Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Peoplesgroup.in
Informative Article Lactic Acidosis In Critically Ill Patients Shafali Nandwani, *Mahip Saluja, **Mayank Vats ,**Yatin Mehta Department of Medicine, * Department of Pulmonary Medicine, Subharti Medical College, Meerut-250002, **Department of Pulmonary
and Critical Care, Indraprastha Apollo Hospital, New Delhi-110044
Abstract:
Lactic acidosis is defined as increase in blood lactate levels in association with acidemia. It should be suspected
in all patients presenting with shock & decreased mayocardial contractility. The patients with lactic acidosis have highmortality. However, the prognosis and case fatality are completely dependent on underlying disease in each patient withlactic acidosis being an independent indicator of severity of shock. All efforts should be directed towards treatment ofunderlying cause and concomitant correction of acidosis. Key Words: Lactate, Pyruvate, Lactic acidosis,THAM. History:
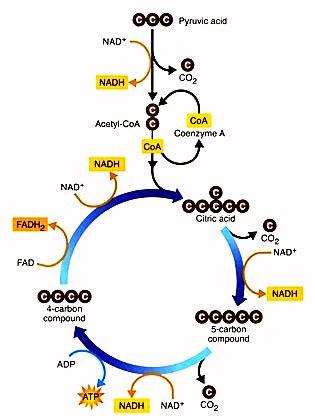
Adinine Dinucleotide Phosphate (NAD/NADH). (The
Lactic acidosis was first described in literature
normal ratio of lactic acid: pyruvic acid is 10:1).
in the year 1920. Clausen in the year 1925 identifiedaccumulation of lactic acid as a cause of metabolicacidosis. However, till the year 1960 it was notrecognized as significant clinical problem. In year 1976,Cohen & Woods classified lactic acidosis on the basisof presence or absence of adequate tissue oxygenation. Lactic acidosis is the most common under diagnosedlife threatening form of metabolic acidosis present in0.5% to 3.8% critically ill patients. Definition:
Lactic acidosis is a pathological state diagnosed
when the serum concentration of lactate or lactic acid is persistently 5mmol/L or greater and there is significant acidemia and serum pH< 7.35. (Normal lactate concentration is 2.0 mmol/L). Formation of Lactic acid:
There is constant production and metabolism
of lactate in the body. Red blood cells, brain and skinare major sources of lactic acid at rest while duringexercise skeletal muscles release significant amountof lactic acid.
Kidney and liver utilize lactic acid and convert
Fig.I: Kreb’s cycle showing formation of lactic acid.
it into carbon dioxide and water and use it forgluconeogenesis. Normally there is fine balance
between lactic acid production and utilization.
Lact ic acid a nd pyr uvic acid are inter
convertible and the reaction is catalyzed by the enzyme lactate dehydrogenase in the presence of Nicotinamide Adinine Dinucleotide / Nicotinamide
-----------------------------------------------------------------------------
Corresponding Author: Dr Mahip Salu ja, Associa te pr ofessor,
Department of Pulmonary Medicine, Subharti Medical College ,
Phone No.: 9837360657
Fig. II: Metabolic fate of lactic anion. E mail : drmahip@hotmail.com
People’s Journal of Scientific Research 43 Vol.3(1), Jan 2010
Lactic Acidosis In Critically Ill Patients ----------------------------------------- S Nandwani, M Saluja, M Vats & Y Mehta
Classification of Lactic Acidosis (Cohen &
of lactic acid or its diffusion in to total body fluid. This
is associated with fall in bicarbonate concentration,
They classified lactic acidosis into two types-
which rapidly returns to normal once GTCS subsides.
As the acidosis is abrupt and transient, secondary
TYPE A: It occurs in hypoperfusion and hypoxia.
response of hyperventilation may not develop and even
• Tissue hypoxia is seen in carbon monoxide poiso-
if magnitude of acidosis is high, bicarbonate therapy is
ning, severe asthma and severe anemia.
• Hypoperfusion occurs in state of shock (cardioge- (nic, hemorrhagic, septic, regional ischemia)
2. Tissue hypoxia: It is the predominant cause of TYPE B: It occurs when there is no clinical evidence
lactic acidosis in critically ill patients. Prolonged hypoxia
of hypoperfusion. It is further subdivided into 3
will lead to overproduction and underutilization of lactic
acid leading to lactic acidosis. Patients with hypotension
(i) B1is associated with acquired diseases like
either due to septic, hypovolumic or cardiogenic shock,
diabetes mellitus, grand mal seizures, hepatic failure,
may develop lactic acidosis due to poor perfusion of
septicemia, malignancies, pheochromocytoma, post
skeletal muscles and overproduction of lactic acid. The
cardiopulmonary bypass, renal failure, thiamine
degree of lactic acidosis correlates well with the
duration and severity of shock and is a prognostic factor
(ii)B2 is associated with metabolites, drugs and toxins
like acetaminophen, biguanides, cocaine, diethyl ether,epinephrine, norepinephrine, ethanol, ethylene glycol,
3. Cardio-respiratory arrest: It is another cause
isoniazid, lactulose, methanol, nalidixic acid, niacin,
leading to severe acidemia due to combined lactic
nitroprusside, antiretroviral therapy, paraldehyde,
acidosis and respiratory acidosis due to cardiac arrest
parenteral nutrition, terbutaline, theophyline etc.
and respiratory arrest respectively. Similarly patients
(iii)B3 is due to inborn errors of metabolism
with acute left ventricular failure with pulmonary edema
(congenital lactic acidosis) e.g. Glucose-6 phosphate
may develop acidosis due to reduced tissue perfusion
dehydrogenase deficiency, fructose1-6 diphosphatase
and respiratory acidosis due to respiratory failure.
deficiency, pyruvate carboxylase deficiency,organic
Reduced partial pressure of oxygen (PaO ) seldom
aciduria, Leigh’s disease, Alpers disease and
causes lactic acidosis if cardiovascular status is normal
because it is compensated by increased tissue perfusion. In patients of type II respiratory failure secondary to
Miscellaneous:
advanced chronic obstructive airway disease, seldom
Spontaneous lactic acidosis or idiopathic lactic
have lactic acidosis if there are no other confounding
acidosis like chronic recurrent lactic acidosis may be
factors. It is due to the fact that these patients have
due to subclinical, regional hypoperfusion or coexistence
chronic compensated respiratory acidosis and PaO ,
of various predisposing conditions or late manifested
enzymatic defect. D-lactic acidosis is rare and is caused by d-stereo
4. Carbon monoxide poisoning: It typica lly
isomer of lactic acid (d-lactic acid) which is synthesized
produces lactic in the form of acidosis due to lack of
by pathological gut flora. It can not be measured by
compensa tor y mecha nism of incr eased tissue
perfusion. Carbon monoxide binds to hemoglobin andas its affinity for hemoglobin is 40 times more than
Clinically important causes of lactic acidosis are
that of oxygen, it leads to tissue hypoxia and lactic
overproduction or underutilization of lactate or both the
conditions co-existing together. 1. Vigorous exercise: The magnitude of increase in 5. Drugs and toxins: Some of drugs & toxins also
lactic acid concentration depends upon the type and
lead to increased production of lactate. Alcohol
severity of exercise. Same is also true following
ingestion is a common cause of lactic acidosis as
prolonged generalized tonic clonic seizures (GTCS).
ethanol oxidation increases the conversion of pyruvate
Lactate level falls to normal immediately following
to lactate and decreases the clearance of lactate.
cessation of exercise or GTCS due to rapid metabolism
People’s Journal of Scientific Research 44 Vol.3(1), Jan 2010
Lactic Acidosis In Critically Ill Patients ----------------------------------------- S Nandwani, M Saluja, M Vats & Y Mehta
Alcohol induced lactic acidosis is treated by
Diagnosis:
correcting the hypoglycemia and electrolyte imbalance.
The major clues leading to the diagnosis of lactic
Alkali therapy is rarely required in such cases.
Prolonged metformin therapy is associated with lactic
• Increased anion gap (AG) metabolic acidosis
acidosis for many reasons. It increases glycolysis inperipheral tissues, decreases pyruvate oxidation and
Increased level of serum lactic acid (> 5 mmol/
Significant acidemia (arterial pH< 7 .35)
acidosis but it is not certain whether these drugs per
se or associated hypotension produces lactic acidosis. Fructose, frequently used in intravenous fluids and total
Laboratory studies include: Arterial blood gas analysis
parentral nutrition, leads to deficiency of thiamin andaccumulation of lactate. It also leads to inhibition of
(ABG), calculation of anion gap (normal range of anion
lactate utilization by liver and hence produces lactic
gap is 10-12mmol/L), serum lactate assay (for serum
acidosis. Sorbitol also gets converted into fructose and
lactate assay sample must be transferred in ice filled
leads to lactic acidosis by the same mechanism.
pack and analyzed within 4 hours- reference range for
Epinephrine enhances hepatic glycogenolysis
serum lactate is < 2mmol/L).
and glycolysis to lactate and reduces pyruvate utilization
Diagnosis of lactic acidosis may be missed in
resulting in lactic acidosis especially in massive doses.
patients with uremia and concomitant metabolic
Septic patients because of hypotension and poor
alkalosis if the clinical suspicion is not high.
peripheral perfusion are at risk of developing lactic
One should always obtain plasma lactate levels
in patients with acute respiratory failure when everbicarbonate concentration falls unexpectedly which
6. Terminal cirrhosis or hepato-cellular failure: It
may not be explained by respiratory failure alone.
may lead to lactic acidosis due to poor utilization of
concomitant metabolic alkalosis, the clue to thediagnosis is unexpected increase in anion gap. 7. Neoplastic diseases: Leukemia predisposes to lactic acidosis because of production of large amount Differential diagnosis includes the common causes
of lactate by tumor cells and it resolves gradually after
of increased anion gap acidosis like renal failure,
diabetic ketoacidosis and rhabdomyolysis. They may
8. Congenital deficiency of enzymes: Enzymes
occur alone or co-exist with lactic acidosis
which are involved in gluconeogenesis (glucose-6phosphate dehydrogenase, fructose 1, 6 pyruvate
Treatment: The most important therapy in
carboxylase), pyruvate oxidation (Pyruvate
management of lactic acidosis is correction of
dehydrogenase) and key enzymes of oxidative
underlying cause. In hypovolumic or cardiogenic shock,
phosphorylation may also lead to development of
rest oration of per fusion a nd adequate tissue
oxygenation will reverse lactic acidosis. In septic shock,antibiotic treatment, surgical drainage/debridement will
Clinical symptoms of lactic acidosis: Symptoms are
help in reversal of lactic acidosis. Giving intravenous
non specific and are those of underlying primary
thiamine in cases of total parentral nutrition will help in
disorder. Lactic acidosis should be suspected in all
resolution of lactic acidosis. In status asthmaticus, high
critically ill patients who are hypovolumic, hypoxic, in
dose of beta 2 agonist should be tapered gradually to
septic or cardiogenic shock or if unexplained high anion
reduce lactate levels. In shock, vaso constrictors
should be added only after volume replacement as theyworsen the acidosis.
Clinical signs consistent with tissue hypoperfusion(peripheral vasoconstriction), hypotension, oliguria/
Alkali Therapy though theoretically appealing, but
anuria and altered sensorium are usually present in
only few studies document safety and efficacy of
bicarbonate in lactic acidosis. Correction of acidosis
People’s Journal of Scientific Research 45 Vol.3(1), Jan 2010
Lactic Acidosis In Critically Ill Patients ----------------------------------------- S Nandwani, M Saluja, M Vats & Y Mehta
with bicarbonate may reverse depressed cardiac
over bicarbonate as it produces less carbon dioxide.
performance in critically ill patients. The side effects
Clinical trials do not prove THAM to be more effective
of bicarbonate therapy is acute hypercapnia which
than bicarbonate. The dose of THAM should be
increase intracellular acidosis and ionized hypocalcemia
calculated by the formula (0.3 mol/L)=0.3 body weight
which in turn decreases the myocardial contractility.
Bicarbonate is a hypertonic solution and causes volumeoverload and cardiac depression. It also increases the
Carbicarb is an equimolar combination of sodium
lactate production by increasing the activity of rate
carbonate and sodium bicarbonate that produces less
limiting enzyme phosphofructokinase. Adverse effects
carbon dioxide than sodium bicarbonate alone. It has
of bicarbonate can be reduced by giving slow infusions
theoretical advantage but trials have not demonstrated
in preference to rapid boluses, by increasing minute
any reduction in mortality or morbidity.
volume in patients on ventilator and by correctinghypocalcemia. Bicarbonate therapy is useful in patients
Prognosis: Depends on etiology of shock/underlying
of ischemic heart disease as acidosis increases the risk
disease which influences the survival but it has been
of major arrhythmias due to lowering of the myocardial
shown that serum lactate levels greater than 8 mmol/L
threshold. In these patients bicarbonate infusion to keep
are associated with mortality rate of more than 80%.
pH a bove 7. 10 can be justified. In all othercircumstances when lactic acidosis is accompanying
Conclusion: Lactic acidosis is an important and
pulmonary oedema, cardiopulmonary arrest, grand mal
frequently under diagnosed condition in critically ill
seizures, biguanide therapy, ethanol ingestion, and
patients. Timely correction of lactic acidosis can bring
diabetic ketoacidosis, bicarbonate therapy is not
marked change in outcome of patients in Intensive Care
Haemodialysis is rarely indicated as a treatment for Bibliography:
lactic acidosis. It may be used in drug toxicity to speedup elimination of drug/toxin. It is helpful when fluid
1. Adr ogue HJ, Madias NE: Man agemen t of life
overload and cardiac or renal insufficiency is present.
threatening acid base disorders. The New EnglandJournal of Medicine, 1998;338(1):26-34. Recent advances: Methylene blue, an oxidizing agent,
2. Agbenyega T, Angus BJ, Bedu-Addo G, Baffoe-Bonnie
has been used to restore cellular Nicotinamide Adinine
B, Guyton T, Stacpoole PW, Krishna S: Glucose andLactate kinetics in children with severe malaria. The
Dinucleotide (NAD+) with a very limited success. Journal of clinical Endocrinology and Metabolism,
Glucose, insulin infusion, nitropruside infusion,
hemodialysis, peritoneal dialysis have all been used in
3. Benjamin E: Continuous venovenous hemofiltration with
order to treat lactic acidosis but their efficacy is
dialysis and lactate clearance in critically ill patients.
unproven. Thiamine, lipoic acid and dichloroacetate
Critical Care Medicine, 1997;25(1):4-5.
have been used as they increase the activity of
4. Broder G, Weil MH, Excess lactate: An index of
pyruvate dehydrogenase enzyme, which converts
reversibility of shock in human patients. Science,
pyruvic acid to acetyl Co-A, but their clinical utility is
not certain. Riboflavin, Coenzyme-Q, L-carnitine have
5. Clausen SW: Anhydremic acidosis due to lactic acid. American Journal of Diseases in Children, 1925;29(6):761-766. Dichloroacetate (DCA) is an activator of pyruvate
6. Cohen RD, Woods HF: Clinical and biochemical aspects
dehydrogenase. It can lower concentration of lactic
of lactic acidosis. Blackwell Scientific Publication,
acid in patients by improving the lactate utilization but
7. Cohen RD, Woods HF: Lactic acidosis revisited,
when used in large clinical trial it did not show any
Diabetes, 1983;32(2):181-191.
effect on mortality. DCA, however, may be helpful in
8. Cuhaci B, Lee J, Ahmed Z: Sodium bicarbonate
lactic acidosis in children with severe malaria.
controversy in lactic acidosis. Chest, 2000;118(3):882-884. Tris hydroxymethyl aminomethane (THAM)
9. Cooper DJ, Walley KR, Wiggs BR, Russell JA:
It is a weak alkali and theoretical has the advantage
Bicarbonate does not improve harmodynamic is
People’s Journal of Scientific Research 46 Vol.3(1), Jan 2010
Lactic Acidosis In Critically Ill Patients ----------------------------------------- S Nandwani, M Saluja, M Vats & Y Mehta
clinically the patients who have lactic acidosis. Aprospective, controlled clinical Study. Annals of InternalMedicine, 1990; 112(7): 492-498.
10. Forsyth SM, Schmidt GA: Sodium bicarbonate for the
treatment of lactic acidosis. Chest, 2000; 117(1):260-267.
11. Foulks CJ, Wright LF: Successful repletion of bicarbonate
stores in ongoing lactic acidosis: a role for bicarbonate-buffered peritoneal dialysis. Southern Medical Journal,1981;74(9):1162-1163
12. Narins RG, Cohen JJ: Bicarbonate therapy for organic
acidosis: the case for its continued use. Annals ofInternal Medicine, 1987;106(4):615-618.
13. Peretz DI, Scott HM, Duff J, Dossetor JB, MacLean LD,
McGregor M: The significance of lacticacidemia in theshock syndrome. Annals of the New York Academy ofSciences, 1965; 119 (3 Chemistry): 1133-1141.
14. Stacpoole PW, Wright EC, Baumgartner TG, Bersin RM,
Buchalter S, Curry SH, Duncan C, Harman EM,Henderson GN, Jenkinson S: Natural history and courseof acquired lactic acidosis in adults. DCA-LacticAcidosis Study Group. The American Journal ofMedicine, 1994;97(1):47–54.
15. Stacpoole PW: Lactic acidosis. Endocrine andMetabolic Clinics of North America, 1993; 22(2): 221-245.
16. Stacpoole PW, Harman EM, Curry SA, Baumgartner TG,
Misbin RI: Tr eatmen t of lactic acidosis withdichloroacetate. New England Journal of Medicine,1983; 309(7): 390-396.
17. Totaro RJ, Raper RF: Epinephrine-induced lactic acidosis
following cardiopulmonary bypass. Critical CareMedicine, 1997; 25(10): 1693-1699.
People’s Journal of Scientific Research 47 Vol.3(1), Jan 2010
Biochemistry 1999, 38, 3067-3072 Stabilization of Tubulin by Deuterium Oxide†Gopal Chakrabarti,‡ Shane Kim,‡ Mohan L. Gupta, Jr.,‡ Janice S. Barton,§ and Richard H. Himes*,‡ Department of Molecular Biosciences, Uni V ersity of Kansas, Lawrence, Kansas 66045, and Department of Chemistry, Washburn Uni V ersity, Topeka, Kansas 66621 Recei V ed October 15, 1998; Re V ised Manus
Tipps und Tricks zur Gen-Spirale Allgemein Die Reagenzien sind reichlich bemessen. Während des Transports fliessen die Lösungen jedoch in die Deckel der Röhrchen. Deshalb vor Öffnen der Röhrchen alle Reagenzien kurz abzentrifugieren. (Bcn1 nur für 2 Sekunden!). So reichen die gelieferten Mengen gut für 6 oder mehr Gruppen. Damit die Pipettenspitzen auch auf die Socorex Mikro
 Informative Article
Informative Article