Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Research.indd
Eili Klein,* David L. Smith,† and Ramanan Laxminarayan*
Hospital-acquired infections with Staphylococcus au-
increased, fi rst to other hospitals and then into the commu-
reus, especially methicillin-resistant S. aureus (MRSA) in-
nity (5). By the late 1960s, >80% of community- and hos-
fections, are a major cause of illness and death and impose
pital-acquired S. aureus isolates were resistant to penicillin
serious economic costs on patients and hospitals. However,
(4). Recent reports suggest that the evolution and spread of
the recent magnitude and trend of these infections have not
methicillin-resistant S. aureus (MRSA) seems to be follow-
been reported. We used national hospitalization and resis-
ing a similar wavelike emergence pattern (5).
tance data to estimate the annual number of hospitalizations
MRSA is now endemic, and even epidemic, in many
and deaths associated with S. aureus and MRSA from 1999
US hospitals, long-term care facilities (
through 2005. During this period, the estimated number
of S. aureus–related hospitalizations increased 62%, from
(7,8). Contrary to the generally accepted view, community-
294,570 to 477,927, and the estimated number of MRSA-
associated MRSA strains may be spreading into the health-
related hospitalizations more than doubled, from 127,036 care system rather than the other way around (9). Data from to 278,203. Our fi ndings suggest that S. aureus and MRSA
the National Nosocomial Infections Surveillance system
should be considered a national priority for disease control.
suggest that in intensive care units the proportion of S. au-reus isolates that are resistant to methicillin has increased to 59.5%–64.4% (
10,11). Recent reports also suggest that
taphylococcus aureus is a leading cause of hospital-ac-quired infections. It is the primary cause of lower re-
community-associated MRSA infections have become the
spiratory tract infections and surgical site infections (
dominant cause of community-associated S. aureus skin
and the second leading cause of nosocomial bacteremia (
and soft tissue infections (9,12). An understanding of the
pneumonia, and cardiovascular infections (
magnitude of the problem requires accurate national esti-
mates of incidence. However, national studies examining
S. aureus are especially diffi cult to treat because of
evolved resistance to antimicrobial drugs. Resistance to the effect of S. aureus or MRSA on the healthcare system penicillin and newer narrow-spectrum β-lactamase–resis-
are >5 years old (13,14). For 2000–2001, Noskin et al. es-
tant penicillin antimicrobial drugs (e.g., methicillin, oxacil-
timated that there were 290,000 S. aureus-related hospital-
lin) appeared soon after they were introduced into clinical izations (14). Kuehnert et al. estimated a similar number of practice in the 1940s and 1960s, respectively (
S. aureus–related hospitalizations for 1999–2000 and re-
resistance was initially confi ned to a small number of hos-
ported that 43.2% (125,969) were likely resistant to methi-
pitalized patients, but resistance spread as use of penicillin cillin (13).
In this study, we estimated the magnitude of the effect
*Resources for the Future, Washington DC, USA; and †National
and trend in the incidence and associated mortality rates
Institutes of Health, Bethesda, Maryland, USA
of infections related to S. aureus and MRSA over a 7-year
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
period, from 1999 through 2005, paying particular atten-
US Food and Drug Administration (15). Results are fi ltered
tion to the overall S. aureus infection level and the trend to remove repeat isolates and identify microbiologically of typical community-associated infections. Evidence on atypical results for confi rmation or verifi cation before be-the magnitude and trend of the problem on a national level ing included. informs rational, evidence-based decisions about how to
We included S. aureus isolates from inpatient areas
allocate resources and adjust healthcare policy to address that were tested for susceptibility to oxacillin (which is this issue. Infection trends are useful to clinicians, hospi-
used as a proxy for all β-lactam antimicrobial drugs, in-
tal administrators, insurers, and policymakers who make cluding methicillin) and classifi ed as susceptible, interme-decisions regarding control measures, especially infection-
diate, or resistant according to NCCLS breakpoint criteria.
control measures to contain the spread of nosocomial and Data included >65,000 isolates annually, of which <0.01% community-associated pathogens.
had intermediate resistance and so were classifi ed suscep-tible. To ensure comparability with NHDS data, isolates
were stratifi ed by the type of infection (i.e., isolates from
Our analysis focused on the period 1999–2005 and fol-
the lungs were classifi ed as pneumonias; those from the
lowed an approach similar to that described by Kuehnert blood, as septicemias or bacteremias) and geographic re-et al. (13). Estimated incidence of S. aureus was based on gion based on the US Census Bureau regions. hospitalizations with S. aureus–related discharge diagno-
The annual estimated number of S. aureus–related
ses from the National Hospital Discharge Survey (NHDS). hospitalizations was obtained from NHDS. The total The NHDS covers ≈270,000 patients and 500 short-stay number of MRSA-related hospitalizations was estimated hospitals by using a stratifi ed, multistage survey to create by multiplying the number of S. aureus–related infections a nationally representative annual sample of discharge re-
by the estimated percentage of S. aureus isolates that
cords. Children and general hospitals are included; federal, were resistant, stratifi ed by infection type and region. Fre-military, Veterans Affairs, or institutional hospitals are quencies of primary and secondary diagnoses were also not included. Each discharge record contains <7 different extracted for all hospitalizations that included S. aureus–International Classifi cation of Diseases, Ninth Revision related infections. (ICD-9), Clinical Modifi cation, discharge diagnosis codes
Relative standard errors for incidence of S. aureus
and is population weighted on the basis of the probabil-
were calculated by following guidelines for NHDS ac-
ity of sample selection and adjusted for nonresponse. All curacy described by Dennison and Pokras (16). Standard acute-care hospitalizations, excluding those of infants born errors and 95% confi dence intervals (CIs) were calculated in the hospital, were considered.
by multiplying the relative standard error by the estimated
S. aureus–related discharges were included if any of incidence. CIs for TSN data were calculated by using the
the 7 diagnosis codes contained specifi c S. aureus infection Wilson score method and incorporating continuity correc-codes: 038.11 (S. aureus septicemias), 482.41 (S. aureus tion as detailed by Newcombe (17). The variance of MRSA pneumonias), and 041.11 (other S. aureus infections). Re-
incidence was estimated by using the method described by
cords that contained multiple S. aureus–related discharge Barnett (18) and Goodman (19). codes were only counted once, with septicemia preferen-
NHDS reports whether or not hospitalization results
tially included, followed by S. aureus–related pneumonia.
in patient death but does not specify the cause of death.
Because there is no MRSA-specifi c ICD-9 code, we Because the primary diagnosis suggests that the disease
indirectly estimated the proportion of S. aureus–related played a role in patient death, we estimated the number of infections that were methicillin resistant by using antimi-
S. aureus–related deaths where the primary diagnosis code
crobial drug testing data from The Surveillance Network was an S. aureus–related code. We used the same proce-(TSN) Database-USA (Focus Diagnostics, Herndon, VA, dure as described above to determine the estimated number USA). TSN is an electronic repository of susceptibility test of deaths for which MRSA was involved. results collected from >300 microbiology laboratories in the United States; it has been used extensively to evalu-
ate antimicrobial drug resistance patterns and trends (15).
From 1999 through 2005, annual hospital discharges in
Participating laboratories are geographically dispersed and the United States increased ≈8%, from 32.1 million to 34.7 make up a nationally representative sample on the basis of million. During this period, the estimated number of hospi-hospital bed size and patient population. Patient isolates are talizations involving S. aureus–related infections increased tested for susceptibility to several different antimicrobial 62%, from 294,570 (95% CI 257,304–331,836) to 477,927 agents on site as part of routine diagnostic testing by using (95% CI 421,665–534,189). S. aureus–related hospitaliza-standards established by the National Committee for Clini-
tions with diagnosis codes for septicemia and pneumonia
cal Laboratory Standards (NCCLS) and approved by the increased 38% and 7%, respectively, and hospitalizations
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
involving other S. aureus–related infections in conditions classifi ed elsewhere nearly doubled. Overall, the rate of S. aureus–related diagnoses per 1,000 hospitalizations in-creased 50%, from 9.17 to 13.79 (Table 1).
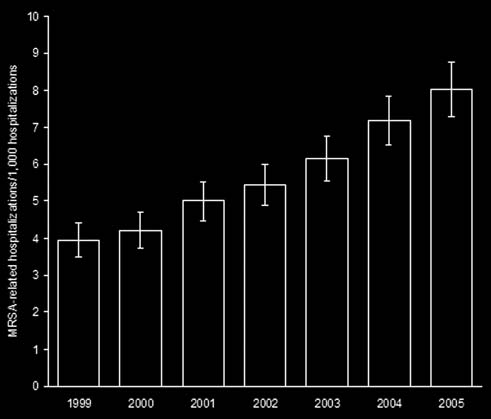
From 1999 through 2005, estimated MRSA-related
hospitalizations more than doubled, from 127,036 (95% CI 112,356–141,716) to 278,203 (95% CI 252,788–303,619). MRSA-related hospitalizations with a diagnosis code for septicemia increased 81.2%, from 31,044 (95% CI 25,170–36,918) to 56,248 (95% CI 46,830–65,665), and MRSA-re-lated hospitalizations with a diagnosis code for pneumonia increased 19.3%, from 30,632 (95% CI 24,597–36,666) to 36,540 (95% CI 29,527–43,554). The largest increase in MRSA-related hospitalizations involved infections outside the lungs or blood; these almost tripled from 65,361 (95% CI 55,801–74,920) to 185,415 (95% CI 162,102–208,728). Overall, the rate of MRSA-related discharges per 1,000 hospitalizations more than doubled, from 3.95 to 8.02 (Fig-
Figure 1. Estimated methicillin-resistant Staphylococcus aureus
(MRSA)–related hospitalization rates, United States, 1999–2005.
Rates are no. MRSA-related discharges/1,000 hospitalizations.
S. aureus–related septice-
Error bars represent 95% confi dence intervals.
mia and pneumonia were listed as any 1 of the 7 discharge diagnoses, these diagnoses were coded as the primary di-agnosis, on average, in 38% (standard deviation 6.4%) and Overall, the rate of S. aureus–related infections increased 54% (3.7%) of records, respectively, over the 7-year pe-
5% per year in the Northeast, 7% in the Midwest and South,
riod. The most frequent primary diagnosis associated with and 8% in the West. The rate of MRSA-related infections other S. aureus–related infections was other cellulitis and in the Northeast, Midwest, and South increased 9%, 11%, abscess (ICD-9 682), followed by postoperative infection and 12% per year, respectively. In contrast, the West had (ICD-9 998.59), infections from an implanted device or the lowest incidence and frequency of MRSA-related in-graft (ICD-9 996), osteomyelitis (ICD-9 730), and diabe-
fections, but the rate of MRSA-related infections increased
tes mellitus (ICD-9 250). Cellulitis infections increased 18% per year. Although increases were considerable, none >25% per year from 22,451 (95% CI 17,007–27,895) to of the rates in any region was signifi cantly different in any 87,500 (95% CI 75,485–99,515), which was nearly a 4-
year from the others at the 95% CI level.
fold increase. No other primary diagnosis infection code
In 2005, there were ≈11,406 S. aureus–related deaths
increased over this time period (Figure 2).
(95% CI 7,609–15,203), of which 6,639 were MRSA-relat-
Similar rates of discharge associated with S. aureus–
ed (95% CI 4,429–8,850). Since 1999, no trend was seen in
related and, more specifi cally, MRSA-related infections the number of deaths. We estimated that S. aureus–related per 1,000 hospitalizations were observed across all 4 US deaths averaged ≈10,800 per year (range 7,440–13,676) regions (Northeast, South, Midwest, and West; Table 2). and MRSA-related deaths averaged ≈5,500 per year
Table 1. Staphylococcus aureus and methicillin-resistant S. aureus (MRSA)–related hospital discharge diagnoses, by infection site and year, United States
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
respectively, during the study period. Resistance to genta-micin and trimethoprim-sulfamethoxazole decreased 76% and 64%, respectively. No instances of vancomycin-resis-tant (or intermediate-resistant) S. aureus in hospitalized pa-tients were reported. Discussion
MRSA, a common cause of nosocomial infections, has
emerged as an increasingly common cause of community-associated infections (20). Our analysis extends the work of Kuehnert et al. (13) and quantifi es recent trends and the ef-fect of S. aureus and MRSA on the US healthcare system.
This study focused on the effect and trends in the inci-
dence of S. aureus–related infections generally and MRSA-related infections specifi cally. Although the number of hospitalizations associated with an S. aureus infection in-creased 62% or ≈8.4% per year, the number of S. aureus
Figure 2. Primary diagnoses of Staphylococcus aureus–related
infections resistant to methicillin increased 119% or ≈14%
hospitalizations. The most frequent primary diagnosis associated
per year. In addition, although steady growth was observed
with other S. aureus–related infections was other cellulitis and
in the incidence of S. aureus– and MRSA-related septice-
abscess (International Classifi cation of Diseases [ICD]-9 682), followed by postoperative infection (ICD-9 998.59), infections from
mia, pneumonia, and device-associated infections that are
an implanted device or graft (ICD-9 996), osteomyelitis (ICD-9 730),
typically nosocomial, dramatic increases were observed in
and diabetes mellitus (ICD-9 250). Cellulitis and abscess infections
the incidence of skin and soft tissue infections that are typi-
increased at a rate >25% per year from 1999 through 2005. No
cally community associated. We also found no trend in the
other primary diagnosis infection showed a major increase over this
number of deaths caused by MRSA, and a decreasing trend
in the percentage of S. aureus– and MRSA-related hospi-talizations that resulted in death. These results suggest a
(range 3,809–7,372) (Figure 3). However, the percentage change in the ecology of the disease; community-associ-of S. aureus–related and MRSA-related hospitalizations ated MRSA is spreading more rapidly and possibly making that resulted in death did show a trend, a decrease from its way into hospitals.
≈3.7% in 1999 to only 2.4% in 2005. We also calculated
The indication that community-associated MRSA is
the number of deaths in which any diagnosis code was spreading rapidly into hospitals has implications for hos-S. aureus–related. These calculations showed that deaths pital and community infection control as well as empiri-with an S. aureus–related discharge code increased 18% cal treatment. In hospitals, handwashing practices, which from 24,715 (95% CI 17,853–31,577) to 29,164 (95% CI have been shown to be the leading intervention for limiting 21,620–36,708) from 1999 through 2005. Deaths in which the spread of nosocomial infections, should be improved MRSA was likely present increased >50%, from 11,240 to meet recommended guidelines (21). Because of the in-(95% CI 8,117–14,362) to 17,260 (95% CI 12,794–21,726) crease in skin and soft tissue infections, standard precau-over the same period. However, despite the increases, the tions, including use of gloves, are likely warranted when percentage of S. aureus–related hospitalizations that result-
dealing with all skin and soft tissue infections in outpatient
ed in death decreased from 8.4% in 1999 to 6.1% in 2005, clinics and acute-care facilities. Contact precautions, in-and the percentage of MRSA-related hospitalizations that cluding use of gowns and gloves, should be implemented resulted in death decreased from 8.8% to 6.2%.
for all wound care in acute-care facilities, and institution-
S. aureus resistance to ampicillin/sulbactam, cepha-
al programs to enhance antimicrobial drug stewardship
lothin, and erythromycin increased 21%, 35%, and 27%, should be implemented. Programs to increase community
Table 2. Hospitalizations and rates of infections with Staphylococcus aureus and methicillin-resistant S. aureus (MRSA) by region and year, United States*
*Rates are no. hospitalizations with S. aureus MRSA–related discharge diagnoses/1,000 discharges. Values in parentheses are rates for MRSA.
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
comial infections increase patient illness and the length of hospital stays. The direct cost has been estimated to be >$6 billion (infl ation adjusted) (29); costs of longer inpa-tient visits are shared by hospitals. The increasing trend in hospitalizations associated with S. aureus infections has considerable cost implications for the healthcare system, including costs when community-associated infections re-quire hospitalization and the additional expenses from as-sociated nosocomial infections.
Antimicrobial drug–resistant infections impose even
greater costs than susceptible infections. Several studies have estimated that antimicrobial drug–resistant infections increase death, illness, and direct costs by 30%–100% (30). Estimates of the excess cost of an infection with MRSA compared with an infection with methicillin-sensitive S. aureus range from ≈$3,000 to $35,000 (31–33). This sug-gests that MRSA cost the healthcare system (patients and hospitals) an extra $830 million–$9.7 billion in 2005, even
Figure 3. Estimated hospital deaths associated with Staphylococcus
without taking into account indirect costs related to patient
aureus and methicillin-resistant S. aureus (MRSA), United States,
pain, illness, and time spent in the hospital.
1999–2005. Error bars represent 95% confi dence intervals.
Another important implication of our analysis is that
the increasing incidence of MRSA in hospitalized patients, whether the infection was acquired in the hospital or the
awareness to control spread of infections and initiatives to community, is likely to increase the demand for vancomy-reduce inappropriate use of antimicrobial drugs should also cin. Despite several new (daptomycin, linezolid, tigecy-be implemented, especially in institutions that are focal in-
cline) and old (trimethoprim-sulfamethoxazole, clindamy-
stitutions such as daycare centers, schools, and prisons, as cin) antimicrobial drugs available for treatment of MRSA well as in high-risk groups such as immunodefi cient per-
infections, vancomycin has remained the fi rst-line drug for
sons, children, and elderly persons. Clinicians should be treating MRSA (12,34). This pattern has broad implications aware of the magnitude of the issue and consider MRSA a for the future control of MRSA as well as other pathogens. highly likely cause of skin and soft skin tissue infections, S. aureus infections resistant to vancomycin are already even in areas where the prevalence of MRSA is believed emerging (35), and vancomycin-resistant enterococci are to be low.
already a major problem in hospitals. Vancomycin use
Previous hospitalization has been associated with com-
should be restricted to methicillin-resistant S. aureus in-
munity MRSA carriage (22), and some recent studies have fections and used only for MRSA infections in situations suggested that MRSA infection rates in the community where other drugs are not appropriate. are positively correlated with S. aureus infection rates in
Our analysis has some limitations. First, it was restrict-
the hospital (23,24). Although a recent study suggests that ed to the incidence of disease associated with acute-care community-associated MRSA is causing hospital-acquired management within the hospital setting. Recent reports MRSA (25), it is unclear from our study whether commu-
suggest that MRSA has been increasing in outpatients
nity-associated MRSA is responsible for increasing rates (36,37). Thus, our results represent only a part of the prob-of nosocomial MRSA or the other way around. In all like-
lem, although hospitalizations outweigh outpatient visits
lihood, MRSA is spreading in hospitals and communities by ≈4 to 1. and complicating efforts to prevent infections in hospital-
Second, NHDS data enables the coding of only 7 diag-
ized patients. Regardless, our fi ndings demonstrate that re-
nosis codes; hospital information systems typically include
cent reports of localized increases in community-acquired 15–20 diagnosis codes for each admission (38). Thus, addi-MRSA (7,26–28) are part of a larger trend of MRSA be-
tional diagnoses in which S. aureus played a role may have
coming rapidly endemic in communities all over the United been excluded. Errors in ICD coding when transcribing states, emulating the wave-like pattern of emerging resis-
from doctors’ discharge summaries are another potential
tance to penicillin in the middle of the 20th century (5).
source of bias, as is the possibility that multiorgan failure,
Hospital-acquired infections from all causes are esti-
an end stage of sepsis, was coded as septicemia. One study
mated to cause >90,000 deaths per year in the United States concluded that the positive predictive value of the 038 code and are the sixth leading cause of death nationally. Noso-
on NHDS records to predict sepsis was 88.9%–97.7%, de-
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
pending on the criteria, and the negative predictive value research to quantify the relative importance and interaction was 80.0% (39). The authors of another study that exam-
between community- and healthcare-associated coloniza-
ined whether sepsis was coded correctly on hospital bills tion and infection, improved investments in hospital-in- concluded that strict reliance on administrative data may fection control, and greater public investment to support be prone to bias because only 75.4% of sepsis cases were research and development of an S. aureus vaccine. accurately coded (38). Thus, our results may be an under- estimate of the true effect, although trends are likely robust Acknowledgments to coding errors.
We thank Dan Sahm and Tracy Scheckel for providing drug
Third, TSN data provide information concerning only resistance data.
the site of isolate collection and not the infection. Thus,
E.K. and R.L. were supported by a Pioneer Portfolio grant
some isolates from blood or the lung area may not be as-
from the Robert Wood Johnson Foundation.
sociated with septicemia or pneumonia, respectively. In ad-dition, the code for S. aureus septicemia was given priority
Mr Klein is a senior research assistant at Resources for the
over the other more site-specifi c codes; this could have af-
Future. His research interests include the ecology and epidemiol-
fected the estimates of MRSA infections. However only a ogy of resistance to antimicrobial drugs and policies to prevent limited number of records had overlapping codes.
the emergence and spread of drug resistance.
Fourth, although the 2 data sources from TSN and
NHDS used in this article are nationally representative, they may not represent a stratifi ed random sample of hos-
References
pitals by type and region. However, the trends are likely 1. Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial in-robust enough to avoid bias. In addition, the percentage of
fections in medical intensive care units in the United States. Crit
S. aureus isolates resistant to methicillin reported in the
TSN database has increased similar to that reported by oth-
2. Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial in-
fections in pediatric intensive care units in the United States. Pediat-
er national studies (Figure 4). Finally, our estimates of the
number of hospitalizations and deaths are associated with, 3. Wisplinghoff H, Bischoff T, Tallent SM, Seifert H, Wenzel RP, but cannot be directly attributed to, S. aureus and MRSA
Edmond MB. Nosocomial bloodstream infections in US hospitals:
because NHDS does not report the immediate cause of
analysis of 24,179 cases from a prospective nationwide surveillance study. Clin Infect Dis. 2004;39:309–17.
death, and older, sicker patients are more likely to contract 4. Lowy FD. Antimicrobial resistance: the example of Staphylococcus a nosocomial infection (40). aureus. J Clin Invest. 2003;111:1265–73.
Our fi ndings suggest that S. aureus and MRSA should 5. Chambers HF. The changing epidemiology of Staphylococcus au-
become a national priority for disease control. Possible re-
reus. Emerg Infect Dis. 2001;7:178–82.
6. Strausbaugh LJ, Crossley KB, Nurse BA, Thrupp LD. Antimicrobial
sponses include expanding national surveillance or report-
resistance in long-term-care facilities. Infect Control Hosp Epide-
ing requirements for S. aureus and MRSA infections, more
7. Crum NF, Lee RU, Thornton SA, Stine OC, Wallace MR, Barrozo C,
et al. Fifteen-year study of the changing epidemiology of methicil-lin-resistant Staphylococcus aureus. Am J Med. 2006;119:943–51.
8. Lowy FD. Staphylococcus aureus infections. N Engl J Med.
9. Carleton HA, Diep BA, Charlebois ED, Sensabaugh GF, Perdreau-
Remington F. Community-adapted methicillin-resistant Staphylo-coccus aureus (MRSA): population dynamics of an expanding com-munity reservoir of MRSA. J Infect Dis. 2004;190:1730–8.
10. Centers for Disease Control and Prevention. National Nosocomial
Infections Surveillance (NNIS) system report, data summary from January 1992 through June 2004, issued October 2004. Am J Infect Control. 2004;32:470–85.
11. Klevens RM, Edwards JR, Tenover FC, McDonald LC, Horan T,
Gaynes R. Changes in the epidemiology of methicillin-resistant Staphylococcus aureus in intensive care units in US hospitals, 1992–2003. Clin Infect Dis. 2006;42:389–91.
12. King MD, Humphrey BJ, Wang YF, Kourbatova EV, Ray SM, Blum-
berg HM. Emergence of community-acquired methicillin-resistant
Figure 4. Percentage of Staphylococcus aureus isolates resistant
Staphylococcus aureus USA 300 clone as the predominant cause of
to methicillin in national surveys, United States, 1999–2004. TSN,
skin and soft-tissue infections. Ann Intern Med. 2006;144:309–17.
13. Kuehnert MJ, Hill HA, Kupronis BA, Tokars JI, Solomon SL, Jerni-
The Surveillance Network (data include hospital infections); NNIS,
gan DB. Methicillin-resistant Staphylococcus aureus hospitaliza-
National Nosocomial Infections Surveillance System (data include
tions, United States. Emerg Infect Dis. 2005;11:868–72.
only intensive care units); SENTRY, includes only skin and soft tissue infections.
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
14. Noskin GA, Rubin RJ, Schentag JJ, Kluytmans J, Hedblom EC, 28. Ossowski K, Chun RH, Suskind D, Baroody FM. Increased isola-
Smulders M, et al. The burden of Staphylococcus aureus infec-
tion of methicillin-resistant Staphylococcus aureus in pediatric head
tions on hospitals in the United States: an analysis of the 2000
and neck abscesses. Arch Otolaryngol Head Neck Surg. 2006;132:
and 2001 nationwide inpatient sample database. Arch Intern Med.
29. Martone WJ, Jarvis WR, Edwards JR, Culver D, Haley RW. Inci-
15. Sahm DF, Marsilio MK, Piazza G. Antimicrobial resistance in key
dence and nature of endemic and epidemic nosocomial infections.
bloodstream bacterial isolates: electronic surveillance with the sur-
In: Bennett JV, Brachman PS, editors. Hospital infections, 4th ed.
veillance network database—USA. Clin Infect Dis. 1999;29:259–
Philadelphia: Lippincott Williams and Wilkins; 1998. p. 461–76.
30. Cosgrove SE, Carmeli Y. The impact of antimicrobial resistance on
16. Dennison C, Pokras R. Design and operation of the National Hos-
health and economic outcomes. Clin Infect Dis. 2003;36:1433–7.
pital Discharge Survey: 1988 redesign. Vital Health Stat 1. 2000 31. Cosgrove SE, Qi Y, Kaye KS, Harbarth S, Karchmer AW, Carmeli Y. Dec;(39):1–42.
The impact of methicillin resistance in Staphylococcus aureus bac-
17. Newcombe RG. Two-sided confi dence intervals for the single pro-
teremia on patient outcomes: mortality, length of stay, and hospital
portion: comparison of seven methods. Stat Med. 1998;17:857–72.
charges. Infect Control Hosp Epidemiol. 2005;26:166–74.
18. Barnett HA. The variance of the product of two independent vari-
32. McHugh CG, Riley LW. Risk factors and costs associated with
ables and its application to an investigation based on sample data.
methicillin-resistant Staphylococcus aureus bloodstream infections.
Journal of the Institute of Actuaries. 1955;81:190.
Infect Control Hosp Epidemiol. 2004;25:425–30.
19. Goodman LA. On the exact variance of products. J Am Stat Assoc.
33. Rubin RJ, Harrington CA, Poon A, Dietrich K, Greene JA, Moidud-
din A. The economic impact of Staphylococcus aureus infection in
20. Moran GJ, Krishnadasan A, Gorwitz RJ, Fosheim GE, McDou-
New York City hospitals. Emerg Infect Dis. 1999;5:9–17.
gal LK, Carey RB, et al. Methicillin-resistant S. aureus infec-
34. Freidlin J, Acharya N, Lietman TM, Cevallos V, Whitcher JP, Mar-
tions among patients in the emergency department. N Engl J Med.
golis TP. Spectrum of eye disease caused by methicillin-resistant
Staphylococcus aureus. Am J Ophthalmol. 2007;144:313–5.
21. Boyce JM, Pittet D; Healthcare Infection Control Practices Advi-
35. Sieradzki K, Roberts RB, Haber SW, Tomasz A. The development of
sory Committee; HIPAC/SHEA/APIC/IDSA Hand Hygiene Task
vancomycin resistance in a patient with methicillin-resistant Staphy-
Force. Guideline for hand hygiene in health-care settings. Recom-
lococcus aureus infection. N Engl J Med. 1999;340:517–23.
mendations of the Healthcare Infection Control Practices Advisory
36. Johnson JK, Khoie T, Shurland S, Kreisel K, Stine OC, Rogh-
Committee and the HIPAC/SHEA/APIC/IDSA Hand Hygiene Task
mann MC. Skin and soft tissue infections caused by methicillin-
Force. Am J Infect Control. 2002;30:S1–46.
resistant Staphylococcus aureus USA300 clone. Emerg Infect Dis.
22. Warshawsky B, Hussain Z, Gregson DB, Alder R, Austin M, Bruck-
schwaiger D, et al. Hospital- and community-based surveillance 37. McCaig LF, McDonald LC, Mandal S, Jernigan DB. Staphylococcus of methicillin-resistant Staphylococcus aureus: previous hospi-
aureus–associated skin and soft tissue infections in ambulatory care.
talization is the major risk factor. Infect Control Hosp Epidemiol.
Emerg Infect Dis. 2006;12:1715–23.
38. Ollendorf DA, Fendrick AM, Massey K, Williams GR, Oster G.
23. Jones ME, Mayfi eld DC, Thornsberry C, Karlowsky JA, Sahm DF,
Is sepsis accurately coded on hospital bills? Value Health. 2002;5:
Peterson D. Prevalence of oxacillin resistance in Staphylococcus au-reus among inpatients and outpatients in the United States during
39. Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of
2000. Antimicrob Agents Chemother. 2002;46:3104–5.
sepsis in the United States from 1979 through 2000. N Engl J Med.
24. Salgado CD, Farr BM, Calfee DP. Community-acquired methicillin-
resistant Staphylococcus aureus: A meta-analysis of prevalence and
40. Lucet J-C, Chevret S, Durand-Zaleski I, Chastang C, Regnier B.
risk factors. Clin Infect Dis. 2003;36:131–9.
Prevalence and risk factors for carriage of methicillin-resistant
25. Maree CL, Daum R, Boyle-Vavra S, Matayoshi K, Miller L. Com-
Staphylococcus aureus at admission to the intensive care unit: re-
munity-associated methicillin-resistant Staphylococcus aureus iso-
sults of a multicenter study. Arch Intern Med. 2003;163:181–8.
lates causing healthcare-associated infections. Emerg Infect Dis. 2007;13:236–42.
Address for correspondence: Ramanan Laxminarayan, Resources for the
26. Fridkin SK, Hageman JC, Morrison M, Sanza LT, Como-Sabetti K,
Jernigan JA, et al. Methicillin-resistant
Future, 1616 P St NW, Washington, DC 20009, USA; email: ramanan@
ease in three communities. N Engl J Med. 2005;352:1436–44.
27. Herold BC, Immergluck LC, Maranan MC, Lauderdale DS, Gaskin
RE, Boyle-Vavra S, et al. Community-acquired methicillin-resistant
Use of trade names is for identifi cation only and does not imply
Staphylococcus aureus in children with no identifi ed predisposing
endorsement by the Public Health Service or by the U.S.
Department of Health and Human Services. Search past issues of EID at www.cdc.gov/eid
Emerging Infectious Diseases • www.cdc.gov/eid • Vol. 13, No. 12, December 2007
How to Use … Nicotine Patches • Remove patch from the sachet and then peel off the plastic backing. • Wave the patch in the air for 20 seconds to evaporate the alcohol off the patch. • Apply the patch to clean, dry, hairless skin, such as on the front or side of the chest, upper arm, sole of the foot, buttock or hip. • Do not use the same area on two consecutive days.
Health Education Kent, Surrey and Sussex Skills Development Strategy Primary and Community Care Workforce Development Programme Contents 1. Introduction and purpose 2. Key objectives of this programme 3. Education, training and workforce needs 4. Workforce profile 5. Education and Training needs identified to date in Kent Surrey and Sussex 6. Primary and Community Care Workforc
 involving other S. aureus–related infections in conditions classifi ed elsewhere nearly doubled. Overall, the rate of S. aureus–related diagnoses per 1,000 hospitalizations in-creased 50%, from 9.17 to 13.79 (Table 1).
involving other S. aureus–related infections in conditions classifi ed elsewhere nearly doubled. Overall, the rate of S. aureus–related diagnoses per 1,000 hospitalizations in-creased 50%, from 9.17 to 13.79 (Table 1).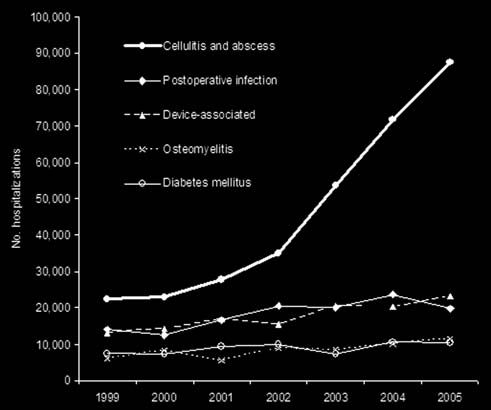 respectively, during the study period. Resistance to genta-micin and trimethoprim-sulfamethoxazole decreased 76% and 64%, respectively. No instances of vancomycin-resis-tant (or intermediate-resistant) S. aureus in hospitalized pa-tients were reported.
respectively, during the study period. Resistance to genta-micin and trimethoprim-sulfamethoxazole decreased 76% and 64%, respectively. No instances of vancomycin-resis-tant (or intermediate-resistant) S. aureus in hospitalized pa-tients were reported.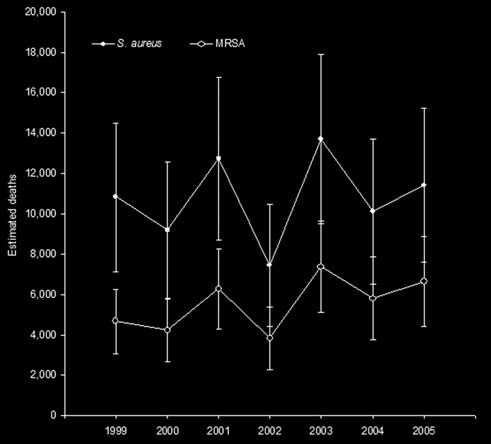 comial infections increase patient illness and the length of hospital stays. The direct cost has been estimated to be >$6 billion (infl ation adjusted) (29); costs of longer inpa-tient visits are shared by hospitals. The increasing trend in hospitalizations associated with S. aureus infections has considerable cost implications for the healthcare system, including costs when community-associated infections re-quire hospitalization and the additional expenses from as-sociated nosocomial infections.
comial infections increase patient illness and the length of hospital stays. The direct cost has been estimated to be >$6 billion (infl ation adjusted) (29); costs of longer inpa-tient visits are shared by hospitals. The increasing trend in hospitalizations associated with S. aureus infections has considerable cost implications for the healthcare system, including costs when community-associated infections re-quire hospitalization and the additional expenses from as-sociated nosocomial infections.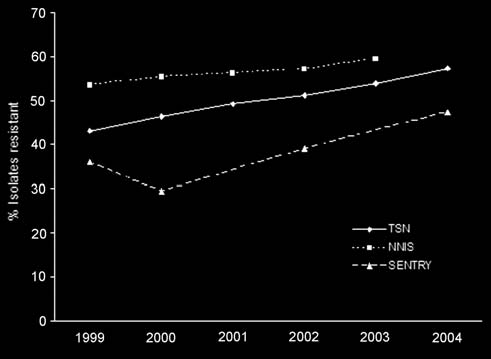 pending on the criteria, and the negative predictive value research to quantify the relative importance and interaction was 80.0% (39). The authors of another study that exam-
between community- and healthcare-associated coloniza-
ined whether sepsis was coded correctly on hospital bills tion and infection, improved investments in hospital-in-
pending on the criteria, and the negative predictive value research to quantify the relative importance and interaction was 80.0% (39). The authors of another study that exam-
between community- and healthcare-associated coloniza-
ined whether sepsis was coded correctly on hospital bills tion and infection, improved investments in hospital-in-