Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Microsoft powerpoint - katz-wilfert clinical case-erin staples.ppt
• 12-year-old male presents with an eight-
– Started with right hip and leg pain eight
– Developed subjective fevers 2 days into
– Day after fever the right hip and leg pain
• Seen by his primary care doctor same
• Leg pain continued to increase, and by
the fifth day, he had persistent daily fevers
• Admitted to District Hospital on day 5
– Given pain meds and unknown IV antibiotic– The fevers went away, but the pain
further evaluation then two days later to tertiary care center
1. Asthma on Singulair, Zyrtec, Advair, and
Lives in Southeastern NC. He is in seventh
grade. He has two older siblings. No pets
– Fevers, no Δ weight or night sweats– Cold symptoms 2 weeks prior to hip pain onset,
– No CV or resp problems other than asthma (no
– No vomiting, diarrhea, or constipation– No problems with urination– Significant hip pain, difficulty standing, and he is
• VS: T 36.1, HR 67, RR 16, BP 112/61, Wt 50 kg
• HEENT and Neck: Normal except for halitosis
• CV: Regular S1 and S2 without murmurs
• Abdomen: Soft, NT, ND, BS present, no masses
– Sacroiliac tenderness R > L– Tenderness with compression of bilateral iliac crests– No trochanter tenderness– ROM limited on his R hip on flexion and extension– Int and ext rotation produce significant pain in SI area– Knee joints normal without effusion– Rest of extremities reveal no swollen joints, NT, full ROM– 2+ DP and 2+ radial pulses bilaterally
• Neurologic: Strength appears normal, but significantly
• With OM, 35% had leukocytosis at admission
• Inflammatory markers (ESR, CRP) are ↑ in > 90%
– Can be used to follow response to therapy– CRP and ESR often ↑ in first 2-5 days after initiation of
therapy and return to normal within 1 (CRP) to 3 (ESR)
• Needle aspiration likely to yield an organism in
• Blood cxs yield + results in 36% to 55% of specimens
Very sensitive, even in early Long study, often disease, may reveal pus
septic arthritis of his sacroiliac joint and a psoas abscess
• Urinary tract infection• Extracorporeal shock
– Bloody, “mild purulent tinge” fluid drained
– Areas irrigated– Fluid sent for culture
– First generation cephalosporin– Clindamycin
– Third generation cephalosporin– Vancomycin
• All cultures grew Coagulase-negative Staphylococcus
• Yes until susceptibility testing is done
• Acts more like CoPS than the indolent CoNS
• Can cause many types of infection, ranging from
superficial skin infections to life-threatening
• Frequently beta-lactamase-negative and thus
susceptible to penicillin. Most isolates susceptible to
antibiotics such as clindamycin, erythromycin, TMP-
Surveillance Summaries Giardiasis Surveillance United States, 1992–1997 U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES Centers for Disease Control and Prevention (CDC) Continuing Medical Education for U.S. Physicians and Nurses August 11, 2000 The MMWR series of publications is published by the Epidemiology Program Office,Centers for Disease Control and Prevention (CDC), U.
ABA Guidance for the Responsible Labeling and Marketing of Energy Drinks BACKGROUND AND OBJECTIVE The American Beverage Association (ABA) is the trade association representing the broad spectrum of companies that manufacture and distribute non-alcoholic beverages in the United States. This Guidance relates to the labeling and marketing of energy drinks. Energy drinks are non-alcohol
 • 12-year-old male presents with an eight-
– Started with right hip and leg pain eight
– Developed subjective fevers 2 days into
– Day after fever the right hip and leg pain
• 12-year-old male presents with an eight-
– Started with right hip and leg pain eight
– Developed subjective fevers 2 days into
– Day after fever the right hip and leg pain
 • Seen by his primary care doctor same
• Leg pain continued to increase, and by
the fifth day, he had persistent daily fevers
• Seen by his primary care doctor same
• Leg pain continued to increase, and by
the fifth day, he had persistent daily fevers
 • Admitted to District Hospital on day 5
– Given pain meds and unknown IV antibiotic– The fevers went away, but the pain
further evaluation then two days later to tertiary care center
• Admitted to District Hospital on day 5
– Given pain meds and unknown IV antibiotic– The fevers went away, but the pain
further evaluation then two days later to tertiary care center
 1. Asthma on Singulair, Zyrtec, Advair, and
Lives in Southeastern NC. He is in seventh
grade. He has two older siblings. No pets
1. Asthma on Singulair, Zyrtec, Advair, and
Lives in Southeastern NC. He is in seventh
grade. He has two older siblings. No pets
 – Fevers, no Δ weight or night sweats– Cold symptoms 2 weeks prior to hip pain onset,
– No CV or resp problems other than asthma (no
– No vomiting, diarrhea, or constipation– No problems with urination– Significant hip pain, difficulty standing, and he is
– Fevers, no Δ weight or night sweats– Cold symptoms 2 weeks prior to hip pain onset,
– No CV or resp problems other than asthma (no
– No vomiting, diarrhea, or constipation– No problems with urination– Significant hip pain, difficulty standing, and he is
 • VS: T 36.1, HR 67, RR 16, BP 112/61, Wt 50 kg
• HEENT and Neck: Normal except for halitosis
• CV: Regular S1 and S2 without murmurs
• Abdomen: Soft, NT, ND, BS present, no masses
• VS: T 36.1, HR 67, RR 16, BP 112/61, Wt 50 kg
• HEENT and Neck: Normal except for halitosis
• CV: Regular S1 and S2 without murmurs
• Abdomen: Soft, NT, ND, BS present, no masses
 – Sacroiliac tenderness R > L– Tenderness with compression of bilateral iliac crests– No trochanter tenderness– ROM limited on his R hip on flexion and extension– Int and ext rotation produce significant pain in SI area– Knee joints normal without effusion– Rest of extremities reveal no swollen joints, NT, full ROM– 2+ DP and 2+ radial pulses bilaterally
• Neurologic: Strength appears normal, but significantly
– Sacroiliac tenderness R > L– Tenderness with compression of bilateral iliac crests– No trochanter tenderness– ROM limited on his R hip on flexion and extension– Int and ext rotation produce significant pain in SI area– Knee joints normal without effusion– Rest of extremities reveal no swollen joints, NT, full ROM– 2+ DP and 2+ radial pulses bilaterally
• Neurologic: Strength appears normal, but significantly
 • With OM, 35% had leukocytosis at admission
• Inflammatory markers (ESR, CRP) are ↑ in > 90%
– Can be used to follow response to therapy– CRP and ESR often ↑ in first 2-5 days after initiation of
therapy and return to normal within 1 (CRP) to 3 (ESR)
• Needle aspiration likely to yield an organism in
• Blood cxs yield + results in 36% to 55% of specimens
• With OM, 35% had leukocytosis at admission
• Inflammatory markers (ESR, CRP) are ↑ in > 90%
– Can be used to follow response to therapy– CRP and ESR often ↑ in first 2-5 days after initiation of
therapy and return to normal within 1 (CRP) to 3 (ESR)
• Needle aspiration likely to yield an organism in
• Blood cxs yield + results in 36% to 55% of specimens
 Very sensitive, even in early Long study, often disease, may reveal pus
Very sensitive, even in early Long study, often disease, may reveal pus
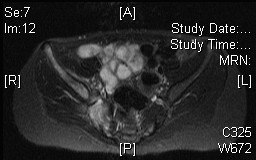
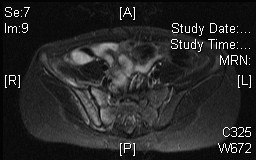 septic arthritis of his sacroiliac joint and a psoas abscess
septic arthritis of his sacroiliac joint and a psoas abscess
 • Urinary tract infection• Extracorporeal shock
• Urinary tract infection• Extracorporeal shock
 – Bloody, “mild purulent tinge” fluid drained
– Areas irrigated– Fluid sent for culture
– Bloody, “mild purulent tinge” fluid drained
– Areas irrigated– Fluid sent for culture
 – First generation cephalosporin– Clindamycin
– Third generation cephalosporin– Vancomycin
– First generation cephalosporin– Clindamycin
– Third generation cephalosporin– Vancomycin
 • All cultures grew Coagulase-negative Staphylococcus
• Yes until susceptibility testing is done
• All cultures grew Coagulase-negative Staphylococcus
• Yes until susceptibility testing is done
 • Acts more like CoPS than the indolent CoNS
• Can cause many types of infection, ranging from
superficial skin infections to life-threatening
• Frequently beta-lactamase-negative and thus
susceptible to penicillin. Most isolates susceptible to
antibiotics such as clindamycin, erythromycin, TMP-
• Acts more like CoPS than the indolent CoNS
• Can cause many types of infection, ranging from
superficial skin infections to life-threatening
• Frequently beta-lactamase-negative and thus
susceptible to penicillin. Most isolates susceptible to
antibiotics such as clindamycin, erythromycin, TMP-