Urge incontinence Definition
Urge incontinence involves a strong, sudden need to urinate, followed by a bladder contraction, which results in leakage.
Alternative Names
Overactive bladder; Detrusor instability; Detrusor hyperreflexia; Irritable bladder; Spasmodic bladder; Unstable bladder; Incontinence - urge
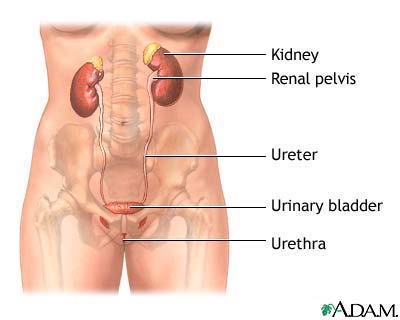
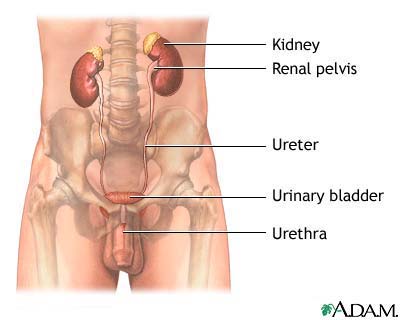
A person's ability to hold urine and maintain continence depends on normal function of the lower urinary tract, the kidneys, and the nervous system. The person must also have a physical and psychological ability to recognize and appropriately respond to the urge to urinate.
The bladder's ability to fill and store urine requires a functional sphincter muscle (which controls the flow of urine out of the body) and a stable bladder wall muscle (detrusor).
The process of urination involves two phases:
During the filling and storage phase, the bladder stretches so it can hold the increasing amount of urine. The bladder of an average person can hold 350 mL to 550 mL of urine. Generally, a person feels like they need to urinate when approximately 200 mL of urine fills up in the bladder. The nervous system tells you that you need to urinate, and also allows the bladder to continue to fill.
The emptying phase requires that the detrusor muscle contract, forcing urine out of the bladder. The sphincter muscle must relax at the same time, so that urine can flow out of the body.
The bladder of an infant automatically contracts when a certain volume of urine is collected in the bladder. As the child grows older and learns to control urination, part of the brain (cerebral cortex) helps prevent bladder muscle contraction. This allows urination to be delayed until the person is ready to use the bathroom.
Undesired bladder muscle contractions may occur from neurological problems and bladder irritation.
Urge incontinence is leakage of urine due to bladder muscles that contract inappropriately. Often these contractions occur regardless of the amount of urine that is in the bladder. Urge incontinence may result from neurological injuries (such as spinal cord injury or stroke), neurological diseases (such as multiple sclerosis), infection, bladder cancer, bladder stones, bladder inflammation, or bladder outlet obstruction.
In men, urge incontinence may be due to neurologic disease or bladder changes caused by benign prostatic hypertrophy (BPH) or bladder outlet obstruction from an enlarged prostate.
The majority of cases of urge incontinence are idiopathic, which means a specific cause cannot be identified.
Although urge incontinence may occur in anyone at any age, it is more common in women and the elderly.
Symptoms
z Sudden and urgent need to urinate (urinary urgency) z Frequent urination, in the daytime and at night z Abdominal distention or discomfort z Involuntary loss of urine
Exams and Tests
A physical examination will include examination of the abdomen and rectum. Women will also have a pelvic exam. Men will also have a genital exam. In most cases the physical exam reveals nothing abnormal.
If there are neurologic causes, other neurologic abnormalities may be found.
z Post-void residual (PVR) to measure amount of urine left after urination z Urinalysis or urine culture to rule out urinary tract infection z Urinary stress test (the patient stands with a full bladder and coughs) z Pad test (after placement of a pre-weighed sanitary pad, patient exercises, then pad is weighed to determine urine loss) z Pelvic or abdominal ultrasound z X-rays with contrast dye z Cystoscopy (inspection of the inside of the bladder) z Urodynamic studies (measurement of pressure and urine flow) z EMG (myogram) - rarely needed
Further tests will be performed to rule out other types of incontinence. These tests may include the "Q-tip test," which measures the change in the angle of the urethra at rest and when straining. An angle change of greater than 30 degrees often indicates significant weakness of the muscles that support the bladder, which is common in stress incontinence.
Treatment
There are several different approaches that may be used in managing and treating urge incontinence. If evidence of infection is found in urine culture, antibiotics will be prescribed. The choice of a specific treatment will depend on the severity of the symptoms and the extent that the symptoms interfere with lifestyle. There are three main approaches to treatment: medication, retraining, and surgery.
Medications used to treat urge incontinence are aimed at relaxing the involuntary contraction of the bladder and improving bladder function. There are several types of medications that may be used alone or in combination:
z Anticholinergic agents (oxybutynin, tolterodine, enablex, sanctura, vesicare, oxytrol) z Antispasmodic medications (flavoxate) z Tricyclic antidepressants (imipramine, doxepin)
Oxybutynin (Ditropan) and tolterodine (Detrol) are medications to relax the smooth muscle of the bladder. These are the most commonly used medications for urge incontinence and are available in a once-a-day formulation that makes dosing easy and effective.
The most common side effects of anticholinergic medicines are dry mouth and constipation. The medications cannot be used by patients with narrow angle glaucoma.
An antispasmodic drug is flavoxate (Urispas). However, studies have shown inconsistent benefit in controlling symptoms of urge incontinence.
Tricyclic antidepressants have also been used to treat urge incontinence because of their ability to inhibit or "paralyze" the bladder smooth muscle. Possible side effects include fatigue, dry mouth, dizziness, blurred vision, nausea, and insomnia.
The goal of any surgery to treat urge incontinence is aimed at increasing the storage ability of the bladder while decreasing the pressure within the bladder. Surgery is reserved for patients who are severely debilitated by their incontinence and who have an unstable bladder (severe inappropriate contraction) and poor ability to store urine.
Augmentation cystoplasty is the most frequently performed surgical procedure for severe urge incontinence. In this reconstructive surgery, a segment of the bowel is added to the bladder to increase bladder size and allow the bladder to store more urine.
Possible complications include those of any major abdominal surgery, including bowel obstruction, blood clots, infection, and pneumonia.
There is a risk of developing urinary fistulae (abnormal tubelike passages that result in abnormal urine drainage), urinary tract infection, and difficulty urinating. Augmentation cystoplasty is also linked to a slightly increased risk of developing tumors.
Some experts recommend a regimen of controlled fluid intake in addition to other therapies in the management of urge incontinence. The goal of this program is to distribute the intake of fluids throughout the course of the day, so the bladder does not need to handle a large volume of urine at one time.
Do not drink large quantities of fluids with meals -- limit your intake to less than 8 ounces at one time. Sip small amounts of fluids between meals. Stop drinking fluids approximately two hours before bedtime.
Additionally, it may be helpful to eliminate your intake of foods that may irritate the bladder, such as caffeine, spicy foods, carbonated drinks, and highly acidic foods such as citrus fruits and juices.
Management of urge incontinence usually begins with a program of bladder retraining. Occasionally, electrical stimulation and biofeedback therapy may be used in conjunction with bladder retraining.
A program of bladder retraining involves becoming aware of patterns of incontinence episodes and relearning skills necessary for storage and proper emptying of the bladder.
Bladder retraining consists of developing a schedule of times when you should try to urinate, while trying to consciously delay urination between these times. One method is to force yourself to wait 1 to 1 1/2 hours between urinations, despite any leakage or urge to urinate in between these times. As you become skilled at waiting, gradually increase the time intervals by 1/2 hour until you are urinating every 3 to 4 hours.
Pelvic muscle training exercises called Kegel exercises are primarily used to treat people with stress incontinence. However, these exercises may also be beneficial in relieving the symptoms of urge incontinence. The principle behind Kegel exercises is to strengthen the muscles of the pelvic floor, thereby improving the urethral sphincter function. The success of Kegel exercises depends on proper technique and adherence to a regular exercise program.
Another approach is to use vaginal cones to strengthen the muscles of pelvic floor. A vaginal cone is a weighted device that is inserted into the vagina. The woman contracts the pelvic floor muscles in an effort to hold the device the place. The contraction should be held for up to 15 minutes and should be performed twice daily. Within 4 to 6 weeks, about 70% of women trying this method had some improvement in their symptoms.
For people who are unsure if they are performing Kegel exercises correctly, biofeedback and electrical stimulation may be used to help identify the correct muscle group to work. Biofeedback is a method of positive reinforcement in which electrodes are placed on the abdomen and the anal area.
Some therapists place a sensor in the vagina (for women) or the anus (for men) to assess contraction of the pelvic floor muscles. A monitor will display a graph showing which muscles are contracting and which are at rest. The therapist can help identify the correct muscles for performing Kegel exercises.
About 75% of people who use biofeedback to enhance performance of Kegel exercises report symptom improvement, with 15% considered cured.
Electrical stimulation involves using low-voltage electric current to stimulate the correct group of muscles. The current may be delivered using an anal or vaginal probe. The electrical stimulation therapy may be performed in the clinic or at home. Treatment sessions usually last 20 minutes and may be performed every 1 to 4 days.
Another form of electrical stimulation called sacral neuromodulation involves the placement of a "bladder pacemaker," which stimulates the bladder nerves. This device may provide excellent relief of symptoms for those who do not respond to other therapies.
An experimental therapy involves injecting botulinum toxin (Botox) into the bladder muscle to help stop the involuntary contracts that lead to urge incontinence. Early study results suggest this is a promising treatment option for those who do not respond to other therapies.
People with urge incontinence may find it helpful to avoid activities that irritate the urethra and bladder, such as taking bubble baths or using caustic soaps
Urinary incontinence is a chronic (long-term) problem. Although you may be considered cured by various treatments, you should continue to see your provider to evaluate the progress of your symptoms and monitor for possible complications of treatment.
Outlook (Prognosis)
How well you do depends on your symptoms, an accurate diagnosis, and proper treatment. Many patients must try different therapies (some at the same time) to reduce symptoms.
Instant improvement is unusual. Perseverance and patience are usually required to see improvement. A small number of patients need surgery to control their symptoms.
Possible Complications
Physical complications are rare, but psychosocial problems may arise, particularly if incontinence results from an inability to get to the bathroom when urgency arises.
When to Contact a Medical Professional
Call your health care provider for an appointment if symptoms are causing you problems, if pelvic discomfort or burning with urination occurs, or if symptoms occur daily.
Prevention
Early initiation of bladder retraining techniques may be useful in reducing the severity of symptoms.
A.D.A.M., Inc. is accredited by URAC, also known as the American Accreditation HealthCare Commission (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics and subscribes to the principles of the Health on the Net Foundation (www.hon.ch).
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Call 911 for all medical emergencies. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. 1997- 2008 A.D.A.M., Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
Complementary and Alternative Medicine Online Continuing Education Series NCCAM CHAPTER I: OVERVIEW OF COMPLEMENTARY AND ALTERNATIVE MEDICINE Let’s drill down and talk a little more about some of the approaches, some of the potential hazards, and some of the opportunities. I’m going to go back to those CAM domains again; I mentioned 5 of them, and you have the wheel in the upper lef
UnitedHealthcare SignatureValueTM Offered by UnitedHealthcare of California 20/250a Performance HMO Schedule of Benefits (Benefit Package D, Network 1) These services are covered as indicated when authorized through your Primary Care Physician in your Participating Medical Group. (Only one hospital Copayment per admit is applicable. If a transfer to another facility is necessary, you are not re
 Urge incontinence
Urge incontinence 
 Urinary incontinence is a chronic (long-term) problem. Although you may be considered cured by various treatments, you should continue to see your provider to evaluate the progress of your symptoms and monitor for possible complications of treatment.
Outlook (Prognosis)
Urinary incontinence is a chronic (long-term) problem. Although you may be considered cured by various treatments, you should continue to see your provider to evaluate the progress of your symptoms and monitor for possible complications of treatment.
Outlook (Prognosis)