Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Layout
1 9 . D R U G T R E A T M E N T T R I A L S
The science behind the Progeria clinical drug trials
The science behind the Progeria clinical drug trials
There are three drugs currently being studied in treatment trials for Progeria:
3) A bisphosphonate called Zoledronic Acid
All of these drugs work in different places along a common pathway thatwe hope will improve disease symptoms in Progeria.
> How did we get from gene discovery to drug therapy
Finding the gene for Progeria was the key element to this entire avenue ofexploration. This gene is called LMNA, and it normally encodes a proteincalled prelamin A (this protein is further processed and becomes laminA). Children with Progeria have a mutation in LMNA which leads to theproduction of an abnormal form of prelamin A called “progerin.” Manyyears’ worth of basic research on prelamin A and lamin A gave us the ability tounderstand that the drugs administered in this trial may prevent progerinfrom damaging cells and thus reduce the severity of the disease Progeria. Since 2003, research has focused on systematically examining this pos-sibility, first testing these drugs on Progeria cells and then on Progeria mice. 1 9 . 2 T H E P R O G E R I A H A N D B O O K
> How will the drugs work in Progeria?
The protein that we believe is responsible for Progeria is called progerin. In order to block normal cell function and cause Progeria, a molecule calleda “farnesyl group” must be attached to the progerin protein. There are aseries of steps necessary for a cell to make the farnesyl group, and place itonto the progerin protein. Each of the three drugs in this protocol target adifferent step in that process. Pravastatin, Zoledronic Acid, and Lonafarnibact by blocking (inhibiting) the production or the attachment of the farnesylgroup onto progerin (see figure 1). The current clinical trial will evaluatewhether the three drugs administered in this trial can effectively block thisfarnesyl group attachment to progerin with a resulting reduction in diseaseseverity. Since all three drugs work at a different point in the pathway thatleads to the production of the protein that is believed to cause the disease,their combination provides the opportunity to amplify the efficacy over thedrugs used individually.
T h e P r o g e r i a R e s e a r c h F o u n d a t i o n ;
D R U G T R E A T M E N T T R I A L S 1 9 . 3
Lonafarnib is a Farnesyltransferase Inhibitor (FTI). FTIs are a class of
drugs that inhibit an enzyme that is required to attach the farnesyl group
to proteins. Because many proteins that regulate cancer cell growth requirefarnesylation, drug companies have been developing and testing these drugs
to evaluate their effect on cancer cells. Progeria cells are not cancer cells,but progerin is a protein that shares this need to be farnesylated in order to
fully function. The farnesylated form of progerin leads to some of the cellular
damage observed in Progeria. FTIs prevent this farnesyl group attachment,and were therefore evaluated as a possible therapy for Progeria. Lonafarnib
is not approved by the U.S. Food & Drug Administration, and can only begiven through approved clinical trials.
Pravastatin (marketed as Pravachol or Selektine) is a member of the drugclass of statins. It is usually used for lowering cholesterol and preventingcardiovascular disease. Children with Progeria do not usually have highcholesterol. Pravastatin is being used for Progeria because it also has aneffect on blocking the production of the farnesyl molecule that is needed forprogerin to create disease in progeria. The U.S. Food & Drug Administrationapproved Pravastatin for sale in the United States for the first time on April2006. It comes as a tablet that can be crushed into food for administration. It is usually given once daily.
Zoledronic Acid or Zoledronate (marketed under the trade names Zometaand Reclast) is a bisphosphonate. This agent is used to improve bone densityin women with osteoporosis, and to prevent skeletal fractures in peoplesuffering from some forms of cancer. It has been used in children with abone disease called osteogenesis imperfecta, and for other bone problems. Children with Progeria can have low bone density and Zoledronic Acid may,over time, help with that problem. It also has an effect on blocking the production of the farnesyl molecule that is needed for progerin to createdisease in Progeria. The U.S. Food & Drug Administration approved ZoledronicAcid for sale in the United States for the first time on August 2001 for thetreatment of hypercalcemia of malignancy. It is administered intravenouslyseveral times per year. 1 9 . 4 T H E P R O G E R I A H A N D B O O K
> Treating cells in the laboratory: FTI improves Progeria in cell cultures
The nucleus (plural nuclei) is the structure at the center of each cell thatcontains DNA (the genes). Unlike the round nuclei from normal cells, Progeria cells have abnormally shaped nuclei. These abnormally shapednuclei with multiple “lobes” can look like a cluster of grapes or bubbles(see figure 2).
The gene LMNA normally produces a protein called prelamin A. When thisgene is mutated, as occurs in Progeria, it causes abnormal cell shape andfunction that results in the clinical problems that are characteristic of thisdisease. Prelamin A requires a molecule attached to the end of it called a farnesyl group. It needs this farnesyl molecule to anchor the protein tothe nuclear membrane. In normal cells, this farnesyl group is removed, butthis step does not take place in Progeria because of the mutation and theprogerin protein therefore remains stuck in the membrane, where it doesits damage. FTIs function by not allowing the farnesyl molecule to attachonto progerin in the first place. In the laboratory, treating Progeria cellswith FTIs restored their nuclei to a normal appearance (see figure 2).
> Training mouse models of Progeria: FTI, statins, and bisphosphonates
improve Progeria in mouse models of disease
Whenever possible, new medications are given to mice before they are considered for humans. These mice are observed for side effects and toxicityeffects, as well as for changes that may indicate the medicines would improve disease in people.
PRF-funded researchers at the University of California in Los Angeles developed two separate mouse models of Progeria that mimic many aspectsof the human disease. They treated these mice with FTIs at a young age
T h e P r o g e r i a R e s e a r c h F o u n d a t i o n ;
D R U G T R E A T M E N T T R I A L S 1 9 . 5
before the onset of symptoms. Both types of Progeria mice received FTIsin their water and were followed for several months. FTI treatment dramatically prevented the development of disease characteristics. FTI reduced bone fractures, delayed the onset of the disease, helped withweight gain, and increased life spans. There were minimal side effects atthe dose of drug that was given. It is not clear whether these two UCLAProgeria mice develop heart (vascular) disease. In a separate study, researchers at the National Institutes of Health created a mouse model ofProgeria that does develop cardiovascular disease. They began daily treatmentswith FTIs at a young age before the onset of symptoms, and found that theheart disease was improved in treated mice when compared to untreatedmice. Based on these studies, a first-ever clinical trial was undertaken inwhich a single FTI was given to children with Progeria.
Subsequently, researchers in Spain also treated a Progeria-like mousemodel with Pravastatin and Zoledronic Acid. The mice experienced longer,healthier lives with more body fat and improved hair and bones. This exper-iment provided the scientific evidence needed for the development ofclinical trials using these drugs in children with Progeria, either aloneor in combination with an FTI.
> Reliable measures of disease improvement are essential for the clinical trials
Although studies with cells and mice are extremely encouraging, as withany experimental treatment, we must have measures of disease improvementthat we can rely on to tell us whether the drugs are helping the children,within the two-year time frame of the trials. This means that careful off-drug measures need to be taken prior to the start of drug treatment, so thatwe will be able to measure changes while on this drug. To this end, carefulanalysis of baseline clinical status of children with Progeria is performed,using their medical charts, the weighing-in program, and data from pre-drugstudies performed at the trial site. The baseline measurements can thenbe compared to measurements taken periodically while on the treatmentdrug, so that we can determine as precisely as possible the exact impact ofthe treatment on the children.
1 9 . 6 T H E P R O G E R I A H A N D B O O K
Over the past 10 years, Progeria has gone from obscurity, to gene finding,to first-ever treatment trials. There are currently two clinical drug trialsongoing for Progeria. This section will provide information on clinical trialsin general, and where the Progeria clinical trials stand today. Websiteswhere you can find more detailed information are provided.
Thanks to the 2003 Progeria gene discovery, studies in the years that followed paved the way for The Progeria Research Foundation to fund and co-coordinate a first-ever clinical trial for children with Progeria at Children’s Hospital Boston, USA. Twenty-eight children from 15 differentcountries, speaking 9 different languages, flew to Boston every 4 months fora period of 2.5 years, from May 2007 through December 2009. The trial drugwas an FTI. FTIs have shown great promise in the laboratory and in animalmodels of Progeria. Results will be announced in 2010.
Since 2007, two additional treatment trials for Progeria have begun. A trialin France was initiated in 2008 and is treating children with the drugsPravastatin and Zoledronic Acid.
The third trial, which began in 2009 and is taking place at Children’s Hospital Boston, is treating children with all three drugs: FTI, Prava-statin, and Zoledronic Acid. Forty-five children from 24 different countries,speaking 17 different languages, fly to Boston every 6 months for testingand treatment, for a period of 2 years.
There is a vast amount of information about clinical trials available to you through the world wide web. Learning about clinical trials is very important, so that each family can decide whether to participate in anygiven study.
All clinical trials are considered research and are completely voluntary. The basic information for this section is derived from www.clinicaltrials.govand modified for the Progeria clinical trials.
Broadly defined, a clinical trial is a health-related research study in whicheither or both health observation or intervention may be applied. For Progeria, we have embarked on research studies with both goals in mind. We study as many things as possible before, during, and after children aretaking trial medications. Studying the “natural history” of Progeria helps
T h e P r o g e r i a R e s e a r c h F o u n d a t i o n ;
D R U G T R E A T M E N T T R I A L S 1 9 . 7
us to define what is happening to the children, and develop treatmentstrategies for them in our efforts towards improving quality and longevityof their lives.
> Why participate in a clinical trial?
Participants in clinical trials can play a more active role in their own healthcare, gain access to new research treatments before they are widely avail-able, and help others by contributing to medical research.
> Who can participate in a clinical trial?
All clinical trials have guidelines about who can participate. Using inclusion/exclusion criteria is an important principle of medical research that helpsto produce reliable results. The factors that allow someone to participatein a clinical trial are called “inclusion criteria” and those that disallowsomeone from participating are called “exclusion criteria”. For some of the Progeria trials, these criteria have included genetic confirmation ofProgeria, age, record of weight gain over time, liver and kidney health status, previous treatment history, and other medical conditions. Beforejoining a clinical trial, a participant must qualify for the study. Inclusionand exclusion criteria are never used to reject people personally. Instead,the criteria are used to identify appropriate participants and keep themsafe, since there is always a risk/benefit ratio to think about in research. The criteria help ensure that researchers will be able to answer the questionsthey plan to study.
> What happens during a clinical trial?
The clinical trial team includes many types of researchers, such as doctors,nurses, therapists, statisticians, coordinators, laboratory technicians, andother health care professionals. They check the health of the participantat the beginning of the trial, give specific instructions for participating inthe trial, monitor the participant carefully during the trial, and stay in touchafter the trial is completed.
For the Progeria trials, each patient family periodically flies to the trial sitefor testing and drug supply. There is also some monitoring at home, so thatany toxicities can be addressed immediately.
Informed consent is the process of learning the key facts about a clinicaltrial before deciding whether or not to participate. It is also a continuingprocess throughout the study to provide information for participants.
1 9 . 8 T H E P R O G E R I A H A N D B O O K
To help someone decide whether or not to participate, the investigators involved in the trial explain the details of the study. The information is provided in the primary language of each family to ensure clear communi-cation. Translation assistance is provided. Then the research team providesan informed consent document that includes details about the study, suchas its purpose, duration, required procedures, and key contacts. Risks andpotential benefits are explained in the informed consent document. Theparticipant, or parents or legal guardians, then decide whether or not tosign the document. Children able to understand the major issues are usuallyasked to sign a form after the trial is explained to them in age-appropriateterms. For a child under age 18, this is called assent. Informed consent isnot a contract, and the participant may withdraw from the trial at any time.
> What are the benefits and risks of participating in a clinical trial?
Benefits: Clinical trials that are well-designed and well-executed are thebest approach for eligible participants to:
•Play an active role in their own health care
•Gain access to new research treatments before
•Obtain expert medical care at leading health care facilities
•Help others by contributing to medical research
Risks: There are always risks to clinical trials:
•There are almost always side effects to experimental treatment.
These are carefully monitored, but since the treatment drug has
either never been given to children with Progeria, or the drug has notbeen given to many people in the world, we don’t know all of the sideeffects that may occur. Side effects, especially newly identified side effects, are reported to participant families during the trial, whereastrial results about benefits cannot be reported until the trial hasended.
•The experimental treatment may not be effective for the participant.
It is the clinical trial itself that asks whether the treatments are beneficial to children with Progeria. We do not know the answer until we finish the trial and analyze all of the data.
•The trial requires time and effort on the part of each family, including
trips to the study site, more treatments, hospital stays or complexdosage requirements. Each family is a partner in the trial process.
T h e P r o g e r i a R e s e a r c h F o u n d a t i o n ;
D R U G T R E A T M E N T T R I A L S 1 9 . 9
It takes tremendous courage to travel far from home, to meet with peoplewho often do not speak your language, and to entrust the care of your childto them.
> Does a participant continue to work with a home primary health care
Yes. The clinical trials provide short-term treatments related to a designatedillness or condition, but do not provide extended or complete primaryhealth care. Testing is focused on changes that may occur on drug. Homehealth care is focused on general health of the child. In addition, by havingthe health care provider work with the research team, the participant canensure that other medications or treatments will not conflict with the trialmedications.
> Can a participant leave a clinical trial after it has begun?
Yes. A participant can leave a clinical trial at any time. When decidingwhether to withdraw from the trial, the participant should discuss it withthe research team, to ensure that stopping the drugs is done safely. Thedrugs will usually need to be returned; the cost will be paid by the peoplerunning the trial, not the family.
> Where did the ideas for the trials come from?
Ideas for clinical trials came from researchers. (See The science behindthe Progeria clinical drug trials on page 19.1 of this section.) After researchers test new therapies in the laboratory and in animal studies(called preclinical studies), the experimental treatments with the mostpromising laboratory results move into clinical trials. It is important to remember that, although treatments can look great in the laboratory, wewill only know if and how well they work in patients by giving the treatmentsand then looking carefully at the results from the clinical trials.
Clinical trials can be sponsored or funded by a variety of organizations orindividuals. In the United States, Progeria treatment trials have beenfunded by The Progeria Research Foundation, by the National Institutes of Health (NIH), Children’s Hospital Boston, and Dana-Farber Cancer Institute. There is also a treatment trial ongoing in France for which European resources are used.
1 9 . 1 0 T H E P R O G E R I A H A N D B O O K
A protocol is a study plan on which all clinical trials are based. The plan is carefully designed to safeguard the health of the participants as well as answer specific research questions. A protocol describes what types of people may participate in the trial; the schedule of tests, procedures,medications, and dosages; and the length of the study. While in a clinicaltrial, participants following a protocol are seen regularly by the researchstaff to monitor their health and to determine the safety and effectivenessof their treatment.
> What types of clinical trials are the Progeria trials?
Phase I trials determine drug dosage and toxicity in a small number of people.
Phase II trials determine both drug toxicity and the effectiveness of drugson a disease in a small population.
Phase III trials determine the activity of a treatment by giving the realdrugs to half the patients and placebo (sugar pills) or other therapy to theother half. These trials usually include a large number of people (1,000-3,000) to confirm its effectiveness, monitor side effects, compare it to com-monly used treatments, and collect information that will allow theexperimental drug or treatment to be used safely. Phase IV trials are post-marketing studies that delineate additional infor-mation including the drug’s risks, benefits, and optimal use.
To date, all of the Progeria trials are Phase II trials, where both toxicity andeffect on disease progression are studied. They are also “open label” trials,in which all of the children receive the same drug treatment (none of theparticipants receive placebo).
T h e P r o g e r i a R e s e a r c h F o u n d a t i o n ;
Erprobung von Hilfsmitteln bei infantiler Cerebralparese mit der Bewegungs- und Ganganalyse Überblick Wegen meiner Tätigkeit am Spastiker-Zentrum München befasst sich mein beruflicher Alltag hauptsächlich mit der infantilen Zerebralparese und anderen neuroorthopädischen Erkrankungen. Zunächst werde ich einen aktuellen Überblick über die Zerebralparese und die Spastik geben und
Any alteration in adverse factors can take 10-12 weeks to show an normal fertilisation after intercourse, but cannot be guaranteed to do so. A poor swim up has less than 4 million/ml rapidly motile sperm and would be unlikely to achieve fertilisation after normal intercourse or standard in-vitro Parameters measured in sperm function tests fertilisation (IVF). Persistently poor sperm swim u

 1 9 . D R U G T R E A T M E N T T R I A L S
1 9 . D R U G T R E A T M E N T T R I A L S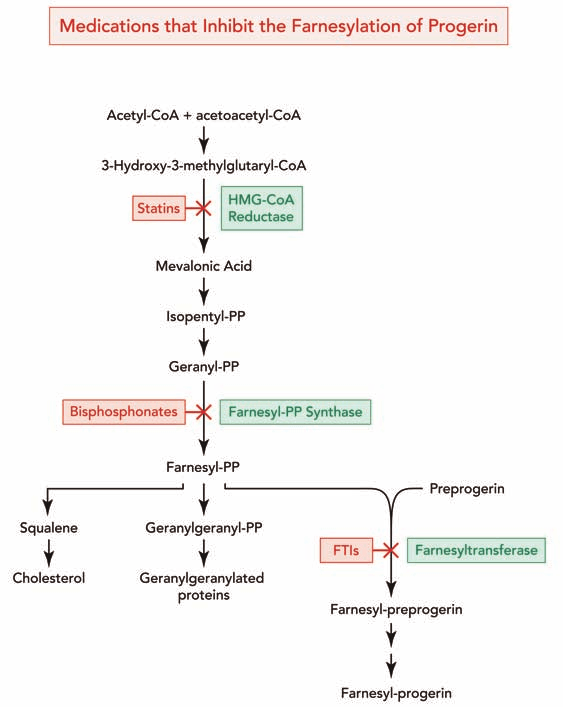 1 9 . 2 T H E P R O G E R I A H A N D B O O K
1 9 . 2 T H E P R O G E R I A H A N D B O O K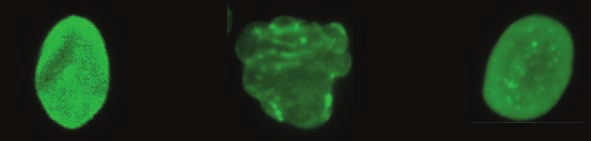 1 9 . 4 T H E P R O G E R I A H A N D B O O K
1 9 . 4 T H E P R O G E R I A H A N D B O O K