, 23, 259–280.
Hollingshead, A. B. (1975). Four factor index of social status. Unpublished manuscript, Yale University. Kazdin, A. E. (1978). Evaluating the generality of findings in analogue therapy research. Journal of Consulting and ClinicalPsychology, 46, 673–686.
Knutson, J. F., & Bower, M. E. (1994). Physically abusive parenting as an escalated aggressive response. In M. Potegal & J. F.
Knutson (Eds.), The dynamics of aggression: Biological and social processes in dyads and groups (pp. 195–225). Hillsdale,NJ: Erlbaum.
Knutson, J. F., & Schartz, H. A., (1997). Physical abuse and neglect of children. In T. A. Widiger, A. J. Frances, H. A. Pincus, R.
Ross, M. B. First, & F. W. Davis (Eds.), DSM-IV sourcebook (Vol. 3, pp. 713–804). Washington, DC: American PsychiatricAssociation.
Knutson, J. F., Boyd, R. C., Goldman, M., & Sullivan, P. M. (1997). Psychological characteristics of child cochlear implant
candidates and children with hearing impairments. Ear and Hearing, 18, 355–363. J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Knutson, J. F., Boyd, R. C., Reid, J. B., Mayne, T., & Fetrow, R. (1997). Observational assessments of the interaction of implant
recipients with family and peers: Preliminary findings. Otolaryngology, Head and Neck Surgery, 117, 196–207.
Knutson, J. F., Ehlers, S. L., Wald, R. L., & Tyler, R. S. (2000). Psychological predictors of pediatric cochlear implant use and
benefit. Annals of Otology, Rhinology, and Laryngology, 109(12, Part 2), 100–103.
Knutson, J. F., Schartz, H. A., & Zaidi, L. Y. (1991). Victim risk factors in the physical abuse of children. In R. Banninger (Ed.),
Targets of violence and aggression (pp. 103–155). North Holland: Elsevier Science Publishers B.V.
Knutson, J. F., Wald, R. L., Ehlers, S. L., & Tyler, R. S. (2000). Psychological consequences of pediatric cochlear implant use. Annals of Otology, Rhinology, and Laryngology, 109(12, Part 2), 109–111.
Lane, H., & Bahan, B. (1998). Ethics of cochlear implantation in young children: A review and reply from a deaf-world
perspective. Otolaryngology—Head and Neck Surgery, 119, 297–313.
National Institute of Health. (1995). Cochlear implants: NIH consensus statement (Vol. 13, No. 2). Washington, DC: US
Office of Human Development Services. (1988). Study findings: Study of national incidence and prevalence of child abuse andneglect: 1988. Washington, DC: US Department of Health and Human Services.
Passman, R. H., & Mulhern, R. K., Jr. (1977). Maternal punitiveness as affected by situational stress: An experimental analogue
of child abuse. Journal of Abnormal Psychology, 86(5), 565–569.
Riggins-Caspers, K. M., Cadoret, R. J., Knutson, J. F., & Langbehn, D. (2003). Biology-environment interaction and evocative
biology-environment correlation: Contributions of harsh discipline and parental psychopathology to problem adolescentbehaviors. Behavior Genetics, 33, 205–220.
Rodriquez, C. M., & Sutherland, D. (1999). Predictors of parents’ physical disciplinary practices. Child Abuse & Neglect, 23,
Schlesinger, H., & Meadow, K. (1972). Sound and sign: Child deafness and mental health. Berkeley, CA: University of California
Sobsey, D. (1994). Preventing the abuse of people with disabilities: Research and practical implications. Baltimore, MD: Brooks
Starr, R. H., Dietrich, K. N., Fischhoff, J., Ceresnie, S., & Zweier, D. (1984). The contribution of handicapping conditions to
child abuse. Topics in Early Childhood Special Education, 4, 55–69.
Sullivan, P. M., & Knutson, J. F. (1998). The association between child maltreatment and disabilities in a hospital-based
epidemiological study. Child Abuse & Neglect, 22(4), 271–288.
Sullivan, P. M., & Knutson, J. F. (2000). Maltreatment and disabilities: A population-based epidemiological study. Child Abuse
& Neglect, 24, 1257–1274.
Sullivan, P. M., Brookhouser, P. E., Scanlan, J. M., Knutson, J. F., & Schulte, L. E. (1991). Patterns of physical and sexual abuse
of communicatively handicapped children. Annals of Otology, Rhinology, and Laryngology, 100, 188–194.
Vasta, R., & Copitch, P. (1981). Simulating conditions of child abuse in the laboratory. Child Development, 52, 164–170. Verdugo, M. A., Bermejo, B. G., & Fuertes, J. (1995). The maltreatment of intellectually handicapped children and adolescents. Child Abuse & Neglect, 19, 205–215.
Westat, Inc. (1993). A report on the maltreatment of children with disabilities. Washington, DC: National Center on Child Abuse
Wever, C. C. (2002). Parenting deaf children in the era of cochlear implantation: A narrative-ethical analysis. Thesis. Nijmegen,
The Netherlands: University of Nijmegen.
Whitmore, E. A. W., Kramer, J. R., & Knutson, J. F. (1993). The association between punitive childhood experiences and
hyperactivity. Child Abuse & Neglect, 17, 357–366.
Winer, B. J. (1971). Statistical principles in experimental design (2nd ed.). San Francisco, CA: McGraw-Hill. Zaidi, L. Y., Knutson, J. F., & Mehm, J. G. (1989). Transgenerational patterns of abusive parenting: Analog and clinical tests. Aggressive Behavior, 15, 137–152. R´esum´e Objectif: ´
Evaluer les diff´erentes formes de discipline que pr´ef`erent des m`eres d’enfants profond´ement
sourds et d’enfants entendants, au moyen d’un test qui propose des liens entre les handicaps infantiles etles comportements punitifs des parents. J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937M´ethode: On a ´evalu´e trois groupes de m`eres par rapport `a la forme de discipline qu’elles pr´ef`erent: celles qui cherchaient un implant cochl´eaire pour leur enfant sourd (n = 22); celles qui ne cherchaient pas `a obtenir un implant pour leur enfant (n = 57); et celles dont les enfants ´etaient entendants (n = 27). On a assign´e aux m`eres des tˆaches semblables o`u il s’agissait de choisir un type de discipline en r´eaction
`a des diapositives montrant des enfants qui se comportent normalement ou qui sont clairement d´eviants
et irritants. R´esultats: Les r´esultats indiquent que les m`eres des enfants profond´ement sourds sont plus aptes `a choisir une discipline corporelle et plus aptes aussi `a intensifier leur discipline corporelle lorsque l’enfant persiste dans son comportement insupportable. De plus, cette intensification est plus probable lorsqu’il s’agit de situations o`u les enfants s’adonnent `a des comportements dangereux et destructeurs que dans des situations o`u ils enfreignent un r`eglement quelconque. Conclusions: On a not´e une coh´erence entre les constats et: l’hypoth`ese voulant que les handicaps infantiles et la maltraitance soient li´es; et aussi l’hypoth`ese que les enfants handicap´es qui ont des probl`emes de communication sont `a risque d’ˆetre maltrait´es. Objetivo: Evaluar las preferencias disciplinarias de las madres de ni˜nos profundamente sordos y ni˜nos con audici´on normal con la intenci´on de valorar la uni´on entre la presencia de minusval´ıas y mayor presencia de castigo f´ısico. M´etodo: Se evaluaron las preferencias disciplinarias de un grupo de madres que consultan para un implante coclear para sus hijos sordos profundos (n = 57), un grupo de madres que no consultan por este implante para sus hijos sordos (n = 22) y un grupo de madres con hijos con audici´on normal (n = 27) utilizando una tarea an´aloga en la cual los sujetos seleccionaron disciplinas en respuesta a diapositivas de ni˜nos que realizan conductas normales o claramente desviadas que son potencialmente irritantes. Resultados: Las madres de los ni˜nos con alteraciones profundas de la audici´on ten´ıan m´as tendencia para seleccionar la disciplina f´ısica en respuesta a las transgresiones infantiles y m´as tendencia a escalar hacia la disciplina f´ısica cuando el ni˜no es presentado como persistente en la transgresi´on. Adem´as, la escalada agresiva era m´as probable en respuesta a escenas que presentan al ni˜no implicado en actos peligrosos y destructivos que en actos que violan las normas. Conclusiones: Los hallazgos fueron consistentes con la hipot´etica uni´on entre minusval´ıas infantiles y el maltrato infantil. Se apoya adem´as la hip´otesis de que los ni˜nos con minusval´ıas asociadas a problemas de comunicaci´on pueden tener un mayor riesgo de maltrato f´ısico.
Gastroclin – Clínica de Endoscopia Digestiva e Gastroenterologia Rua Santo Antônio, 630 – 4º e 6º andares - Centro ORIENTAÇÕES PARA O PREPARO Exame: Colonoscopia Diagnóstica ou Terapêutica (período tarde) Data do Exame: ______/______/ __________ . Hora : 13:30 h Médico responsável: Dr. Frederico Almeida Baptista de Oliveira CRM: 21.346 IMPORTANTE A Colonoscopia é
FOR IMMEDIATE RELEASE PIONEER IN ADDICTION TREATMENT SUPPORTS PROPOSED RESEARCH Dr. Sheila Blume Advocates Testing Baclofen for Alcohol Dependence Bridport, VT – February 26, 2013 – The Foundation for Alcoholism Research (FAR) announces that Sheila Blume, MD endorses the FAR campaign to fund a study on the effects of the medication Baclofen on alcohol dependence. The N
 Child Abuse & Neglect 28 (2004) 925–937
Disciplinary choices of mothers of deaf children
and mothers of normally hearing childrenଝ
John F. Knutson, Christina R. Johnson, Patricia M. Sullivan
a Department of Psychology, The University of Iowa, E-11 Seashore Hall, Iowa City, IA 52240, USA
b Boys Town National Research Hospital, Omaha, NE, USA
Received 18 March 2003; received in revised form 6 April 2004; accepted 7 April 2004
Abstract
Child Abuse & Neglect 28 (2004) 925–937
Disciplinary choices of mothers of deaf children
and mothers of normally hearing childrenଝ
John F. Knutson, Christina R. Johnson, Patricia M. Sullivan
a Department of Psychology, The University of Iowa, E-11 Seashore Hall, Iowa City, IA 52240, USA
b Boys Town National Research Hospital, Omaha, NE, USA
Received 18 March 2003; received in revised form 6 April 2004; accepted 7 April 2004
Abstract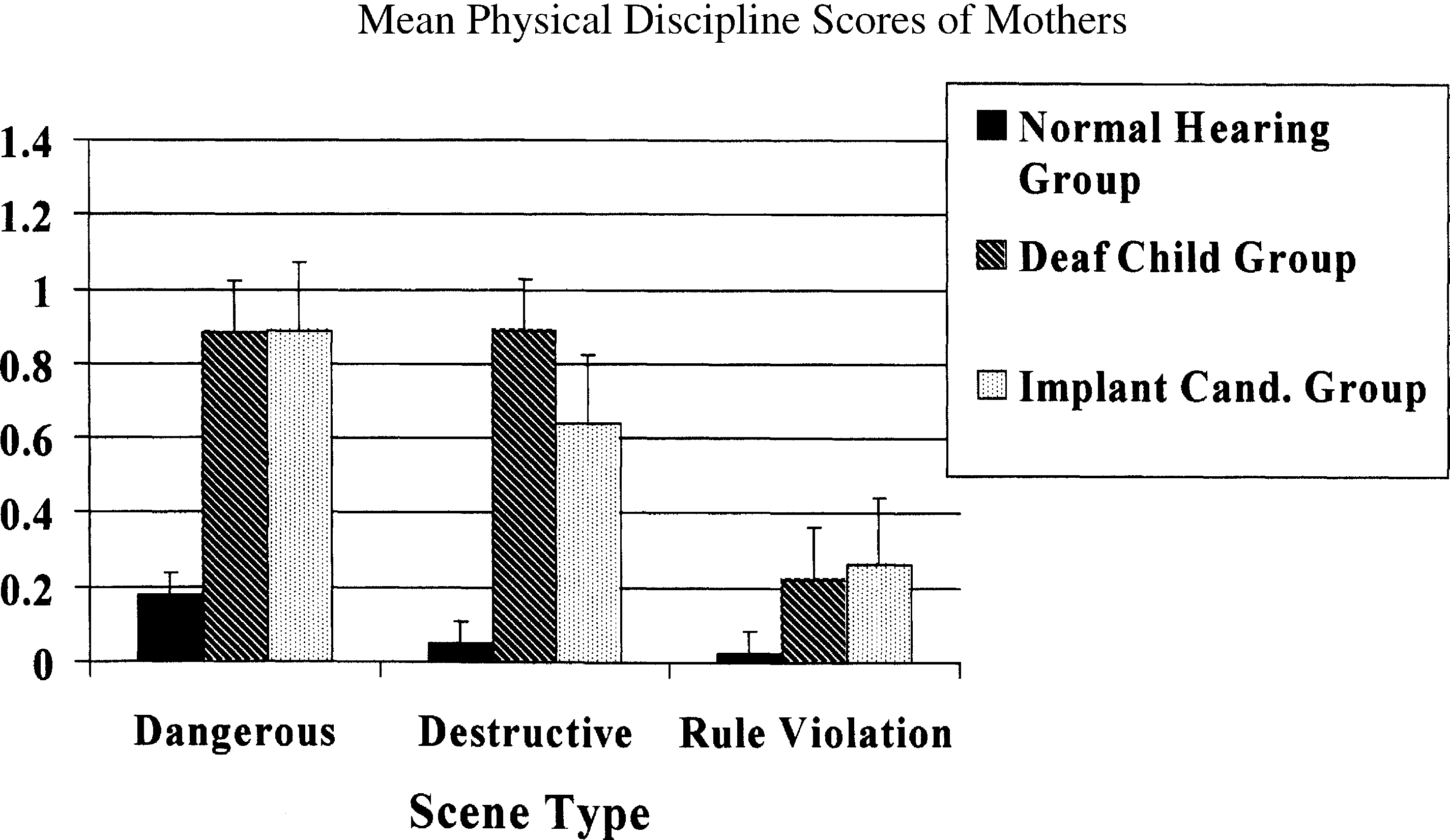
 J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Figure 1. The mean number of scenes within scene-type that resulted in a physical disciplinary response by each group ofmothers.
J.F. Knutson et al. / Child Abuse & Neglect 28 (2004) 925–937
Figure 1. The mean number of scenes within scene-type that resulted in a physical disciplinary response by each group ofmothers.