Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Vesicoureteral reflux (vur)
Vesicoureteral Reflux (VUR) Educational Information sheet What is VUR?:
• The reverse or retrograde flow or urine from the bladder, into the ureters, and
generally into the kidney(s). “Backwash”
• Occurs when the “one way valve” mechanism of the ureter is “immature.” • Most cases are congenital (primary) and occur during fetal development. • VUR (secondary) can arise from high pressure bladder situations (neurogenic /
outlet obstruction) or “holding of the urine” as seen with dysfunctional elimination patients.
How severe is it? :
• Graded using numerical system of 1-5. • Grade I (least severe) / Grade V (most severe). • Rates of resolution: Determined by the initial grade OVER 5 years from time of
• Resolution rates are same for duplicated renal systems (two ureters from one
• Grade I = 90%, II = 70%, III = 50%, IV = 30%, V = 10-15%
Grades of VUR Any Hereditary Component? :
• Affects approximately 1% of “healthy” children. • Can occur in up to 40-45% of siblings with VUR. (Should siblings be screened
early in life? –still remains to be a controversial issue in pediatric practice.)
• If parent had VUR, approx 50% of refluxer’s children will be affected. • Runs in families—but generally occurs in 1:100 live births. • Incidence is higher in infants than in older children.
• The severity is usually greater in infants and males. • Most cases are usually found by UTI at 2-3 years of age. • Affects girls more than boys at a 6:1 ratio.
Why the concern with VUR? :
• A urinary tract infection (UTI) is a bacterial infection any where along the urinary
tract involving bladder (cystitis) OR kidneys (pyelonephritis).
• TAKE HOME MESSAGE: Reflux does not cause UTIs and UTIs don’t cause
• Reflux of sterile urine to kidney is generally not a problem in an otherwise
• VUR can be damaging without infection in an abnormally “high pressure” urinary
• However, when infected urine(bladder infection) refluxes to a kidney the result is
• Result is usually a very sick child with HIGH fever, vomiting, lethargy, pain.
• Increased risk of permanent kidney damage and irreversible scarring with each
• Risk of scarring DECREASES as child approaches 5-7 yo.
What tests or studies are needed to diagnose? :
• Standard work-up for “first time febrile UTI” is
1) Renal Ultrasound (RUS) 2) Voiding Study (VCUG as initial study to grade or NCG for follow-up).
• RUS shows how kidneys LOOK (size, shape, “dilation/swelling” or
• Voiding cystourethrogram (VCUG) requires a catheter in the bladder. More
specific for GRADING the level of VUR (100 times more radiation exposure than NCG).
• Nuclear cystogram (NCG) requires a catheter too, but only shows if VUR is
GONE or PRESENT. Poor for grading / good for follow-up. (100 times less radiation exposure).
• Nuclear Renal Scan (DTPA/Glucoheptonate) requires IV access and catheter.
Estimates kidney function, and GFR. Can evaluate for any scarring changes.
What is the CONSERVATIVE management of VUR? :
• Education of the condition to the family and patient. • Education of family on identification of UTI risk factors. • Treat ANY dysfunctional elimination habits (correct poor peeing, pooping,
• Prophylactic (once daily) low dose antibiotics. First line choice = BACTRIM • This small amount of medication concentrated in bladder to keep urine sterile is
• Yearly voiding studies to check for resolution or worsening.
When would VUR need surgical repair? :
Catheterized, culture-documented “breakthrough” UTI.
Allergic to all prophylactic antibiotics. 5 years of observation with NO resolution. Complications of poor compliance with set management “plan of care”.
What is AGGRESSIVE / SURGICAL management of VUR? :
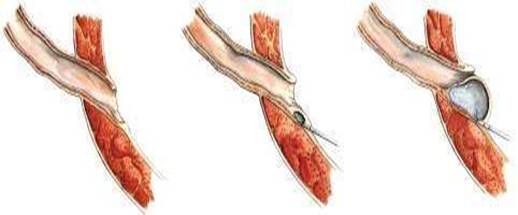
• DEFLUX injection: Otherwise known as the “sting” procedure – Done under
A quick 15-20 minute outpatient procedure. Done via cystoscope (lighted camera in bladder, no incision). Injection of “bulking material / DEFLUX” in the ureteral orifice. Virtually NO recovery time & NO hospital stay. Success rates: Generally 70%-80% with first time injection and greater than
Success rates are generally higher with the lower grades of VUR.
Success rates are slightly lower with anatomic abnormalities (ureteral
Anesthesia: General – can last 3-6 hours. Incision site: “Bikini line” with open procedure. Requires longer RECOVERY time (1-2 weeks) & short 1 day stay in hospital.
• Generally, “younger the child – quicker the recovery.”
Requires the bladder to be opened to reimplant and tunnel the ureters deeper
Success rate: As high as 98% with normal caliber ureters. Success at 93% if
Before surgery No aspirin or ibuprofen for 7 days before surgery (review all medications with your surgeon prior to surgery). After Open Surgery There will be a clear plastic dressing over the wound with several small steristrips underneath. It is not uncommon to see some blood or fluid collect under this dressing, this is normal. This dressing should come off on it’s own after about 7 days. If it does not or has not come off completely it is OK to remove it at that point. There are under the skin and will dissolve on their own. Shower or bath 24 hours after surgery is permitted. A Foley catheter will be placed during surgery that will come out the morning after surgery. Your child will need to void every 2 hours after the catheter is removed. Your child will be allowed to drink fluid the night after surgery and typically return to a normal diet in the morning.
The hospital stay is typically 1 day. Constipation is very common after surgery, but it is important to try and avoid. High water intake and stool softeners will help avoid constipation. You will need to continue prophylactic antibiotics until the follow up images prove resolution of the reflux. Medications at discharge: Ibuprofen as needed for pain Tylenol with codeine for more severe pain Pyridium for 2 days (this is for bladder pain and will turn the urine orange) Medication Most children do well with Ibuprofen (and Tylenol for pain, we recommend that you alternate these every 2 hours for the first 24 to 48 hours (only when child is awake) to keep your child comfortable. (Remember, never give the same medicine type more than once every 4 hours.)
Dosing chart (for Tylenol and Ibuprofen) Example
For children older than 1 year, you will have a prescription for Tylenol with codeine for more severe pain. Follow up (follow up from date of surgery) 3 weeks for a Renal Ultrasound 3 months with a renal ultrasound 6 months with a renal ultrasound and nuclear cystogram.
If STENT = 4 weeks Cystourethroscopy and stent removal 3 weeks after stent removal for a nuclear renal scan (lasix/NO cath) 3 months with a renal ultrasound 6 months with a renal ultrasound and nuclear cystogram.
After Deflux Your child should have very minimal discomfort after this procedure. Expect some burning with urination for the first couple of voids after surgery. It is normal to have some blood in the urine for a few days after surgery. Your child should void every 2 to 3 hours while awake for the first 24 hours after surgery (you do not need to wake your child up at night to void). Drink lots of fluids for a few days after surgery. You may resume bathing the day of surgery.
Medications at discharge: Ibuprofen as needed for pain Pyridium for 2 days (this is for bladder pain and will turn the urine orange)
3 weeks with Renal Ultrasound 2 months with a Nuclear Cystogram (NCG)
Contact information University of Oklahoma Children’s Hospital Out-patient surgery 405-271-4130 Weekdays 8am – 5pm Pediatric Urology Clinic 405-271-3800 After 5 pm and weekends Hospital operator 405-271-5656 (ask for pediatric Urology Doctor on-call)
framing how we think about our moneydecember 2012 “I used to think that the human brain was the most fascinating part of the body. Then I thought, what part of my body is telling me that?” “Rose coloured glasses are never made in bifocals. - Erno Philips (American entertainer/Actor) Nobody ever wants to read the small print in dreams.” - Ann Landers (Agony-aunt for the Ch
The MSCI USA Investable Market Index (IMI) Utilities is designed to capture the large, mid and small cap segments of the US equity universe. All securities in the index are classified in the Utilities sector as per theGlobal Industry Classification Standard (GICS®). Cumulative Index Performance — Gross Returns (Feb 1999 – Feb 2014) — USDIndex Performance — Gross Returns (%) (Februar
 Vesicoureteral Reflux (VUR)
Vesicoureteral Reflux (VUR) 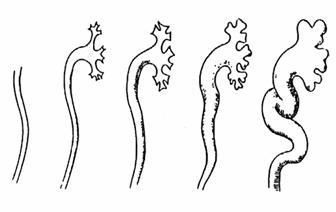 Any Hereditary Component? :
Any Hereditary Component? : 








 • Standard work-up for “first time febrile UTI” is
1) Renal Ultrasound (RUS) 2) Voiding Study (VCUG as initial study to grade or NCG for follow-up).
• RUS shows how kidneys LOOK (size, shape, “dilation/swelling” or
• Voiding cystourethrogram (VCUG) requires a catheter in the bladder. More
specific for GRADING the level of VUR (100 times more radiation exposure than NCG).
• Nuclear cystogram (NCG) requires a catheter too, but only shows if VUR is
GONE or PRESENT. Poor for grading / good for follow-up. (100 times less radiation exposure).
• Nuclear Renal Scan (DTPA/Glucoheptonate) requires IV access and catheter.
Estimates kidney function, and GFR. Can evaluate for any scarring changes.
What is the CONSERVATIVE management of VUR? :
• Standard work-up for “first time febrile UTI” is
1) Renal Ultrasound (RUS) 2) Voiding Study (VCUG as initial study to grade or NCG for follow-up).
• RUS shows how kidneys LOOK (size, shape, “dilation/swelling” or
• Voiding cystourethrogram (VCUG) requires a catheter in the bladder. More
specific for GRADING the level of VUR (100 times more radiation exposure than NCG).
• Nuclear cystogram (NCG) requires a catheter too, but only shows if VUR is
GONE or PRESENT. Poor for grading / good for follow-up. (100 times less radiation exposure).
• Nuclear Renal Scan (DTPA/Glucoheptonate) requires IV access and catheter.
Estimates kidney function, and GFR. Can evaluate for any scarring changes.
What is the CONSERVATIVE management of VUR? :




 Success rates are slightly lower with anatomic abnormalities (ureteral
Anesthesia: General – can last 3-6 hours. Incision site: “Bikini line” with open procedure. Requires longer RECOVERY time (1-2 weeks) & short 1 day stay in hospital.
• Generally, “younger the child – quicker the recovery.”
Requires the bladder to be opened to reimplant and tunnel the ureters deeper
Success rate: As high as 98% with normal caliber ureters. Success at 93% if
Before surgery
Success rates are slightly lower with anatomic abnormalities (ureteral
Anesthesia: General – can last 3-6 hours. Incision site: “Bikini line” with open procedure. Requires longer RECOVERY time (1-2 weeks) & short 1 day stay in hospital.
• Generally, “younger the child – quicker the recovery.”
Requires the bladder to be opened to reimplant and tunnel the ureters deeper
Success rate: As high as 98% with normal caliber ureters. Success at 93% if
Before surgery 
 After Deflux Your child should have very minimal discomfort after this procedure. Expect some burning with urination for the first couple of voids after surgery. It is normal to have some blood in the urine for a few days after surgery. Your child should void every 2 to 3 hours while awake for the first 24 hours after surgery (you do not need to wake your child up at night to void). Drink lots of fluids for a few days after surgery. You may resume bathing the day of surgery.
Medications at discharge: Ibuprofen as needed for pain Pyridium for 2 days (this is for bladder pain and will turn the urine orange)
3 weeks with Renal Ultrasound 2 months with a Nuclear Cystogram (NCG)
Contact information University of Oklahoma Children’s Hospital Out-patient surgery 405-271-4130 Weekdays 8am – 5pm Pediatric Urology Clinic 405-271-3800 After 5 pm and weekends Hospital operator 405-271-5656 (ask for pediatric Urology Doctor on-call)
After Deflux Your child should have very minimal discomfort after this procedure. Expect some burning with urination for the first couple of voids after surgery. It is normal to have some blood in the urine for a few days after surgery. Your child should void every 2 to 3 hours while awake for the first 24 hours after surgery (you do not need to wake your child up at night to void). Drink lots of fluids for a few days after surgery. You may resume bathing the day of surgery.
Medications at discharge: Ibuprofen as needed for pain Pyridium for 2 days (this is for bladder pain and will turn the urine orange)
3 weeks with Renal Ultrasound 2 months with a Nuclear Cystogram (NCG)
Contact information University of Oklahoma Children’s Hospital Out-patient surgery 405-271-4130 Weekdays 8am – 5pm Pediatric Urology Clinic 405-271-3800 After 5 pm and weekends Hospital operator 405-271-5656 (ask for pediatric Urology Doctor on-call)