Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
438umb_laranne.qxd
Eur Arch Otorhinolaryngol (2002) 259 : 274–278
Jussi Laranne · Leo Keski-Nisula · Riitta Rautio · Markus Rautiainen · Mari Airaksinen
OK-432 (Picibanil) therapy for lymphangiomas in children
Received: 20 July 2001 / Accepted: 26 October 2001
Abstract Lymphangiomas are benign, soft tumors that
sent as soft, non-tender masses. Lymphangiomas may
most often affect the head and neck area, usually causing
cause marked disfigurement, recurrent infections, respira-
marked cosmetic and functional problems. Treatment op-
tory obstruction, malocclusion, dysphagia, dysphonia and
tions include surgery and a large number of different scle-
dysarthria as a result of the infiltration and compression of
rotherapy agents. Surgical treatment is challenging be-
neighboring structures. On the basis of their histological
cause of the need for complete excision. The risk of dam-
appearance, lymphangiomas are classified as capillary,
age to surrounding structures or poor cosmetic results is
cavernous or cystic and contain dilated lymphatic spaces
high. Various sclerotherapy agents have been shown to
in sizes ranging from small channels to large cysts. Often
have minimal effects on lymphangiomas. Their use has
the lesions are a combination of these subtypes and may
been associated with severe systemic, local and cosmetic
also contain hemangiomatous components [l]. Otolaryn-
side effects. OK-432 (Picibanil) is a new and promising
gologic manifestations are common since the head and
form of sclerotherapy. An intracystic injection of OK-432
neck region is the most often affected area [6]. Further-
produces a local inflammatory reaction, which leads to
more, lesions involving the lip, hypopharynx, larynx,
resolution of the lesion. We have treated 11 pediatric lym-
tongue and floor of the mouth have high rates of recurrent
phangioma patients with OK-432 with excellent results:
or persistent disease [11]. Spontaneous regression is un-
complete regression in six, marked regression in four and
no response in one case. Local swelling should be antici-
Complete and meticulous surgical excision is the text-
pated, especially when treating lesions near the upper air-
book recommendation for the primary approach to lym-
way. We found OK-432 injections to be safe and effective
phangiomas. However, complete excision is often impos-
as a first line of treatment for lymphangiomas.
sible due to the risk of damage to vitally or functionallyimportant surrounding structures. In addition, the cos-metic outcome after such radical surgery may be unac-
ceptable, especially in children, because it is an essen-tially benign lesion.
To avoid complications of surgical therapy, several
Lymphangiomas are relatively rare congenital malforma-
treatment options, including laser therapy [5], interferon-
tions of the lymphatic system. They make up approxi-
alpha [12] and various intralesional sclerosing agents, i.e.,
mately 6% of all benign lesions in children [11], occur
steroids, hypertonic saline, ethanol, and bleomycin, have
typically in patients younger than 2 years of age and pre-
been used to treat lymphangiomas, usually with little suc-cess. Intralesional injections of sclerosing agents are asso-ciated with a risk of extensive scar formation, resulting in
cosmetically unacceptable results and making eventual
Department of Otolaryngology, Head and Neck Surgery,
later surgical procedures more difficult. In addition, other
local and systemic side effects, such as pulmonary fibro-
P.O. Box 2000, 33521 Tampere, Finlande-mail: Jussi.Laranne@uta.fi
sis with bleomycin, make most sclerosants unsatisfactoryforms of treatment.
OK-432 (Picibanil, Chugai Pharmaceutical Co, Tokyo)
Department of Radiology, Tampere University Hospital, P.O. Box 2000, 33521 Tampere, Finland
is a lyophilized biological preparation containing the cellsof Streptococcus pyogenes (group A, type 3, strain Su)
treated with benzylpenicillin. It has been used in Japan
Department of Pharmacy, Tampere University Hospital, P.O. Box 2000, 33521 Tampere, Finland
primarily as immunotherapy for malignant tumors. The
Table 1 Results of OK-432 therapy
first report of its use for the treatment of lymphangiomas
microcystic component in four cases. There were seven boys and
was published in 1987 [9]. Since then, more reports with
four girls with a mean age of 5.5 years (9 months–13 years) at thetime of the first injection. Four patients had been operated on, and
good results and without any serious side effects have
one had received interpheron-alpha without success prior to the
been published [1, 3, 6, 8, 12, 13, 14]. We report our re-
sults using OK-432 in the treatment of lymphangiomas in
All treatments were performed under general anesthesia, and
the number of treatments per patient ranged from one to seven(Table 1). Lymphangiomas were punctured under ultrasound guid-ance, and a small amount of contrast was injected into the cysts todefine the position of the needle and dimensions of the lesion. In-
tracystic fluid was aspirated, and an equal volume of 0.01 mg/mlOK-432 solution was injected into the lesions. In one patient
Eleven children with lymphangioma were treated with OK-432 at
with a large cystic lesion in the hypopharynx (case 6), a pretreat-
Tampere University Hospital between 1998 and 2000. The diagno-
ment tracheotomy was performed as a safety measure. Following the
sis was made after clinical and radiological examinations. All lym-
treatment, the patients were monitored in the hospital for 24–
phangiomas were considered to be macrocystic, but with a mixed
Fig. 1 MRI-images of patient no. 3. *Lymphangioma in the right axilla: a before treatment, b complete regression after one OK-432 in- jection Fig. 2 MRI-images of patient no. 2. *Lymphangioma behind the right sternocleidomastoid muscle: a before treatment, b complete
lems it may cause. Especially in the head and neck region,
acute complications such as airway obstruction and prob-lems with swallowing and speech production may arise.
Complete regression was observed in six patients, marked
Lesions in this region also cause a notable cosmetic prob-
regression in four and no response in one patient (Table 1).
In patients with complete regression, no recurrence has
In a recent review of pediatric lymphangiomas, Orvi-
been observed during the follow-up period (Fig. 1, Fig. 2,
das and Kasperbauer [11] recommend that meticulous sur-
gical excision should be the primary approach to treat
All patients with complete regression had not been op-
these lesions. On the other hand, they report a quite re-
erated on or otherwise treated prior to sclerotherapy with
markable 20% incidence of permanent cranial nerve in-
jury in their own study involving 49 patients. Further-
Swelling, slight tenderness and fever continuing for
more, there was a positive correlation between the num-
2–4 days after the injection were noted in each case. In
ber of surgical procedures and the surgical complications.
case no. 6 (Fig. 4), marked soft tissue swelling developed
This underlines the importance of complete removal of
following the first treatment, and the decision to perform
the lesion during the primary operation.
a pretreatment tracheotomy served the patient well. Dur-
Particularly in the head and neck region, this is often
ing the following treatments, tracheotomy was not
extremely difficult, and the operation has to be staged,
needed. In other patients, serious side effects were not en-
leading to an increased risk of surgical complications.
countered, and the local inflammation did not cause scar
Thus, when dealing with complicated lymphangiomatous
formation or damage to the overlying skin.
lesions in the head and neck area, one might primarilyconsider non-surgical treatment options.
The spontaneous infection of lymphangioma can lead
to total regression of the lesion. This finding has led to the
Even though lymphangioma is a benign lesion, some kind
idea of using intracystic sclerosing agents. The mecha-
of treatment is necessary because of the potential prob-
nism behind a sclerosant involves the destruction of the
Fig. 3 CT-images of patient no. 6. *A large lymphangioma in the
neck compressing the larynx and hypopharynx: a before treatment, b marked regression after three OK-432 injections
epithelial lining of the cysts, with the following decrease
lesions respond better than cavernous or microcystic ones
in fluid production and collapse of the lesion. So far, the
because of greater communication between the intrale-
best results have been obtained with bleomycin. Orford et
sional spaces, which allows for better diffusion of the
al. [10] report good or excellent results in 88% of their
sclerosing agent throughout the lesion.
cases. However, with bleomycin there is a small risk of
Our results seem to be in line with the previously pub-
pulmonary fibrosis developing as a complication, and
lished studies. Complete regression was observed in six
therefore, its use has virtually been abandoned. The use of
patients, marked regression in four and no response in
alcohol (Ethibloc) has led to mediocre results with subse-
one. In our study, it appears that previous, unsuccessful
quent scar problems [4]. Recently, good results have been
surgical treatment hampers the sclerosing effect of OK-
obtained by intracystic injections of a fibrin sealant (Tis-
432. Only marked regression or no response was observed
sucol) in simple, monocystic lymphangiomas [2].
in this group. Postoperative intralesional scar formation
OK-432 is produced by incubating a culture of a low
obviously hinders the sclerosing agent’s diffusion through
virulence, SU strain of type III, group A Streptococcus
the lymphangioma, thus giving only partially satisfactory
pyogenes of human origin with penicillin G potassium
results. For this reason, we feel that OK-432 should be
followed by the lyophilization of the incubation mixture.
used as the primary form of treatment for lymphangio-
This results in the complete disappearance of the strep-
mas, and surgery should be considered only if sclerother-
tolysin S-producing ability [7]. In lymphangioma, an in-
tracystic injection of OK-432 produces an inflammatory
Here, we report the first serious side effect with OK-
reaction leading to the destruction of the epithelial lining
432. In case no. 6, soft tissue swelling after the first treat-
and the subsequent sclerosis and cicatricial contraction of
ment was quite marked and resulted in hypopharyngeal
the lesion. The only common side effects reported in pre-
edema with swallowing problems and a relative airway
vious studies have been fever and a local inflammatory re-
obstruction. This resolved in 5 days, and the tracheotomy
tube eventually was removed without further problems.
In seven different studies [1, 3, 6, 8, 12, 13, 14], a total
Since the local inflammatory reaction with swelling is a
of 64 children with lymphangiomas have been treated
normal response to the treatment, one should keep in
with OK-432, and the combined results show total shrink-
mind and be prepared for possible airway obstruction
age in 31, marked shrinkage in 10, slight shrinkage in 12
when treating paratracheal or hypopharyngeal lesions
and no response in 11 patients. It appears that macrocystic
Fig. 4 Patient no. 6: a follow- ing the first OK-432 injection a marked soft tissue swelling in the neck and laryngopharyn- geal region developed; b com- plete regression after four OK- 432 injections
Our results and those of the previously published stud-
6. Greinwald JH, Burke DK, Sato Y, Poust RI, Kimura K, Bau-
ies show that OK-432 is safe and effective in the treat-
man NM, Smith RJH (1999) Treatment of lymphangiomas inchildren: an update of Picibanil (OK-432) sclerotherapy. Oto-
ment of lymphangiomas. It can be considered as the first
line of treatment, especially in cases where surgical treat-
7. Ishida N, Hoshimoto T (1985) A streptococcal preparation as a
ment is associated with the possibility of serious func-
potent biological response modifier OK-432, 2nd edn. Amster-
8. Luzatto C, Midrio P, Tchaprassian Z, Guglielmi M (2000)
Sclerosing treatment of lymphangiomas with OK-432. ArchDis Child 82: 316–318
9. Ogita S, Tsuto T, Tokiwa K, Takahashi T (1987) Intracystic in-
jection of OK-432: a new sclerosing therapy for cystic hy-
1. Brewis C, Pracy JP, Albert DM (2000) Treatment of lymphan-
groma in children. Br J Surg 74: 690–691
giomas of the head and neck in children by intralesional injec-
10. Orford J, Barker A, Thonell S, King P, Murphy J (1995)
tion of OK-432 (Picibanil). Clin Otolaryngol 25: 130–134
Bleomycin therapy for cystic hygroma. J Ped Surg 30: 1282–
2. Castanon M, Margarit J, Carrasco R, Vancells M, Albert A,
Morales L (1999) Long-term follow-up of 19 cystic lymphan-
11. Orvidas U, Kasperbauer JL (2000) Pediatric lymphangiomas of
giomas treated with fibrin sealant. J Pediatr Surg 34: 1276–
the head and neck. Ann Otol Rhinol Laryngol 109: 411–421
12. Reinhardt MA, Nelson SC, Sencer SF, Bostrom BC, Ku-
3. Claesson G, Gordon L, Kuylenstierna R (1998) Japansk metod
racheck SC, Nesb ME (1997) Treatment of childhood lym-
revolutionerar behandlingen av lymphangiom. Läkartidningen
phangiomas with interferon-alpha. J Pediatr Hematol Oncol 19:
4. Dubois J (1997) Lymphangiomas in children: percutaneous
13. Schmidt B, Schimpl G, Höllwarth ME (1996) OK-432 therapy
sclerotherapy with an alcoholic solution of zein. Radiology
of lymphangiomas in children. Eur J Pediatr 155: 649–652
14. Smith RJH, Burke DK, Sato Y, Poust RI, Kimura K, Bauman
5. Eyrich GK, Bruder E, Hilfiker P, Quick HH, Patak MA, Grat
NM (1996) OK-432 therapy for lymphangiomas. Arch Oto-
KW, Sailer HF (2000) Temperature mapping of magnetic reso-
nance-guided laser interstitial thermal therapy (LITT) in lym-phangiomas of the head and neck. Lasers Surg Med 26: 467–476
Computer Science Department TECHNICAL REPORT Order of Magnitude Reasoning in Qualitative Differential Equations Ernest Davisf Technical Report #31 2 August 1987 o o Qj r-( l-i 0) H- fD Qj < l-h f" fD Ml cn l-( O (T> 3 ' O o i-h n ^ f-( en 3 O (tiQ M 3 D (D tfl n- iQ C C 0) (-â– (D H- rt n- r+ 1-3 wl I u>| O 3 cn < to O NEW YORK UNIVERSITY -eparfment of Computer Science Couran
YUKON QUEST® Official Race Rules for the 31st Annual Yukon Quest International Sled Dog Race As adopted by Yukon Quest International June 12, 2013 English is the official language of the Yukon Quest International Sled Dog Race All dollar amounts are in U.S. currency GENERAL RACE PROCEDURE 1. Race Start: The official starting date for the 2014 race will be Saturday, Febru
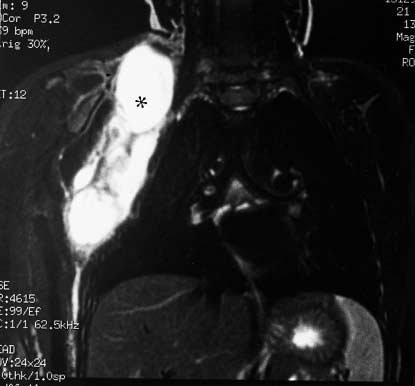
 Table 1 Results of OK-432 therapy
Table 1 Results of OK-432 therapy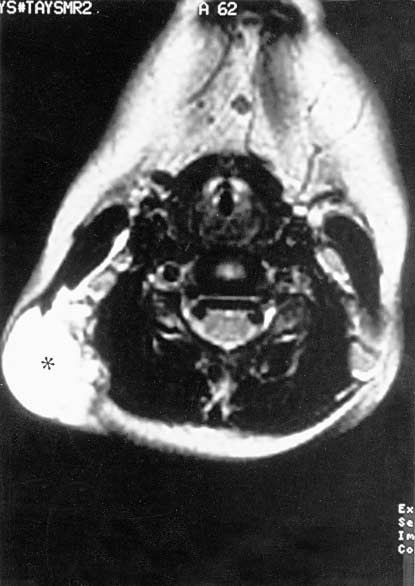
 Fig. 2 MRI-images of patient no. 2. *Lymphangioma behind the
Fig. 2 MRI-images of patient no. 2. *Lymphangioma behind the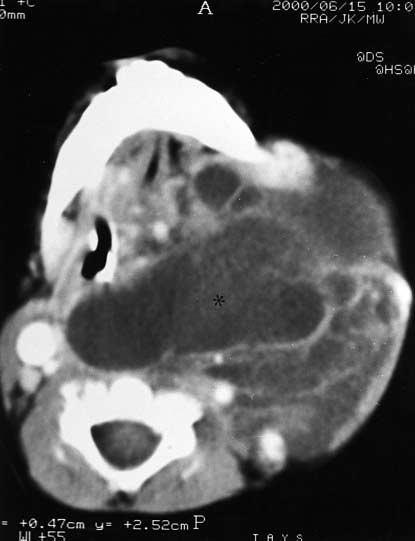
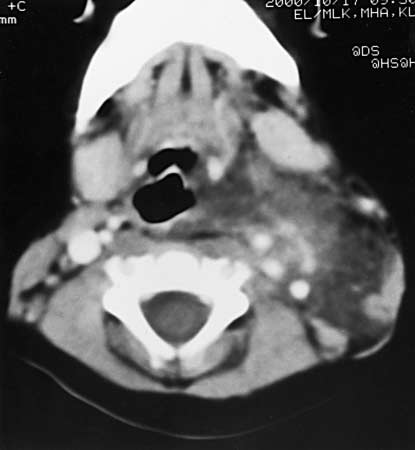 Fig. 3 CT-images of patient no. 6. *A large lymphangioma in the
Fig. 3 CT-images of patient no. 6. *A large lymphangioma in the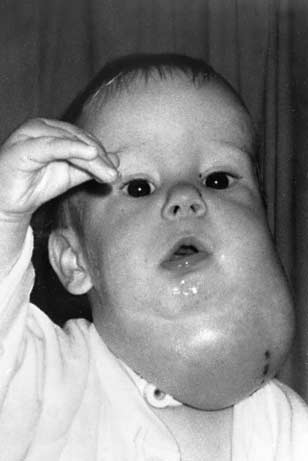
 Fig. 4 Patient no. 6: a follow-
Fig. 4 Patient no. 6: a follow-