Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Ro0410_01_titel
I case report _ calcified mandibular molar Author_ Dr Rafaël Michiels, Belgium _Treatment and discussion
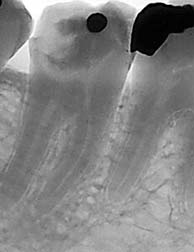
A diagnostic radiograph (Fig. 1), which is essential
in determining the treatment strategy, was taken to visualise the extent of the lesion and the anatomy ofthe roots. The patient was then anesthetised by a loweralveolar nerve block with 4% articaine, 0.01mg/ml epinephrine (Septanest Special, Septodont).
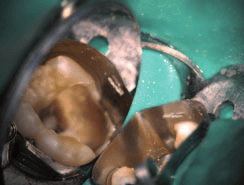
The temporary filling and cotton pellet were
removed, exposing a large carious lesion. In order tofacilitate the temporary restoration after treatment,an AutoMatrix (DENTSPLY Caulk) was placed. This also enabled better isolation. The tooth was then iso-lated with a rubber dam (Coltène/Whaledent; Fig. 2).
Isolation, which is one of the fundamental prin -
ciples in endodontics, is more than 100 years old. In
Fig. 1_Diagnostic radiograph.
_Endodontics has evolved enormously over the 1864 already, Sanford C. Barnum developed the rub- Fig. 2_Placement of rubber dam last few decades. However, the basic principles from
ber dam, which was generally accepted as a necessity
the past still apply today. The following case report in achieving good isolation and better prognosis.1
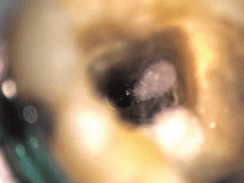
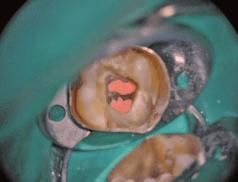
Fig. 3_Calcified tissue in gives an example of the manner in which the old prin-
ciples are applied with newer techniques, devices and
The first step in the treatment of a tooth […] is theadjustment of rubber dam over the diseased tooth topreclude the possibility of the entrance of germs in the_History and diagnosis oral secretions into the pulp chamber. This should bethe invariable rule.2
A 37-year-old female patient was referred to our
practice for a problem with her lower right second
However, a recent survey found that only 3.4% of
mandibular molar (tooth #31). She had no health is- general dental practitioners use the rubber dam insues, and was given an ASA score of 1. The referring their endodontic routine.3dentist opened the tooth because of an acute pulpitisdue to an extensive carious lesion disto-lingually. She
Visualisation and magnification can help clini-
had difficulty locating the mesial canals because the cians greatly in cases like the one presented here. pulp chamber was heavily calcified. She had placed Without the use of a surgical operating microscopecalcium hydroxide upon the orifices of the canals and (OM), it is very difficult to locate canals in the presencesealed the tooth with a cotton pellet and a temporary of a great deal of calcification. “You cannot treat whatrestoration. The patient had no clinical symptoms you cannot see” is a quote that is regularly heard andwhen she presented to our office for treatment.
that hits the nail right on the head. case report _ calcified mandibular molar I
In this case, visualisation and magnification were
obtained through the OM (OPMI pico, Carl Zeiss). Photographs were taken with a Canon PowerShotA650 IS (Canon) mounted on the FlexioStill adapter(Carl Zeiss).
I removed the carious dentine with LN burs
(DENTSPLY Maillefer). There was a great deal of cal -cified tissue in the pulp chamber (Fig. 3), which I alsoremoved with LN burs. The calcium hydroxide waseasily removed with 10% citric acid.
After a clean opening cavity had been created, the
actual root-canal treatment was begun. Two mesialcanals were located and coronally pre-flared withProTaper SX (DENTSPLY Mail efer; Fig. 4). Workinglength was determined with an ISO size 10 K-file(DENTSPLY Mail efer; Table I) and the Root ZX miniapex locator (J. Morita Europe). A glide path was thenestablished with K-Flexofiles sizes 15 and 20.
Cleaning was performed with 3% NaOCl, which
was ultrasonically activated with an Irrisafe tip (Sa -
Size in mm Working length Reference point
telec) several times throughout the procedure. The
ultrasonic activation of the irrigating solution resultsin more effective removal of organic tissue, debris and
planktonic bacteria.4 It is a very easy and inexpensive
procedure and should be incorporated in every endo -dontic routine.
canal, giving the canal sufficient taper but a small api- Fig. 4_Locating the mesial canals.
Shaping was done with ProTaper files S1, S2 and F1 cal diameter. Many controversies exist about shaping Table I_Working lengths and apical
in the mesial canals and ProTaper file F2 in the distal the apical diameter. I prefer an apical diameter of at diameters of the canals. Fig. 5_Fractured Irrisafe tip. Fig. 6_Removed Irrisafe tip. Fig. 7_Confirmation radiograph.
I case report _ calcified mandibular molar Fig. 8_Obturation of the isthmus.
least a size 30 because I rinse with a 30-gauge irri -
Obturation was performed with a hybrid technique
Fig. 9_Pulp chamber after obturation
gation needle. That way, the NaOCl comes into direct in which cold lateral condensation was used to fill the
contact with the apical dentine.5 This results in a sig- apical 4mm. Thereafter, the System B needle was
Fig. 10_Final radiograph.
nificantly better removal of debris from the apical taken 4mm short of working length into the canal. Fig. 11_Final position.
part of the root.6 In order to achieve a bigger apical Backfill was performed with the Elements Extruder indiameter, a ProFile size 30.06 (DENTSPLY Mail efer) smal increments of 2mm each time to reduce shrink-was taken to working length in the mesial canals and age. TopSeal (DENTSPLY Mail efer) was used as aa ProFile size 35.06 in the distal canal. Utilising an ISO sealer. During the backfill, I could see the isthmus size 10 K-file, patency was maintained in al three being obturated with gutta-percha (Fig. 8), which is acanals throughout the entire treatment.
desirable result. Were tissue to have been left in theisthmus, it may have led to failure. After obturation,
After the canals had been shaped, they were rinsed excess sealer in the pulp chamber was removed with
with 10% citric acid, which was ultrasonically acti- 96% alcohol (Fig. 9). A temporary restoration wasvated three times for 20 seconds with an Irrisafe tip. then placed with Fuji IX GP Fast A2 (GC Europe). During the third activation, the tip fractured and became stuck in the isthmus between the mesial
Final radiographs (Figs. 10 & 11) were taken and the
canals. Cotton pellets were placed in the mesio- patient was sent home with instructions regardinglingual and distal canal to prevent the instrument possible post-operative discomfort and a prescrip-from falling into the canals during its retrieval tion for 400 mg ibuprofen. (Fig. 5). Retrieval was done with another Irrisafe tip
(Fig. 6). A final rinse was performed with 3% NaOCl, _Conclusion
which was heated with a few bursts with System B
Dr Rafaël Michiels
(Sybron Endo). Finally, cone pumping was performed
In the past, there were several revolutions in the
with size 06 tapered gutta-percha cones. The lite - field of endodontics, such as isolating with the rubber
rature refers to cone pumping as manual dynamic dam, cleaning with NaOCl and shaping with rotary
irrigation that has proven to be more effective than instruments. Today, we stil make use of these prin -
ciples and are developing them further in order to
make treatment easier and safer and to gain more
A confirmation radiograph was then taken with favourable outcomes._
gutta-percha master cones (DENTSPLY Mail efer) in
place (Fig. 7). The canals were dried with paper points Editorial note: A list of references is available from the(Roeko).
Medical information asymmetry in cyberworld of Manuel Castel sPiotr Kasztelowicz Piotr.Kasztelowicz@am.torun.plTil 1997 Internet was strong associated with universities and education including medical research. Those timewas small number of virtual community members but all had equal access to whole information placed innet. In this time each networking participant was active not only to retri
By: Dr. Ayesha FakirTibb PractitionerMarch 2010Tuberculosis first became a major scourge in Europe during the Industrial Revolution, when overcrowding in cities was common, accounting for more than 30 percent of all deaths. With the development of the antibiotics streptomycin in the 1940ís, isoniazid in the 1950ís, ethambutol in the 1960ís and rifampicin in the 1970ís, the battle against tube

 I case report _ calcified mandibular molar
I case report _ calcified mandibular molar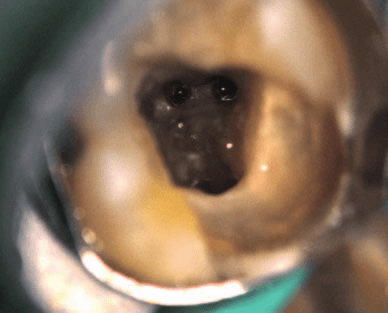
 case report _ calcified mandibular molar I
case report _ calcified mandibular molar I

 I case report _ calcified mandibular molar
I case report _ calcified mandibular molar