Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Otagodiabetesresearch.org.nz
E m e r g i n g T r e a t m e n t s a n d T e c h n o l o g i e s O R I G I N A L Effect of High-Dose Vitamin E on Insulin Resistance and Associated Parameters in Overweight Subjects ATRICK J. MANNING, MMEDSC, FRACP SYLVIA A. DE JONG
implicated in the pathogenesis of insulin
AYNE H.F. SUTHERLAND, PHD ANNE R. RYALLS
resistance is the free fatty acid (FFA) (7). OBERT J. WALKER, MD, FRCP LIZABETH A. BERRY
Although the rate of release of FFAs from
HEILA M. WILLIAMS, MSC
individual adipocytes may not be raisedin obesity, the increased amount of adi-pose tissue overall leads to an increase inthe flux of FFAs to the liver and skeletalmuscle, the two tissues most intimately
OBJECTIVE — Markers of oxidative stress and plasma alanine transferase (ALT) levels are
increased and circulating antioxidant concentrations are reduced in individuals with insulin
FFAs enter target tissues, they are either
resistance. Vitamin E improves glycemic control in people with diabetes. We tested the hypoth-esis that vitamin E would decrease markers of oxidative stress and plasma ALT levels and
stored as triglycerides or are utilized as a
improve insulin sensitivity in overweight individuals.
substrate for oxidation by the cell’s mito-chondria. As a result of the normal pro-
RESEARCH DESIGN AND METHODS — Eighty overweight individuals (BMI Ͼ27
cess of oxidation, reactive oxygen species
kg/m2) were randomly allocated to receive either 800 IU vitamin E per day or a matching placebo
for 3 months. The dose of vitamin E was increased to 1,200 IU per day for a further 3 months.
potentially harmful to cellular functions. To prevent these harmful effects, the cell
RESULTS — Plasma peroxides decreased by 27% at 3 months and by 29% at 6 months in the
group that received vitamin E and were positively correlated with plasma vitamin E concentra-
tions at the 6-month time point. At 3 months, fasting plasma glucose and insulin concentrations
idant concentrations are reduced in obese
were significantly reduced and homeostasis model assessment increased. These changes werenot apparent at 6 months. Plasma ALT concentrations declined significantly throughout the
between the production of ROS and anti-oxidant defenses results in oxidative
CONCLUSIONS — In conclusion, these findings indicate that vitamin E improves oxidative
stress (10). Although the relationship be-
stress and hepatocellular function. Although insulin resistance also improves, this effect appears
tween oxidative stress and certain diabe-
tes-related complications has been firmlyestablished (11), there is still uncertainty
Diabetes Care 27:2166 –2171, 2004
concerning its role in the development ofinsulin resistance. Theprevalenceofdiabetesisincreas- factorsisalteredintheobeseindividual inglucosehomeostasis,andhepaticinsu-
(3). Diabetes results when, in addition to
lin sensitivity is of profound importance
in determining fasting glucose concentra-
that of obesity, with insulin resistance ex-
occurs, leading to relative insulin defi-
plaining the link between these two enti-
␥-glutamyl transferase (GGT) predict fu-
responsible for insulin resistance remains
ture risk of developing diabetes (12).
unclear, it would appear that a number of
antioxidant activity. Systemic concentra-
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Department of Medical and Surgical Sciences, Dunedin School of Medicine, University of Otago,
individuals probably reflect nonalcoholic
Dunedin, New Zealand; and the 2Department of Preventive and Social Medicine, Dunedin School of Med-
fatty liver disease, which is itself a marker
icine, University of Otago, Dunedin, New Zealand.
of insulin resistance (13). Whether anti-
Address correspondence and reprint requests to Dr. Patrick J. Manning, Department of Medical and
Surgical Sciences, University of Otago, Private bag, Dunedin, New Zealand. E-mail: patrickmanning@
Received for publication 4 April 2004 and accepted in revised form 15 June 2004.
tions in obese individuals is uncertain. Abbreviations: ALT, alanine transferase; AST, aspartate aminotransferase; CRP, C-reactive protein; FFA,
free fatty acid; GGT, ␥-glutamyl transferase; HOMA, homeostasis model assessment; IL, interleukin; ROS,
to improve insulin signaling in vitro (14)
reactive oxygen species; TNF, tumor necrosis factor.
and improves glycemic control in individ-
A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
2004 by the American Diabetes Association.
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
Manning and Associates
correlation coefficients were used to test
insulin sensitivity and/or the other meta-
for relationships between variables.
resistance. This study was designed to in-
RESULTS — Six subjects dropped out
agnostic Laboratories, Dunedin Hospital.
from the study for personal reasons before
RESEARCH DESIGN AND METHODS — Eighty-six healthy sub-
characteristics of the remaining 80 partic-
jects, aged 31– 65 years, with a BMI Ͼ27
cant differences existed in any variables
(IL)-6 and tumor necrosis factor (TNF)-␣
centrations at baseline were Ͼ35 IU/l in
10, 7, and 14 subjects, respectively. Self-
supplements, serious illness, and clinical
that 55% of participants did not drink al-
ric, health, and lifestyle information was
collected. Participants gave informed and
method is based on the cleavage of perox-
the initial 3 months but gave blood at all
ides by horseradish peroxidase, leading to
randomization with stratification for sex
count indicated that 84% of subjects dur-
calibrator (Roche Diagnostics). As deter-
Ͻ25 kg/m2) is 27.2 (21.7–48.5) pmol/l. during the study.
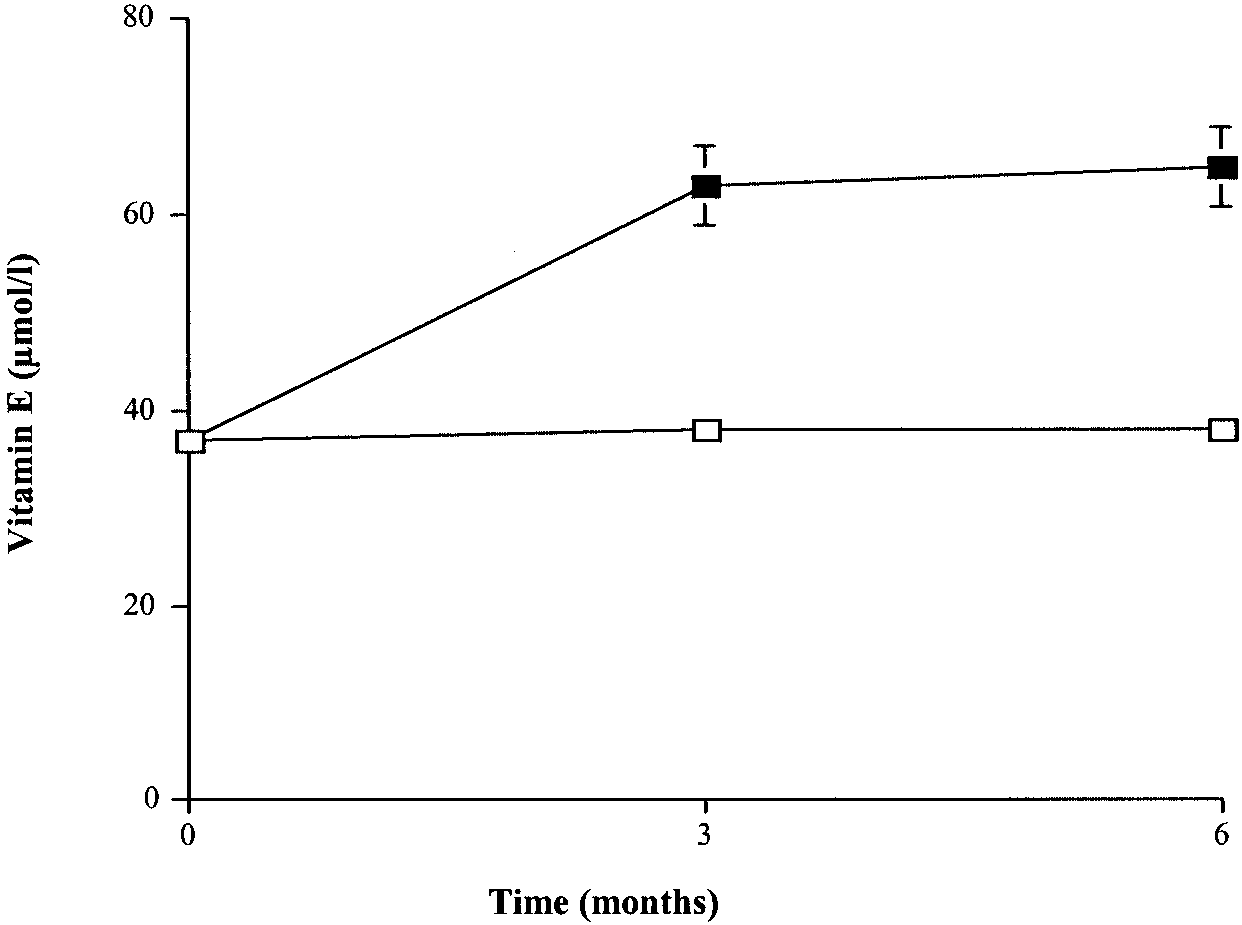
creased significantly in participants who
cebo for a further 3 months. Subjects were
␣-tocopherol concentration was mea- were randomized to vitamin E treatment
and did not change significantly in those
receiving placebo (Fig. 1). Despite an in-
the same assay to reduce interassay varia-
crease in vitamin E dosage in the final 3
months of the study, circulating vitamin E
plasma insulin, CRP, IL-6, TNF-␣, perox-
searcher (W.H.F.S.), who did not interact
index of insulin sensitivity was calculated
(fasting glucose ϫ fasting insulin).
tion was carried out in blocks of six. Par-
lifestyle changes during the study. Assess-
Values are given as median (interquartile
glucose, insulin, and peroxide concentra-
tions were significantly less than zero and
significantly greater than zero. Plasma tri-
that accounted for the underlying covari-
ance structure in the data and adjusted for
the baseline measures was used to analyze
variables were significantly different from
for all variables, the results being reported
tubes, the tubes were then centrifuged at
1,500g for 15 min at 4°C, and plasma and
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
Vitamin E and insulin resistance Table 1—Characteristics of the subjects at baseline
39). After lipid standardization, the re-sults remained unchanged, although thecorrelation between baseline vitamin E
statistically significant (r ϭ Ϫ0.120,
CONCLUSIONS — Oxidative stress
studies but not all (20), antioxidant ther-
type 2 diabetes (15,16). In addition, anti-
reduced in individuals at increased risk of
antioxidant therapy improves insulin sen-
sitivity in nondiabetic individuals who are
obese. Our results suggest that vitamin E
improves insulin sensitivity and the asso-
Data are median (interquartile range).
the magnitude of this improvement in in-sulin sensitivity, as indicated by fastinginsulin levels, depends on the magnitude
of the increase in plasma vitamin E. It is
was significantly correlated with the in-
well established that fasting insulin and
at 6 months (r ϭ Ϫ0.404, P ϭ 0.01, n ϭ
sulin sensitivity and correlate well with
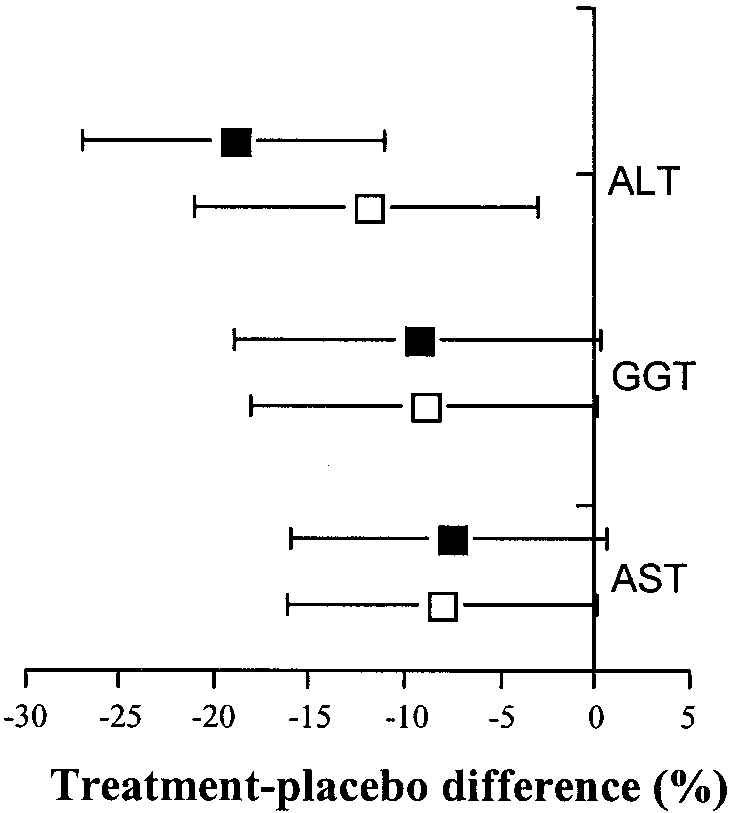
95% CIs, for plasma ALT, GGT, and ASTconcentrations at 3 months and 6 monthsare shown in Fig. 3. The differences forplasma ALT at 3 and 6 months were sig-nificantly different from zero. The corre-sponding differences for plasma GGT andAST were close to attaining statistical sig-nificance from zero.
body weight (P ϭ 0.77), BMI (P ϭ 0.87),blood pressure, and plasma concentra-tions of cholesterol, HDL cholesterol,HbA1c, CRP, IL-6, and TNF-␣ did notchange significantly in subjects receivingvitamin E compared with placebo duringthe study.
concentration was significantly correlatedwith the increase in plasma vitamin Econcentration during the initial 3 monthsof the study (r ϭ Ϫ0.235, n ϭ 80, P ϭ0.04). Plasma peroxide concentrationswere correlated significantly with plasmavitamin E concentration at baseline (r ϭ
Figure 1—Plasma concentration of vitamin E in participants receiving vitamin E (f) or placebo
Ϫ0.272, P ϭ 0.015, n ϭ 80). The de- (Ⅺ) during the study. Values are mean Ϯ SE.
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
Manning and Associates
dylinositol 3-kinase– catalyzed phos-phorylation of tyrosine residues in theseproteins, which is required for effectiveinsulin action. Recent evidence (28) sug-gests that vitamin E may influence the ac-tivity of these enzymes by decreasing thecurvature of plasma membranes.
glucose and insulin metabolism. It is themain site of insulin clearance from theblood (29). Animal studies (30) showthat genetic knockout of hepatic insulinreceptors results in severe insulin resis-
tance, hyperinsulinemia, glucose intoler-
ance, and severe hepatic dysfunction.
ated with hepatic insulin resistance (31)
HOMA at 3 (Ⅺ) and 6 (f)
and elevated levels of hepatic enzymes in
the blood. Furthermore, in nondiabeticindividuals, plasma ALT is associated
with percentage of body fat, hepatic insu-
lin resistance, and hepatic glucose output
in insulin sensitivity in elderly subjects
protection by regulating intracellular lev-
the cellular level that are not dependent
on its antioxidant activity and may poten-
output is the main determinant of fasting
tially contribute to improved insulin ac-
blood glucose levels. High-dose vitamin E
onstrating this effect in obese nondiabetic
els of plasma hepatic enzymes in patients
with nonalcoholic fatty liver disease (33).
ates diacylglycerol kinase activity, thereby
decreasing levels of diacylglycerol, which
cose levels by decreasing cellular oxidant
is an allosteric activator of protein kinase
stress, altering membrane properties, and
C (26). Increased protein kinase C activity
possible that the concomitant decrease in
fasting insulin and glucose levels may be
phosphorylating serine or threonine resi-
due to, at least in part, improved hepato-
insulin resistance and glucose output.
in the chemical-physical state of plasmamembranes as a result of a decrease inoxidative stress. Red cell membrane fluid-ity decreased in association with a de-crease in the ratio of serum oxidized toreduced glutathione and concomitantlywith an increase in insulin sensitivity dur-ing 4 months of vitamin E treatment inelderly subjects (22). In addition, in-creased vitamin E may enhance the en-dogenous cellular antioxidant defensesystem and reduce levels of ROS that areproduced by mitochondria. IncreasedFFA levels may overload the mitochon-drial oxidation process, leading to accel-erated production of ROS (7) andincreased oxidant stress in obese individ-
Figure 3—Treatment-placebo differ-
uals (10). Peroxides are ROS and interfere
ence and 95% CIs for plasma ALT, GGT,
with insulin signaling (24). In the present
and AST activities at 3 (Ⅺ) and 6 (f)
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
Vitamin E and insulin resistance
cient evidence to exclude a clinically im-
portant effect of vitamin E, and a larger
sulin resistance. Studies from our labora-
study is required to clarify this issue.
incidence of type 2 diabetes with lifestyle
described as being associated with insulin
intervention or metformin. N Engl J Med346:393– 403, 2002
5. Tuomilehto J, Lindstrom J, Eriksson JG,
associations have given rise to the meta-
jects in this study did not necessarily meet
the effects of vitamin E on its component
tion, during vitamin E supplementation.
tes mellitus by changes in lifestyle among
These findings suggest that changes in in-
an improvement in insulin sensitivity, we
subjects with impaired glucose tolerance. N Engl J Med 344:1343–1350, 2001
triglycerides at 3 months. This effect had
6. Buchanan TA, Xiang AH, Peters RK, Kjos
sitivity noted during vitamin E treatment.
sistent with the waning effect of vitamin E
ervation of pancreatic -cell function and
cological treatment of insulin resistance in
identified, these were not significant. No
high-risk Hispanic women. Diabetes 51:
this observation. Pill count did not sug-
7. McGarry JD: Banting Lecture 2001: dys-
regulation of fatty acid metabolism in the
intestinal absorption of vitamin E is al-
makes it unlikely that other factors had a
etiology of type 2 diabetes. Diabetes 51:7–
ready saturated at a dose of 800 IU/day. In
significant influence on this finding.
8. Boden G, Shulman GI: Free fatty acids in
obesity and type 2 diabetes: defining their
logical effects of vitamin E, indicated by
proves insulin sensitivity and several of its
role in the development of insulin resis-
associated parameters in overweight indi-
tance and beta-cell dysfunction. Eur J Clin
viduals, but the effect of treatment is not
Invest 32 (Suppl. 3):14 –23, 2002
ing this period. This finding suggests that
9. Evans JL, Goldfine ID, Maddux BA, Grod-
creased circulating levels of ALT, a risk
factor for the development of type 2 dia-
role in the improvement in insulin sensi-
resistance and -cell dysfunction? Diabe-
tivity with vitamin E treatment. We noted
results suggest that vitamin E could have a
a trend to an increase in circulating FFAs
role to play in delaying the onset of dia-
tentially adversely affect insulin action
(7). These observations, which are in con-
Examination Survey. Diabetes 52:2346 –
References
need further investigation. We cannot ex-
11. Brownlee M: Biochemistry and molecular
clude the possibility that in the present
cell biology of diabetic complications. Na-
study the increase in the dose of vitamin E
from 800 to 1,200 IU/day during the final
12. Vozarova B, Stefan N, Lindsay RS, Saremi
impaired glucose tolerance in U.S. adults:
deterioration in insulin sensitivity over
Examination Survey, 1988 –1994. Diabe-
ated with decreased hepatic insulin sensi-
hoc analysis to investigate the possibility
2. Edelstein SL, Knowler WC, Bain RP, An-
type 2 diabetes. Diabetes 51:1889 –1895,
detect a significant improvement in insu-
Haffner SM, Pettitt DJ, Sorkin JD, Muller
13. Angulo P: Nonalcoholic fatty liver dis-
lin sensitivity. Samples of the size used in
ease. N Engl J Med 346:1221–1231, 2002
this study, given the variability of the con-
of progression from impaired glucose tol-
trol group, have an 80% chance of detect-
spective studies. Diabetes 46:701–710,
tection against oxidative stress–induced
in glucose using the 5% level of signifi-
insulin resistance in rat L6 muscle cells by
cance. Although the estimates of the effect
3. Greenberg AS, McDaniel ML: Identifying
the links between obesity, insulin resis-
acid. Diabetes 50:404 – 410, 2001
of vitamin E were not statistically signifi-
tance and beta cell function: potential role
15. Paolisso G, D’Amore A, Galzerano D, Balbi
cant in the last period of the study, the CIs
V, Giugliano D, Varricchio M, D’Onofrio F:
show that effects of a magnitude similar to
pathogenesis of type 2 diabetes. Eur J Clin
those in the first follow-up period cannot
Invest 32 (Suppl. 3):24 –34, 2002
abolic control but not insulin secretion in
elderly type II diabetic patients. Diabetes
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
Manning and Associates
23. Paolisso G, Giugliano D: Oxidative stress
31. Garg A, Misra A: Hepatic steatosis, insulin
16. Jacob S, Ruus P, Hermann R, Tritschler
and insulin action: is there a relationship?
resistance, and adipose tissue disorders. J Clin Endocrinol Metab 87:3019 –3022,
24. Hansen LL, Ikeda Y, Olsen GS, Busch AK,
RAC-␣-lipoic acid modulates insulin sen-
Mosthaf L: Insulin signaling is inhibited
32. Griffith OW, Bridges RJ, Meister A: Evi-
sitivity in patients with type 2 diabetes
by micromolar concentrations of H2O2.
mellitus: a placebo-controlled pilot trial. J Biol Chem 274:25078 –25084, 1999
functions in vivo using intracellular glu-
Free Radic Biol Med 27:309 –314, 1999
25. Azzi A, Ricciarelli R, Zingg JM: Non-anti-
tathione: effects of amino acids and selec-
tive inhibition of enzymes. Proc Natl Acad
tocopherol (vitamin E). FEBS Lett 519:8 –
peroxides-iodide leads to a significant in-
26. Azzi A, Breyer I, Feher M, Pastori M, Ric-
ciarelli R, Spycher S, Staffieri M, Stocker
sera. Anal Biochem 316:147–153, 2003
tients with nonalcoholic steatohepatitis.
18. Sloan JC, Lappin TRJ: Automated colori-
responses to alpha-tocopherol. J NutrAm J Gastroenterol 98:2485–2490, 2003
34. Upritchard JE, Sutherland WH, Mann JI:
erol. Clin Chim Acta 119:197–207, 1982
27. Griffin ME, Marcucci MJ, Cline GW, Bell
fatty acid-induced insulin resistance is as-
activity in type 2 diabetes. Diabetes Care
index derived from oral glucose tolerance
sociated with activation of protein kinase
test. J Clin Endocrinol Metab 88:1019 –
C and alterations in the insulin signaling
35. Devaraj S, Jialal I: Alpha tocopherol sup-
cascade. Diabetes 48:1270 –1274, 1999
20. Skrha J, Sindelka G, Kvasnicka J, Hilger-
28. Bradford A, Atkinson J, Fuller N, Rand
tova J: Insulin action and fibrinolysis in-
RP: The effect of vitamin E on the struc-
ture of membrane lipid assemblies. J Lipid
betic patients. Free Radic Biol Med 29:
diabetes mellitus. Diabetes Res Clin Pract
36. Expert Panel on Detection, Evaluation,
21. Ferrannini E, Mari A: How to measure in-
Hepatic metabolism of insulin. Am J Med
sulin resistance. J Hypertens 16:895–906,
30. Michael MD, Kulkarni RN, Postic C, Pre-
22. Paolisso G, Di Maro G, Galzerano D, Cac-
D’Onofrio F: Pharmacological doses of vi-
hepatocytes leads to severe insulin resis-
tamin E and insulin action in elderly sub-
(Adult Treatment Panel III). JAMA 285:
jects. Am J Clin Nutr 59:1291–1296, 1994
DIABETES CARE, VOLUME 27, NUMBER 9, SEPTEMBER 2004
THE NUTRI-SPEC LETTER Volume 17 Number 12 From: Guy R. Schenker, D.C. December, 2006 Dear Doctor, BITS & PIECES, ODDS & BEGINNINGS. This has been an amazing year for NUTRI-SPEC doctors. --- It is truly gratifying to witness the quality and quantity of service you are providing. KEEP UP THE GOOD WORK … The world needs your systematic, objective approach
Mycologie médicale Place des champignons dans le monde du vivant :Grande diversité du règne fongique : Macromycètes : non concernés en pathologie humaine sauf les cas de mycoses invasives à coprinus (1 fois tous les 10 ans, chez les immunodéprimés)Micromycètes : moisissures (penicilliniums) ; aspergillus et dermatophytes éfinitions : Ce sont des microorganisme uni- ou plurice
 Vitamin E and insulin resistance
Vitamin E and insulin resistance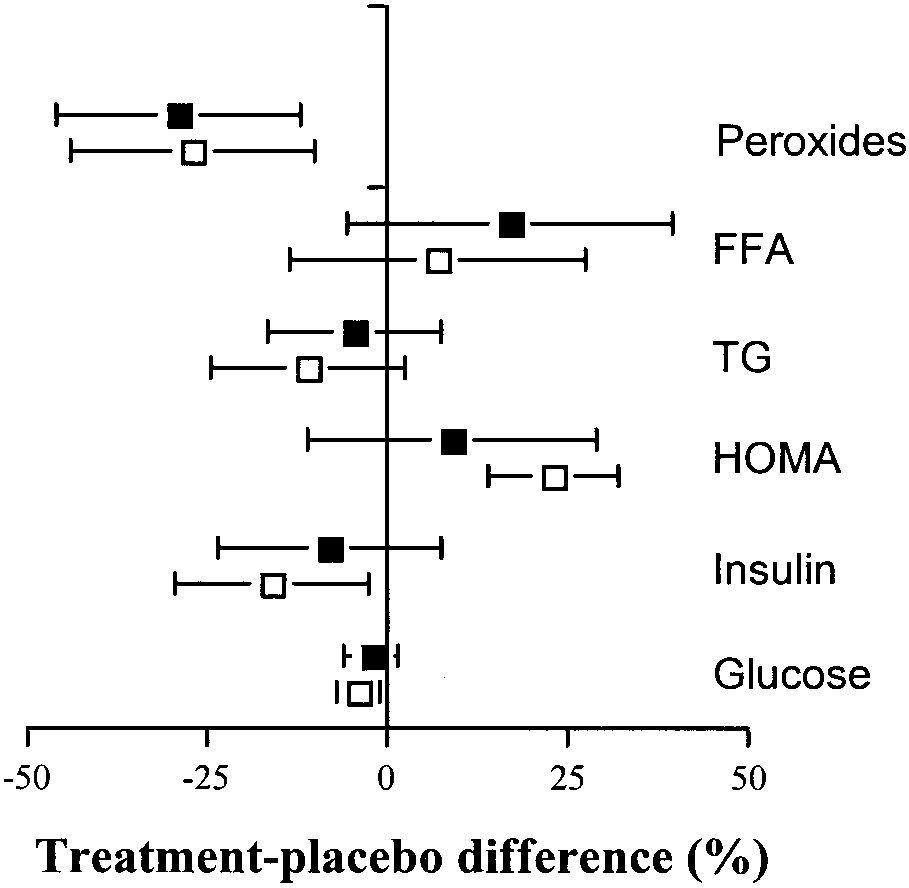
 Manning and Associates
Manning and Associates