Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Lightburn.weisshospital.com
International Journal of Impotence Research (2008) 20, 479–486& 2008 Nature Publishing Group All rights reserved
ORIGINAL ARTICLERandomized, double-blind, placebo-controlled study ofpostoperative nightly sildenafil citrate for the prevention of erectiledysfunction after bilateral nerve-sparing radical prostatectomy
H Padma-Nathan1, AR McCullough2, LA Levine3, LI Lipshultz4, R Siegel5,9, F Montorsi6, F Giuliano7and G Brock8, on behalf of the Study Group10
1Department of Urology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA;
2Department of Urology, New York University School of Medicine, New York University Medical Center, New York, NY,USA; 3Department of Urology, Rush Medical College, Rush University, Chicago, IL, USA; 4Scott Department of Urology,Baylor College of Medicine, Houston, TX, USA; 5Sexual Health Team, Pfizer Inc, New York, NY, USA; 6Department ofUrology, University Vita Salute San Raffaele, Milan, Italy; 7Department of Physical Medicine and Rehabilitation, RaymondPoincare´ Hospital, Garches, France and 8Department of Urology, University of Western Ontario, London, ON, Canada
Four weeks after bilateral nerve-sparing radical retropubic prostatectomy, men with normalerectile function before surgery were randomized to double-blind sildenafil (50 or 100 mg) orplacebo nightly for 36 weeks, followed by an 8-week drug-free period before assessment of erectilefunction. Enrollment was prematurely ceased and only 76 men completed because, assuming aplacebo response rate similar to the published literature (for example, 34% in meta-analysis), the25% response at blinded interim review suggested a lack of treatment effect. On the contrary,spontaneous erectile function (a combined score of X8 for questions 3 and 4 of the InternationalIndex of Erectile Function and a positive response to ‘Were erections good enough for satisfactorysexual activity?’) occurred in only 4% of the placebo group (n ¼ 1 of 25) versus 27% (n ¼ 14 of 51,P ¼ 0.0156, Fisher’s exact test) of the sildenafil group. Nightly sildenafil administration for 36 weeksafter surgery markedly increased the return of normal spontaneous erections. International Journal of Impotence Research (2008) 20, 479–486; published online 24 July 2008
Keywords: prostatectomy; erectile dysfunction; sildenafil citrate
factors, such as the age of the patient, preoperativeerectile function and the experience of the surgeon.
Erectile dysfunction (ED) after bilateral nerve-spar-
Anatomically, the small size of the cavernous nerves
ing radical prostatectomy may be related to multiple
precludes clear visualization during surgery, makingthem susceptible to intraoperative trauma anddamage.Even spared nerves can experience neur-apraxia, a temporary failure in nerve conductionresulting from insult. Neurapraxia may explain
temporary (short-term) ED following nerve-sparing
University School of Medicine, New York University
prostatectomy. Sustained ED is more likely to
Medical Center, 540 1st Avenue, Sirball Building, Suite10U, New York, NY 10016, USA.
be caused by secondary cavernosal trabecular
smooth muscle apoptosis and its replacement with
9R Siegel was an employee of Pfizer at the time of this
Post-prostatectomy ED is severe and may include
10The other members of the Study Group are Professor
loss of nocturnal erections, and recovery is slower
Robert Andrianne, Belgium; David Bell, Canada; Gregory
than generally reported in the literature; many men
Broderick, USA; Serge Carrier, Canada; Professor Beatrice
will not regain erectile function for more than 12
Cuzin, France; Harry Jeoffrey Deeths, USA; Wayne
months.ED after prostatectomy is generally treated
Hellstrom, USA; Sender Herschorn, Canada; Ronald W
symptomatically, as needed when intercourse is
Lewis, USA; Raymond C Rosen, USA; Ridwan Shabsigh,
anticipatHowever, early regular use of intra-
USA; Phillip Stricker, Australia. Received 25 March 2007; revised 23 May 2008; accepted
cavernosal alprostadil injections, in an uncontrolled
23 May 2008; published online 24 July 2008
study, has been shown to improve the recovery rate
Sildenafil and ED after radical prostatectomy
of spontaneous erections after nerve-sparing radical
50- or 100-mg sildenafil, or matching placebo, was
retropubic prostatectomy.Despite this benefit,
taken once daily at nighttime. Erectile function was
pain, complications and inconvenience detract from
assessed, and plethysmography was conducted in
the willingness of patients to use intracavernosal
the subgroup, after 12, 24 and 36 weeks of treatment.
When double-blind treatment was discontinued,
Early, regular (every other night) use of sildenafil
patients remained untreated for 8 weeks (phase 3);
citrate (Viagra; Pfizer Inc, New York, NY, USA) after
no ED therapy, including sildenafil, was permitted.
nerve-sparing radical retropubic prostatectomy has
At the end of this period, erectile function, and
been shown, in an uncontrolled human study, to
nocturnal penile tumescence and rigidity in the
preserve or increase intracorporeal smooth muscle
content.Moreover, sildenafil taken at bedtime has
Computer-generated randomization was in a 1:1:1
been shown to significantly improve nocturnal
ratio using the method of random permuted blocks
erectile activity in men with vasculogenic or
and a pseudorandom number generator. Eligible
patients were allocated a randomization number
mediated by release of cavernous nerve nitric oxide
at the first visit of phase 2. Tablets containing
during rapid eye movement and phase 4 sleep.
50- or 100-mg sildenafil or matching placebo were
Indeed, since the inception of the current study, it
supplied to the investigators in blister cards in a
has become common clinical practice to provide
sildenafil postoperatively for variable periods of
Institutional Review Board/independent Ethics
time. For example, in a study of 167 men who were
Committee approval was obtained at all study sites,
potent before bilateral nerve-sparing radical retropubic
and signed informed consent was obtained from all
prostatectomy, approximately half used sildenafil on
an on-demand basis as needed for the symptomatictreatment of ED; recently reported 4-year follow-updata from this study have shown a continuing
improvement in erectile function with time.
Eligible men were 18–70 years of age, weighing
The current study provides, for the first time,
50–125 kg, and scheduled to undergo bilateral
objective data and a protocol for the use of sildenafil
nerve-sparing radical retropubic prostatectomy by
after nerve-sparing prostatectomy. The objective was
experienced surgeons. Patients had to have normal
to evaluate the efficacy of prophylactic, nightly use
preoperative erectile function, wish to return to
of sildenafil in preventing long-term ED. A second
sexual activity after surgery and be in a stable,
objective was to investigate the potential mechan-
heterosexual relationship for the past 6 months.
ism of action of sildenafil in preventing long-term
Normal preoperative erectile function was defined
ED by evaluating its effects on nocturnal penile
as a combined score of at least 8 on questions 3 and
4 of the International Index of Erectile Function (Q3:‘Over the past 4 weeks, when you attempted sexualintercourse, how often were you able to penetrateyour partner?’; Q4: ‘Over the past 4 weeks, during
sexual intercourse, how often were you able tomaintain your erection after you had penetrated
your partner?’). Individual scores for these questions
This study was designed to be a randomized,
were 0 (‘Did not attempt intercourse’), 1 (‘Almost
never/never’), 2 (‘A few times (much less than half
fixed-dose, multicenter study conducted in three
the time)’), 3 (‘Sometimes (about half the time)’), 4
phases between April 1999 and October 2001 at
(‘Most times (much more than half the time)’) and 5
outpatient urology clinics. A total of 16 sites in
North America, France, Belgium and Australia
For the subgroup undergoing plethysmography,
screened patients, and 11 sites in North America
an additional inclusion criterion was normal penile
and France enrolled and randomized patients.
tumescence and rigidity, defined as X55% base
During the 1- to 4-week preoperative assessment
rigidity for 10 consecutive minutes on at least 1 of 2
(phase 1), all patients underwent baseline evalua-
consecutive nights of monitoring before surgery.
tion of their erectile function using the International
Patients were excluded if they had pathological
Index of Erectile FuncA subgroup, consisting
stage greater than PT2, a tumor Gleason score equal to
of all men enrolled at two sites, also underwent
or greater than 8 on a preoperative biopsy, prostate-
evaluation of nocturnal penile tumescence and
specific antigen levels equal to or greater than
rigidity at home (2 consecutive nights) using penile
20 mg lÀ1, positive lymph nodes or required post-
plethysmography (RigiScan; Timm Medical Tech-
operative radiation or androgen ablation therapy.
nologies, Eden Prairie, MN, USA). At 4 weeks after
Patients were also excluded if they had a sleep
surgery, patients entered the 36-week double-blind,
disorder, were taking sedative/hypnotics as sleep aids
postoperative treatment (phase 2) during which
or were receiving nitrates or any treatment for ED. International Journal of Impotence Research
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
expected based on rates of spontaneous recovery of
The primary measure was the percentage of patients
erectile function reported in the published litera-
ture.After enrollment ceased, two US study
definition was established a priori as those patients
centers remained active to complete all the study
who, at the end of phase 3, had a combined score of
visits in the ongoing patients in the plethysmogra-
at least 8 for Q3 and Q4 of the International Index
phy subgroup and to provide information to aid in
of Erectile Function, and also answered ‘yes’ to
the question, ‘Over the past 4 weeks, have your
All statistical analyses were performed using
erections been good enough for satisfactory sexual
Statistical Analysis System software version 6.12
for efficacy analyses and version 8.2 for demo-
Secondary measures were changes from baseline
graphic and safety analyses. Primary and secondary
in the six-item Erectile Function domain of the
efficacy variables were analyzed in patients who
International Index of Erectile Function and, for
completed the 36-week double-blind treatment
the plethysmography subgroup, the duration of
period and the 8-week drug-free evaluation period.
penile tumescence and rigidity. The Erectile Function
In the original statistical analysis plan, the primary
domain has a score range of 1–30, with ED graded as
efficacy measure (percentage of responders) was
severe (1–10), moderate (11–16), mild to moderate
to be analyzed using the pair-wise Cochran–
(17–21), mild (22–25) and none (26–30).
Mantel–Haenszel (CMH) test. However, becausethe Mantel–Fleiss criterion was not satisfied, theCMH test was determined to be inappropriate foranalysis purposes. Therefore, Fisher’s exact test
(two-tailed) was used as an alternative (and appro-
On the basis of analyses of Q3 and Q4 of the
priate for the existing number of patients) approach,
International Index of Erectile Function in previous
with the Bonferroni adjustment to account for
studies, a conservative standard deviation of 2.00
multiple comparisons with placebo. Secondary
was assumed. If the mean sildenafil versus placebo
efficacy measures were analyzed using the nonpara-
difference for at least one of the sildenafil groups
metric Wilcoxon rank-sum test. Safety was assessed
was 1.5 points for both variables, then a sample size
in patients who took at least one dose of study
of 44 patients per treatment group would provide
90% power to detect a significant differencebetween variables singly and 80% power to detectsignificant differences for both variables jointly,based on two-sided analysis of variance tests
conducted at the 0.05 significance level withDunnett’s adjustment. Assuming that 80% of rando-
Of 238 patients screened, 125 were randomized to
mized patients would contribute to the intent-to-treat
treatment and 123 received at least one dose of study
analyses, a sample size of 55 patients per treatment
drug. In total, 94% (117 of 125) of the randomized
group was required. However, enrollment ceased
patients were enrolled at five North American sites.
after 125 because an interim blinded review of data
Patients were largely similar among treatment
from the 35 completed patients showed a response
rate of only 25% (9 of 35), which was not what was
Across the groups, a similar number of patients
Table 1 Demographics of the patients who took study medication and of the analyzed population
Took study medication (n ¼ 123)/analyzed (n ¼ 76)
aOne additional patient was randomized to this group, but discontinued before receiving study drug. International Journal of Impotence Research
Sildenafil and ED after radical prostatectomy
had concomitant hypertension (n ¼ 10–12), hyper-
Response rate after 36 weeks on study drug and 8
lipidemia (n ¼ 10–11) and ischemic heart disease
(n ¼ 1–2). All patients had good erectile functionat screening and developed ED as a result of
The 36-week double-blind treatment period was
completed by 82 men. The subsequent 8-week
drug-free evaluation period was completed by 76
men, who constituted the population analyzed for
efficacy: placebo, n ¼ 25; sildenafil 50 mg, n ¼ 23;
sildenafil 100 mg, n ¼ 28. Of these 76 men, 54 were
enrolled at the two US study centers, whichremained active to complete all the study visits in
aDefined as those who scored X8 on Q3 and Q4 of the
ongoing patients, and were included in the plethys-
International Index of Erectile Function and also answered ‘yes’
to the question ‘Over the past 4 weeks, have your erections been good
enrolled at three other North American study
enough for satisfactory sexual activity?’
centers. The eight men randomized at the other six
P ¼ 0.02 versus placebo (two-tailed Fisher’s exact test).
study centers were discontinued prematurely when
P ¼ 0.04 versus placebo (two-tailed Fisher’s exact test).
the centers were terminated after the interim review.
P ¼ 0.03 versus placebo (two-tailed Fisher’s exact test).
Reasons for the 47 premature discontinuations inthe placebo, sildenafil 50-mg, and sildenafil 100-mgtreatment groups, respectively, were lack of efficacy
treatment were 26.9±2.2 (27), including 26.3±1.9
(n ¼ 3, 2 and 1); adverse events (n ¼ 1, 5 and 1); loss
(27) in the 50-mg group and 27.3±2.5 (28) in the
to follow-up, withdrawn consent, noncompliance,
100-mg group; for the one patient who responded to
loss of stable sexual partner or protocol violation
(n ¼ 7, 2 and 6) and study closure (n ¼ 6, 8 and 5). Demographics were largely similar among treatmentgroups in the analyzed population, and between the
Secondary efficacy results: nocturnal penile rigidity
analyzed population and the larger population of
Of the 54 men who underwent RigiScan assessment,
35 were randomized to sildenafil treatment. Prior tosurgery, nocturnal penile rigidity at the base of thepenis was similar between sildenafil responders
Primary efficacy results: percentage of responders
(n ¼ 10) and nonresponders (n ¼ 25); (median: 59
At 48 weeks after undergoing prostatectomy (that is,
and 65 min, respectively). Median duration of
8 weeks after discontinuation of drug treatment), 15
nocturnal penile rigidity was markedly reduced to
of 76 patients were categorized as responders (20%),
less than 1 min in both sildenafil responders and
including 6 of 23 in the sildenafil 50 mg group
nonresponders, 4 weeks post-surgery. At 48 weeks
(26%), 8 of 28 in the sildenafil 100 mg group (29%)
after prostatectomy, and 8 weeks after discontinua-
and 1 of 25 in the placebo group (4%); overall, 14 of
tion of drug treatment, sildenafil responders had a
51 patients who completed sildenafil treatment
longer duration of base rigidity (median: 6 min) than
patients treated with sildenafil had a combinedscore of at least 4 for Q3 and Q4 of the InternationalIndex of Erectile Function, indicating that partial
Nightly use of sildenafil was well tolerated The most commonly reported adverse events weredyspepsia, headache, flushing, abnormal vision and
Secondary efficacy results: erectile function domain
rhinitis. Most adverse events were transient and
Erectile Function domain scores were reported as
mild in nature; two patients in the 50-mg sildenafil
mean±s.d. (median). Before surgery, scores were
group discontinued because of treatment-related
28.8±1.6 (30) in the sildenafil group and 28.6±2.2
adverse events. Although six serious adverse events
(30) in the placebo group, indicating no ED. End-
were reported, none of these were related to study
of-study scores were 13.1±9.5 (9) in the men who
had used sildenafil during the treatment phase,including 12.4±9.2 (9) in the 50-mg group and13.7±9.8 (10) in the 100-mg group, compared with
8.8±7.0 (6), in those who had used placebo duringthe treatment phase. More importantly, the end-
In a small but representative sample, we have demon-
of-study scores for the responders to sildenafil
strated that nightly administration of sildenafil
International Journal of Impotence Research
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
Erectile Function domain scores and by nocturnal
penile plethysmography. The similar response rate
between the 50- and 100-mg doses of sildenafil
suggests future study to identify the minimally
The study results reveal that the majority of men
who undergo bilateral nerve-sparing radical retro-
pubic prostatectomy have ED a year later. Because
we assumed a placebo response rate similar to that
of the published literature (see below), the low
overall response rate (25% (9 of 35)) at the blinded
interim review suggested a lack of treatment effect
and resulted in a decision to prematurely cease
enrollment. Most discontinuations were because of
study closure (n ¼ 19). Although prematurely ceas-ing enrollment and closing study sites precluded
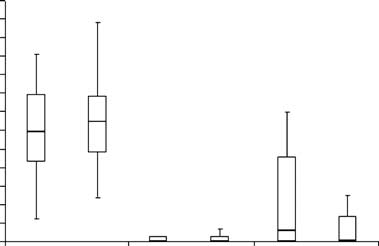
Figure 1 Nocturnal penile rigidity at the base of the penis asassessed using RigiScan, in responders (n ¼ 10) and nonrespon-
achieving the original sample size goal, the treat-
ders (n ¼ 25) to sildenafil treatment, before and 4 and 48 weeks
ment assignment followed the original randomiza-
after prostatectomy. Responders were a priori defined as those
tion ratio. Given the ultimate number of patients,
patients who, at the end of the 8-week drug-free period, had a
use of Fisher’s exact test (two-tailed), with the
combined score of at least 8 on Q3 and Q4 from the International
Bonferroni adjustment to account for multiple
Index of Erectile Function (scores for each question ranged from 0to 5) and answered ‘yes’ to the question ‘Over the past 4 weeks,
comparisons with placebo, was an appropriate
have your erections been good enough for satisfactory sexual
alternative statistical test to the originally planned
activity?’ Data are shown as median and 25th to 75th percentile
statistical analysis. However, the results should be
bars, with 10th and 90th percentile limits. Of the 54 men who
interpreted in the context of patients actually
underwent RigiScan assessment, 19 others were randomized toplacebo.
Nightly sildenafil was well tolerated: only two
patients, both in the sildenafil 50-mg group, dis-
continued the study because of adverse eventsrelated to sildenafil treatment. Six patients discon-
tinued prematurely because of lack of efficacy,
suggesting a misunderstanding of the study objec-tive: the prevention of long-term ED following
The 4% rate of return for spontaneous erectile
function in the placebo group (n ¼ 1 of 25) is
considerably lower than was expected based on
the published literature. There is a wide range of
rates reported in the literature, with the variation
Most commonly occurring AEs (X2% of patients)
being attributed to patient age, preoperative sexual
function, time since surgery, nerve-sparing procedure,
example, in two large series of preoperatively potent
men who underwent nerve-sparing prostatectomy
(most frequently bilateral nerve-sparing), recovery oferections occurred in approximately two-thirds
(571 of 858and 342 of 503the recovery rate
aNone of the serious AEs were considered treatment related.
was inversely related to age at surgery. In contrast, in
bThe only treatment-related AEs that were associated with patient
a series of 1072 Medicare patients, mostly consisting
discontinuation were mild fatigue, headache and dyspepsia in
of older patients with lower rates of preoperative
one patient treated with sildenafil 50 mg, and mild dyspepsia andsevere headache in a second patient treated with sildenafil 50 mg.
potency, only 11% had erections sufficient forintercourse following surgeryIn a meta-analysisof 14 studies conducted through 2001, including
for 9 months, beginning 1 month after bilateral
over 600 patients, the probability of maintaining
erectile function was 34% (95% confidence interval
resulted in the return of spontaneous erections in
(CI) 30–38%) within the year following nerve-
27% (n ¼ 14 of 51) of men, compared with only 4%
sparing prostatectomy.The discrepancy between
(n ¼ 1 of 25) of men receiving placebo. These results
the published literature and the results of the
were observed at the end of an 8-week drug-free
current study may reflect differences from our
period (1 year post-surgery) and were supported by
methodology, such as the absence of controls to
International Journal of Impotence Research
Sildenafil and ED after radical prostatectomy
prevent bias, the use of nonvalidated questionnaires
or a less stringent definition of responders. For
compromising the endothelium-dependent and neu-
example, in other studies the criteria for a positive
rogenic relaxation of corpus cavernosum smooth
response are often not well defined, lack details
(that is, on the quality of erections (full versus
increasing synthesis of transforming growth factor-
partial rigidity)) and do not necessarily correspond
b and endothelin, which ultimately leads to vaso-
to the ability to achieve sexual intercourse.
constriction and corporeal fibrosisSildenafil
In contrast to the published literature, we used a
selectively inhibits phosphodiesterase type 5 and
stringent definition of response. The requirement for
thereby prevents cGMP degradation,compensat-
a combined score of at least 8 for Q3 (‘When you
ing for the reduced availability of nitric oxide during
attempted sexual intercourse, how often were you
hypoxia; this enhances smooth muscle relaxation of
able to penetrate your partner?’) and Q4 (‘During
the corpus cavernosum,promoting blood flow to
sexual intercourse, how often were you able to
maintain your erection after you had penetrated
Sildenafil may have unique and more relevant
your partner?’) necessitated a response of ‘Almost
mechanisms of action in preventing long-term ED
always/always’ on Q3 and ‘Sometimes (about half
after nerve-sparing prostatectomy. In patients with
the time)’ on Q4 or a response of ‘Most times (much
chronic heart failure, in whom vascular endothelial
more than half the time)’ on each question. Penetra-
function (vasodilation) is impaired, administration
tion and maintained erection are clinically mean-
of sildenafil improved endothelium-dependent va-
ingful to the patient because they are prerequisite to
sodilation, as demonstrated by improved flow-
satisfactory sexual intercourse. In addition, we
mediated vasodilation compared with placebo.
required an answer of ‘yes’ to the question, ‘Over
Similarly, in patients with type 2 diabetes, low-dose
the past 4 weeks, have your erections been good
sildenafil improved vascular endothelial function.
enough for satisfactory sexual activity?’ This strin-
Also, phosphodiesterase 5 inhibitors have been
gent definition of response was attained by 27% (14
shown to be neuroprotective to cultured spinal
motor and nonmotor neurons,and sildenafil
Because it is now common clinical practice to
increased neurogenesis and reduced neurological
provide sildenafil on an on-demand basis for
deficits in rats treated within 24 h of strokeThus,
variable periods of time after prostatectomy as
therapeutic postoperative intervention with silde-
needed for the symptomatic treatment of ED, recent
nafil may improve corpus cavernosum endothelial
reports of post-prostatectomy potency often reflect
function and promote recovery of nerve function.
this practice pattern. For example, approximatelyhalf of 167 men who were potent before bilateralnerve-sparing radical retropubic prostatectomy used
sildenafil on-demand; recovery of normal erections,
Even with nerve-sparing surgery, most men will
defined as a score of at least 26 on the Erectile
have severe ED a year after prostatectomy, strongly
Function domain of the International Index of
suggesting the need for early primary prevention
Erectile Function, was achieved by 8% of patients
measures. This is the first long-term, prospective,
after 12 months, compared with 51% after 48
blinded study that assessed prophylactic nightly
months.An on-demand study of sildenafil after
dosing of sildenafil on recovery of erectile function
nerve-sparing radical retropubic prostatectomy has
after bilateral nerve-sparing radical retropubic pros-
demonstrated that treatment satisfaction peaked
tatectomy. The failure to complete the study accord-
between 18 and 24 months.These results suggest
ing to its initial power calculations, which were
that further study is needed to determine the
based on anticipated placebo response rates that did
optimum timing and duration of sildenafil therapy.
not hold true, does not negate the importance of the
The mechanism of action of sildenafil in prevent-
findings. Nightly administration of sildenafil for 36
ing long-term ED following bilateral nerve-sparing
weeks beginning 4 weeks after prostatectomy re-
radical retropubic prostatectomy remains unclear
sulted in a marked restorative effect (an increase
but is probably multifactorial. This is in keeping
over placebo in ability to achieve spontaneous
with the apparently multifactorial etiology of ED
erection) 8 weeks after the end of sildenafil treat-
after prostatectomy, in which vascular factors
ment. These results show that pharmacological
appear to be important in some cases and neuro-
intervention during the convalescent period can
genic factors apparently play a major role.This
enhance the recovery of spontaneous erections, and
study clearly demonstrates the profound loss of
provide objective data and a protocol for the now
nocturnal erections after surgery. Hypoxia may be
common clinical practice of providing sildenafil
involved in both temporary and permanent ED
postoperatively for variable periods of time.
following prostatectomy. Hypoxia causes temporary
Prior to surgery, patients should be counseled
ED by significantly reducing the synthesis and
about the realistic outcome and educated about the
release of nitric oxide (the principal mediator of
most effective treatment alternatives available to
penile erection via the nitric oxide/cyclic guanosine
optimize the return of erectile function after surgery. International Journal of Impotence Research
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
These data suggest that there is an advantage in
initiating early primary prevention measures afterbilateral nerve-sparing radical retropubic prostatect-
1 McCullough AR. Prevention and management of erectile
omy, and that more men may regain spontaneous
dysfunction following radical prostatectomy. Urol Clin North
erectile function when treated proactively with
2 Walsh PC, Partin AW, Epstein JI. Cancer control and quality of
sildenafil. Follow-up studies are warranted to
life following anatomical radical retropubic prostatectomy:
support the results of the current study and to
results at 10 years. J Urol 1994; 152: 1831–1836.
examine the effect of lower doses, earlier initiation
3 Klein LT, Miller MI, Buttyan R, Raffo AJ, Burchard M,
of therapy and intermittent therapy, and to deter-
Devris G et al. Apoptosis in the rat penis after penile
mine the optimal duration of therapy. Other unan-
denervation. J Urol 1997; 158: 626–630.
4 User HM, Hairston JH, Zelner DJ, McKenna KE, McVary KT.
swered questions include the mechanism of action
Penile weight and cell subtype specific changes in a post-
of sildenafil in preserving erectile function and
radical prostatectomy model of erectile dysfunction. J Urol
whether sildenafil use results in better return of
function, faster return of function or both.
5 Zippe CD, Raina R, Thukral M, Lakin MM, Klein EA, Agarwal A.
prostatectomy. Curr Urol Rep 2001; 2: 495–503.
6 Meuleman EJ, Mulders PF. Erectile function after radical
prostatectomy: a review. Eur Urol 2003; 43: 95–102.
7 Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L,
Barbieri L et al. Recovery of spontaneous erectile function
This study was funded by Pfizer Inc. Editorial
after nerve-sparing radical retropubic prostatectomy with and
assistance was provided by Deborah M Campoli-
Richards of Complete Healthcare Communications,
results of a prospective, randomized trial. J Urol 1997; 158:
8 Schwartz EJ, Wong P, Graydon RJ. Sildenafil preserves
intracorporeal smooth muscle after radical retropubic prosta-
tectomy. J Urol 2004; 171: 771–774.
9 Montorsi F, Maga T, Strambi LF, Salonia A, Barbieri L, Scattoni V
Gerald Brock: Consultant, investigator for clinical
et al. Sildenafil taken at bedtime significantly increases
research, and speakers bureau member for Pfizer
nocturnal erections: results of a placebo-controlled study.
Inc, Lilly-ICOS, Bayer, GSK, Johnson & Johnson,
10 Rabbani F, Patel M, Scardino PT. Time course of recovery
of potency after bilateral nerve sparing radical prostatectomy.
Francois Giuliano: Investigator for clinical and
preclinical research, meeting lecturer, and member
11 Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J,
of advisory board for Pfizer Inc, Bayer-GSK, Lilly-
Mishra A. The International Index of Erectile Function (IIEF):
ICOS, Johnson & Johnson; preclinical research for
a multidimensional scale for assessment of erectile dysfunc-
Solvay Pharmaceuticals, Roche; investigator for
12 Cappelleri JC, Rosen RC, Smith MD, Mishra A, Osterloh IH.
preclinical research and meeting lecturer for Sanofi-
Diagnostic evaluation of the erectile function domain of the
International Index of Erectile function. Urology 1999; 54:
Larry Levine: Consultant for Pfizer Inc, Lilly-
ICOS, Auxillium, Johnson & Johnson; investigator
13 Hong EK, Lepor H, McCullough AR. Time dependent patient
for clinical research for Pfizer Inc, Bayer-GSK,
satisfaction with sildenafil for erectile dysfunction (ED)after nerve-sparing radical retropubic prostatectomy (RRP).
Auxillium; lecturer for Pfizer Inc, Lilly-ICOS,
Int J Impot Res 1999; 11: S15–S22.
14 Catalona WJ, Ramos CG, Carvalhal GF. Contemporary results
Larry Lipshultz: Consultant for Pfizer Inc, Lilly-
of anatomic radical prostatectomy. CA Cancer J Clin 1999; 49:
ICOS, Auxillium, and Solvay Pharmaceuticals;
investigator for clinical research for Pfizer Inc and
15 Catalona WJ, Carvalhal GF, Mager DE, Smith DS. Potency,
continence and complication rates in 1870 consecutive radical
retropubic prostatectomies. J Urol 1999; 162: 433–438.
Andrew McCullough: Consultant for Pfizer Inc,
16 Fowler Jr FJ, Barry MJ, Lu-Yao G, Wasson J, Roman A,
Lilly-ICOS, Auxillium, Johnson & Johnson; investi-
Wennberg J. Effect of radical prostatectomy for prostate cancer
gator for clinical research for Pfizer Inc, Lilly-ICOS,
on patient quality of life: results from a Medicare survey.
Bayer-GSK, Guilford Pharmaceuticals, Ion Channel,
17 Robinson JW, Moritz S, Fung T. Meta-analysis of rates of
Johnson & Johnson and Schering Plough; advisory
erectile function after treatment of localized prostate carcino-
board and lecturer for Pfizer Inc, Lilly-ICOS and
ma. Int J Radiat Oncol Biol Phys 2002; 54: 1063–1068.
18 Dubbelman YD, Dohle GR, Schroder FH. Sexual function
before and after radical retropubic prostatectomy: a systematicreview of prognostic indicators for a successful outcome. Eur
Medical System, Bayer-GSK, Johnson & Johnson,
19 Ignarro LJ, Bush PA, Buga GM, Wood KS, Fukuto JM, Rajfer J.
Harin Padma-Nathan: Consultant, received grant
Nitric oxide and cyclic GMP formation upon electrical field
support (for this and other clinical trials) from, and
stimulation cause relaxation of corpus cavernosum smooth
participated in CME educational program for Pfizer
muscle. Biochem Biophys Res Commun 1990; 170: 843–850.
20 Bush PA, Aronson WJ, Buga GM, Rajfer J, Ignarro LJ. Nitric
Inc, Lilly-ICOS, Bayer-GSK, NexMed and Palatin
oxide is a potent relaxant of human and rabbit corpus
cavernosum. J Urol 1992; 147: 1650–1655. International Journal of Impotence Research
Sildenafil and ED after radical prostatectomy
21 Azadzoi KM, Kim N, Brown ML, Goldstein I, Cohen RA,
26 Katz SD. Potential role of type 5 phosphodiesterase inhibition
Saenz de Tejada I. Endothelium-derived nitric oxide and
in the treatment of congestive heart failure. Congest Heart Fail
smooth muscle tone. J Urol 1992; 147: 220–225.
27 Katz SD, Balidemaj K, Homma S, Wu H, Wang J, Maybaum S.
22 Kim N, Vardi Y, Padma-Nathan H, Daley J, Goldstein I, Saenz
de Tejada I. Oxygen tension regulates the nitric oxide pathway.
Physiological role in penile erection. J Clin Invest 1993; 91:
patients with chronic heart failure. J Am Coll Cardiol 2000;
23 Moreland RB. Is there a role of hypoxemia in penile fibrosis: a
28 Desouza C, Parulkar A, Lumpkin D, Akers D, Fonseca VA.
viewpoint presented to the Society for the Study of Impotence.
Acute and prolonged effects of sildenafil on brachial artery
Int J Impot Res 1998; 10: 113–120.
flow-mediated dilatation in type 2 diabetes. Diabetes Care
24 Boolell M, Allen MJ, Ballard SA, Gepi-Attee S, Muirhead GJ,
Naylor AM et al. Sildenafil: an orally active type 5 cyclic
29 Nakamizo T, Kawamata J, Yoshida K, Kawai Y, Kanki R,
GMP-specific phosphodiesterase inhibitor for the treatment of
Sawada H et al. Phosphodiesterase inhibitors are neuropro-
penile erectile dysfunction. Int J Impot Res 1996; 8: 47–52.
tective to cultured spinal motor neurons. J Neurosci Res 2003;
25 Ballard SA, Gingell CJ, Tang K, Turner LA, Price ME, Naylor
AM. Effects of sildenafil on the relaxation of human corpus
30 Zhang R, Wang Y, Zhang L, Zhang Z, Tsang W, Lu M et al.
cavernosum tissue in vitro and on the activities of cyclic
Sildenafil (Viagra) induces neurogenesis and promotes
nucleotide phosphodiesterase isozymes. J Urol 1998; 159:
functional recovery after stroke in rats. Stroke 2002; 33:
International Journal of Impotence Research
must contact Horizon directly. This will enable Horizon to better answer your questions and service you in the event that you may need any assistance. For questions or assistance, please direct your email to productsupport@horizonhobby.com, or call 877.504.0233 toll free to speak to a service technician. Inspection or Repairs If this Product needs to be inspected or repaired, please call for a
Guidelines on Handling Chemical Carcinogens, Teratogens and Mutagens 1995 New Edition incorporating requirements of CoSHH 1994 1. Background, Scope and Purpose of the Code The Control of Substances Hazardous to Health Regulations 1994 (section 7)introduced specific legal duties relating to the use of carcinogens, including a hierarchyof precautions which are MANDATORY . In addition the Ap
 International Journal of Impotence Research (2008) 20, 479–486& 2008 Nature Publishing Group All rights reserved
ORIGINAL ARTICLERandomized, double-blind, placebo-controlled study ofpostoperative nightly sildenafil citrate for the prevention of erectiledysfunction after bilateral nerve-sparing radical prostatectomy
H Padma-Nathan1, AR McCullough2, LA Levine3, LI Lipshultz4, R Siegel5,9, F Montorsi6, F Giuliano7and G Brock8, on behalf of the Study Group10
1Department of Urology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA;
2Department of Urology, New York University School of Medicine, New York University Medical Center, New York, NY,USA; 3Department of Urology, Rush Medical College, Rush University, Chicago, IL, USA; 4Scott Department of Urology,Baylor College of Medicine, Houston, TX, USA; 5Sexual Health Team, Pfizer Inc, New York, NY, USA; 6Department ofUrology, University Vita Salute San Raffaele, Milan, Italy; 7Department of Physical Medicine and Rehabilitation, RaymondPoincare´ Hospital, Garches, France and 8Department of Urology, University of Western Ontario, London, ON, Canada
Four weeks after bilateral nerve-sparing radical retropubic prostatectomy, men with normalerectile function before surgery were randomized to double-blind sildenafil (50 or 100 mg) orplacebo nightly for 36 weeks, followed by an 8-week drug-free period before assessment of erectilefunction. Enrollment was prematurely ceased and only 76 men completed because, assuming aplacebo response rate similar to the published literature (for example, 34% in meta-analysis), the25% response at blinded interim review suggested a lack of treatment effect. On the contrary,spontaneous erectile function (a combined score of X8 for questions 3 and 4 of the InternationalIndex of Erectile Function and a positive response to ‘Were erections good enough for satisfactorysexual activity?’) occurred in only 4% of the placebo group (n ¼ 1 of 25) versus 27% (n ¼ 14 of 51,P ¼ 0.0156, Fisher’s exact test) of the sildenafil group. Nightly sildenafil administration for 36 weeksafter surgery markedly increased the return of normal spontaneous erections.
International Journal of Impotence Research (2008) 20, 479–486& 2008 Nature Publishing Group All rights reserved
ORIGINAL ARTICLERandomized, double-blind, placebo-controlled study ofpostoperative nightly sildenafil citrate for the prevention of erectiledysfunction after bilateral nerve-sparing radical prostatectomy
H Padma-Nathan1, AR McCullough2, LA Levine3, LI Lipshultz4, R Siegel5,9, F Montorsi6, F Giuliano7and G Brock8, on behalf of the Study Group10
1Department of Urology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA;
2Department of Urology, New York University School of Medicine, New York University Medical Center, New York, NY,USA; 3Department of Urology, Rush Medical College, Rush University, Chicago, IL, USA; 4Scott Department of Urology,Baylor College of Medicine, Houston, TX, USA; 5Sexual Health Team, Pfizer Inc, New York, NY, USA; 6Department ofUrology, University Vita Salute San Raffaele, Milan, Italy; 7Department of Physical Medicine and Rehabilitation, RaymondPoincare´ Hospital, Garches, France and 8Department of Urology, University of Western Ontario, London, ON, Canada
Four weeks after bilateral nerve-sparing radical retropubic prostatectomy, men with normalerectile function before surgery were randomized to double-blind sildenafil (50 or 100 mg) orplacebo nightly for 36 weeks, followed by an 8-week drug-free period before assessment of erectilefunction. Enrollment was prematurely ceased and only 76 men completed because, assuming aplacebo response rate similar to the published literature (for example, 34% in meta-analysis), the25% response at blinded interim review suggested a lack of treatment effect. On the contrary,spontaneous erectile function (a combined score of X8 for questions 3 and 4 of the InternationalIndex of Erectile Function and a positive response to ‘Were erections good enough for satisfactorysexual activity?’) occurred in only 4% of the placebo group (n ¼ 1 of 25) versus 27% (n ¼ 14 of 51,P ¼ 0.0156, Fisher’s exact test) of the sildenafil group. Nightly sildenafil administration for 36 weeksafter surgery markedly increased the return of normal spontaneous erections. Sildenafil and ED after radical prostatectomy
of spontaneous erections after nerve-sparing radical
50- or 100-mg sildenafil, or matching placebo, was
retropubic prostatectomy.Despite this benefit,
taken once daily at nighttime. Erectile function was
pain, complications and inconvenience detract from
assessed, and plethysmography was conducted in
the willingness of patients to use intracavernosal
the subgroup, after 12, 24 and 36 weeks of treatment.
Sildenafil and ED after radical prostatectomy
of spontaneous erections after nerve-sparing radical
50- or 100-mg sildenafil, or matching placebo, was
retropubic prostatectomy.Despite this benefit,
taken once daily at nighttime. Erectile function was
pain, complications and inconvenience detract from
assessed, and plethysmography was conducted in
the willingness of patients to use intracavernosal
the subgroup, after 12, 24 and 36 weeks of treatment. Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
expected based on rates of spontaneous recovery of
The primary measure was the percentage of patients
erectile function reported in the published litera-
ture.After enrollment ceased, two US study
definition was established a priori as those patients
centers remained active to complete all the study
who, at the end of phase 3, had a combined score of
visits in the ongoing patients in the plethysmogra-
at least 8 for Q3 and Q4 of the International Index
phy subgroup and to provide information to aid in
of Erectile Function, and also answered ‘yes’ to
the question, ‘Over the past 4 weeks, have your
All statistical analyses were performed using
erections been good enough for satisfactory sexual
Statistical Analysis System software version 6.12
for efficacy analyses and version 8.2 for demo-
Secondary measures were changes from baseline
graphic and safety analyses. Primary and secondary
in the six-item Erectile Function domain of the
efficacy variables were analyzed in patients who
International Index of Erectile Function and, for
completed the 36-week double-blind treatment
the plethysmography subgroup, the duration of
period and the 8-week drug-free evaluation period.
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
expected based on rates of spontaneous recovery of
The primary measure was the percentage of patients
erectile function reported in the published litera-
ture.After enrollment ceased, two US study
definition was established a priori as those patients
centers remained active to complete all the study
who, at the end of phase 3, had a combined score of
visits in the ongoing patients in the plethysmogra-
at least 8 for Q3 and Q4 of the International Index
phy subgroup and to provide information to aid in
of Erectile Function, and also answered ‘yes’ to
the question, ‘Over the past 4 weeks, have your
All statistical analyses were performed using
erections been good enough for satisfactory sexual
Statistical Analysis System software version 6.12
for efficacy analyses and version 8.2 for demo-
Secondary measures were changes from baseline
graphic and safety analyses. Primary and secondary
in the six-item Erectile Function domain of the
efficacy variables were analyzed in patients who
International Index of Erectile Function and, for
completed the 36-week double-blind treatment
the plethysmography subgroup, the duration of
period and the 8-week drug-free evaluation period. Sildenafil and ED after radical prostatectomy
had concomitant hypertension (n ¼ 10–12), hyper-
Response rate after 36 weeks on study drug and 8
lipidemia (n ¼ 10–11) and ischemic heart disease
(n ¼ 1–2). All patients had good erectile functionat screening and developed ED as a result of
The 36-week double-blind treatment period was
completed by 82 men. The subsequent 8-week
drug-free evaluation period was completed by 76
men, who constituted the population analyzed for
efficacy: placebo, n ¼ 25; sildenafil 50 mg, n ¼ 23;
sildenafil 100 mg, n ¼ 28. Of these 76 men, 54 were
enrolled at the two US study centers, whichremained active to complete all the study visits in
aDefined as those who scored X8 on Q3 and Q4 of the
ongoing patients, and were included in the plethys-
International Index of Erectile Function and also answered ‘yes’
to the question ‘Over the past 4 weeks, have your erections been good
enrolled at three other North American study
enough for satisfactory sexual activity?’
centers. The eight men randomized at the other six
P ¼ 0.02 versus placebo (two-tailed Fisher’s exact test).
Sildenafil and ED after radical prostatectomy
had concomitant hypertension (n ¼ 10–12), hyper-
Response rate after 36 weeks on study drug and 8
lipidemia (n ¼ 10–11) and ischemic heart disease
(n ¼ 1–2). All patients had good erectile functionat screening and developed ED as a result of
The 36-week double-blind treatment period was
completed by 82 men. The subsequent 8-week
drug-free evaluation period was completed by 76
men, who constituted the population analyzed for
efficacy: placebo, n ¼ 25; sildenafil 50 mg, n ¼ 23;
sildenafil 100 mg, n ¼ 28. Of these 76 men, 54 were
enrolled at the two US study centers, whichremained active to complete all the study visits in
aDefined as those who scored X8 on Q3 and Q4 of the
ongoing patients, and were included in the plethys-
International Index of Erectile Function and also answered ‘yes’
to the question ‘Over the past 4 weeks, have your erections been good
enrolled at three other North American study
enough for satisfactory sexual activity?’
centers. The eight men randomized at the other six
P ¼ 0.02 versus placebo (two-tailed Fisher’s exact test).
 Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
Erectile Function domain scores and by nocturnal
penile plethysmography. The similar response rate
between the 50- and 100-mg doses of sildenafil
suggests future study to identify the minimally
The study results reveal that the majority of men
who undergo bilateral nerve-sparing radical retro-
pubic prostatectomy have ED a year later. Because
we assumed a placebo response rate similar to that
of the published literature (see below), the low
overall response rate (25% (9 of 35)) at the blinded
interim review suggested a lack of treatment effect
and resulted in a decision to prematurely cease
enrollment. Most discontinuations were because of
study closure (n ¼ 19). Although prematurely ceas-ing enrollment and closing study sites precluded
Figure 1 Nocturnal penile rigidity at the base of the penis asassessed using RigiScan, in responders (n ¼ 10) and nonrespon-
achieving the original sample size goal, the treat-
ders (n ¼ 25) to sildenafil treatment, before and 4 and 48 weeks
ment assignment followed the original randomiza-
after prostatectomy. Responders were a priori defined as those
tion ratio. Given the ultimate number of patients,
patients who, at the end of the 8-week drug-free period, had a
use of Fisher’s exact test (two-tailed), with the
combined score of at least 8 on Q3 and Q4 from the International
Bonferroni adjustment to account for multiple
Index of Erectile Function (scores for each question ranged from 0to 5) and answered ‘yes’ to the question ‘Over the past 4 weeks,
comparisons with placebo, was an appropriate
have your erections been good enough for satisfactory sexual
alternative statistical test to the originally planned
activity?’ Data are shown as median and 25th to 75th percentile
statistical analysis. However, the results should be
bars, with 10th and 90th percentile limits. Of the 54 men who
interpreted in the context of patients actually
underwent RigiScan assessment, 19 others were randomized toplacebo.
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
Erectile Function domain scores and by nocturnal
penile plethysmography. The similar response rate
between the 50- and 100-mg doses of sildenafil
suggests future study to identify the minimally
The study results reveal that the majority of men
who undergo bilateral nerve-sparing radical retro-
pubic prostatectomy have ED a year later. Because
we assumed a placebo response rate similar to that
of the published literature (see below), the low
overall response rate (25% (9 of 35)) at the blinded
interim review suggested a lack of treatment effect
and resulted in a decision to prematurely cease
enrollment. Most discontinuations were because of
study closure (n ¼ 19). Although prematurely ceas-ing enrollment and closing study sites precluded
Figure 1 Nocturnal penile rigidity at the base of the penis asassessed using RigiScan, in responders (n ¼ 10) and nonrespon-
achieving the original sample size goal, the treat-
ders (n ¼ 25) to sildenafil treatment, before and 4 and 48 weeks
ment assignment followed the original randomiza-
after prostatectomy. Responders were a priori defined as those
tion ratio. Given the ultimate number of patients,
patients who, at the end of the 8-week drug-free period, had a
use of Fisher’s exact test (two-tailed), with the
combined score of at least 8 on Q3 and Q4 from the International
Bonferroni adjustment to account for multiple
Index of Erectile Function (scores for each question ranged from 0to 5) and answered ‘yes’ to the question ‘Over the past 4 weeks,
comparisons with placebo, was an appropriate
have your erections been good enough for satisfactory sexual
alternative statistical test to the originally planned
activity?’ Data are shown as median and 25th to 75th percentile
statistical analysis. However, the results should be
bars, with 10th and 90th percentile limits. Of the 54 men who
interpreted in the context of patients actually
underwent RigiScan assessment, 19 others were randomized toplacebo. Sildenafil and ED after radical prostatectomy
prevent bias, the use of nonvalidated questionnaires
or a less stringent definition of responders. For
compromising the endothelium-dependent and neu-
example, in other studies the criteria for a positive
rogenic relaxation of corpus cavernosum smooth
response are often not well defined, lack details
(that is, on the quality of erections (full versus
increasing synthesis of transforming growth factor-
partial rigidity)) and do not necessarily correspond
b and endothelin, which ultimately leads to vaso-
to the ability to achieve sexual intercourse.
Sildenafil and ED after radical prostatectomy
prevent bias, the use of nonvalidated questionnaires
or a less stringent definition of responders. For
compromising the endothelium-dependent and neu-
example, in other studies the criteria for a positive
rogenic relaxation of corpus cavernosum smooth
response are often not well defined, lack details
(that is, on the quality of erections (full versus
increasing synthesis of transforming growth factor-
partial rigidity)) and do not necessarily correspond
b and endothelin, which ultimately leads to vaso-
to the ability to achieve sexual intercourse. Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
These data suggest that there is an advantage in
initiating early primary prevention measures afterbilateral nerve-sparing radical retropubic prostatect-
1 McCullough AR. Prevention and management of erectile
omy, and that more men may regain spontaneous
dysfunction following radical prostatectomy. Urol Clin North
erectile function when treated proactively with
2 Walsh PC, Partin AW, Epstein JI. Cancer control and quality of
sildenafil. Follow-up studies are warranted to
life following anatomical radical retropubic prostatectomy:
support the results of the current study and to
results at 10 years. J Urol 1994; 152: 1831–1836.
Sildenafil and ED after radical prostatectomyH Padma-Nathan et al
These data suggest that there is an advantage in
initiating early primary prevention measures afterbilateral nerve-sparing radical retropubic prostatect-
1 McCullough AR. Prevention and management of erectile
omy, and that more men may regain spontaneous
dysfunction following radical prostatectomy. Urol Clin North
erectile function when treated proactively with
2 Walsh PC, Partin AW, Epstein JI. Cancer control and quality of
sildenafil. Follow-up studies are warranted to
life following anatomical radical retropubic prostatectomy:
support the results of the current study and to
results at 10 years. J Urol 1994; 152: 1831–1836. Sildenafil and ED after radical prostatectomy
21 Azadzoi KM, Kim N, Brown ML, Goldstein I, Cohen RA,
26 Katz SD. Potential role of type 5 phosphodiesterase inhibition
Saenz de Tejada I. Endothelium-derived nitric oxide and
in the treatment of congestive heart failure. Congest Heart Fail
smooth muscle tone. J Urol 1992; 147: 220–225.
Sildenafil and ED after radical prostatectomy
21 Azadzoi KM, Kim N, Brown ML, Goldstein I, Cohen RA,
26 Katz SD. Potential role of type 5 phosphodiesterase inhibition
Saenz de Tejada I. Endothelium-derived nitric oxide and
in the treatment of congestive heart failure. Congest Heart Fail
smooth muscle tone. J Urol 1992; 147: 220–225.