Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Guidelines for primary care on commencement of anti-arrhythmic therapy
Guidance for Primary Care on Commencement of Anti-Arrhythmic Therapy
Background
NSF Chapter 8 has made recommendations on the management of atrial fibrillation. These include the use of sotalol and flecainide, drugs that GPs may be unfamiliar with. The AGW Arrhythmia sub-group has drawn up a protocol for AF management, based on NSF Chapter 8 that includes commencement of sotalol and flecainide treatment in Primary Care in selected cases. The reason for caution is that all anti-arrhythmic drugs carry a risk of pro-arrhythmia, which occasionally can be fatal. However, studies show that the risk is negligible in those without coronary artery disease and normal left ventricular function. This is why the NSF guidelines allow usage in this group. There is also concern that flecainide may occasionally elevate pacing threshold in pacemaker patients. Relevant Pharmacological advice
BNF 52: Sotalol: “with ECG monitoring and measurement of corrected QT interval”, see below). Flecainide: “initiated under direction of hospital consultant”, which this guidance constitutes. On line Summary of Product Characteristics: Sotalol: “caution if QTc on treatment >500, stop if >550”. Guidance
A full cardiovascular history and examination with 12 lead ECG should be carried out before starting sotalol or flecainide. A patient can be regarded as being free of coronary artery disease and left ventricular dysfunction and sotalol (titrated from 40-240mg bd) or flecainide (titrated from 50-150mg bd) started in Primary Care if:
There is no suggestion from the history of angina, MI, heart failure, previous
abnormal CXR, echo or angiogram or other history to suggest structural heart disease. The examination is normal.
The patient does not have a pacemaker (flecainide).
Rest ECG is normal, including pre-treatment QTc (Normal = <420). If in doubt, local
cardiologist can review ECG by post, fax or e mail. ECG should be repeated after 2 weeks and after increases in dose and advice taken if QTc >500 and stopped if QTc >550
Usual beta-blocker contraindications are considered with sotalol
In cases where there is doubt, or if the above conditions are not satisfied, a referral should be made to a local cardiologist, preferably a heart rhythm specialist prior to commencing therapy.
AGW Cardiac Network Guidelines for Primary Care on Commencement of Anti-arrhythmic Therapy Review Date April 2009 Notes on calculation of QTc
Many ECG machines do this automatically QTc = QT( in seconds)
1 small square on ECG at 25 mm/s = 0.04s 1 large square on ECG at 25 mm/s = 0.2s Example: QT interval = 0.44 s RR interval = 1.12s RR = 1.06 QTc = 0.44/1.06 = 0.42 For those of a mathematical bent, it will be noted that this quantity is usually given units of seconds, though in fact its dimensions are [sec] -1, which rather gives doubt to the idea that this is “QT interval corrected for heart rate”, but that is another story!
Note on Amiodarone
Amiodarone should be used in those with structural heart disease who need an antiarrhythmic agent other than a beta blocker since its proarrhythmic effect is lower. While it is not used as first line because of side effects it can be effective and well tolerated. Regimen is 200mg tds for 1 week, 200mg bd for 2 weeks then 200 mg per day. Once rhythm is stable down titration to 100 or even 50 mg per day can be tried. Routine screening include TFT and LFT before commencement, after 1 month and then 6 monthly with annual CXR. AGW Cardiac Network Guidelines for Primary Care on Commencement of Anti-arrhythmic Therapy Review Date April 2009
Streamlining the development of new cold tolerance rice varietiesDan Waters & Robert HenrySouthern Cross University, Lismore in a rice hull • Cold temperatures during the rice growing season can result in significant yield loss and significant income loss to the industry• The deep water required on the rice field throughout the cold sensitive early microspore stage of pollen developmen
Non-Hodgkin Lymphoma Protocol applies to non-Hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2004 Procedures • Cytology (No Accompanying Checklist) • Biopsy • Resection of Lymph Node or Other Organ Authors Carolyn Compton, MD, PhD Department of Pathology, McGill University, Montreal, Quebec, Canada
 Guidance for Primary Care on Commencement of Anti-Arrhythmic Therapy
Guidance for Primary Care on Commencement of Anti-Arrhythmic Therapy 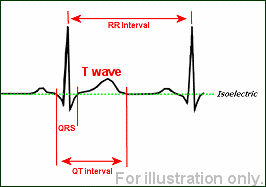
 Notes on calculation of QTc
Notes on calculation of QTc