Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Microsoft word - imic_jp.doc
IMPLANT-SUPPORTED ANTERIOR TOOTH RESTORATION
Various options are available for restoring anterior teeth. Their choice is dictated by the
severity of infection of the teeth to be extracted and the pocket depth. Immediate single-stage
implant placement proved to be the least traumatic option, which best preserved the soft
tissue. A differential use of surgical and prosthodontic techniques is indispensable to account
for conditions in the individual case. Given an adequate amount of hard tissue, soft tissue
contours can be expected to return to normal. Immediate implants combined with a soft tissue
support have been found to ensure that the depth of even larger pockets is stable for years.
Keywords: Dental implants, Immediate implantation, delayed implantation, implant supported, immediate loading.
Esthetic implant-supported anterior tooth restoration is the greatest challenge both surgeons
and prosthodontists are confronted with. Ever since immediate implants have been available,
there is conclusive scientific evidence showing that soft and hard tissue loss can only be
prevented by implants. Although their indications are limited in the anterior maxilla,
immediate implants should invariably be considered whenever an upper anterior tooth is
extracted. However, esthetic aspects or periodontal infections may rule out immediate implant
placement so that the risk of minor hard and soft tissue loss associated with delayed
immediate implant placement may have to be put up with (1, 2,3).
The surgeon is called upon to keep in mind the subsequent prosthodontic work when placing
implants and to make sure that implant positioning or bone grafting permit an optimal crown
design and restoration of the papilla. (4) Implant systems are designed for differential
diameters. Because of the tapering roots of upper anterior teeth, the placement of screw-
shaped implants may be more difficult in the anterior maxilla than that of conical implants.
The implant – to – tooth distance and the inter-implant distance as well as the hard tissue
support of the mucosa also need to be attended to (5, 6, 7).
The recommendations for immediate implant placement reported by Schulte continue to be
valid and are still being followed in minimal invasive surgery today. (1, 8, 9)
With delayed immediate implant placement, some soft and hard tissue loss is inevitable
despite the short interval of 6 to 8 weeks. The severity of ostitis or periodontitis following
tooth extractions is one of the determinants of tissue loss (2). Thanks to improved
prosthodontic materials like zirconium oxide, electroplated crowns or ceramic suprastructures,
less than optimal conditions post surgery can still be turned into a satisfactory or at least
acceptable prosthodontic outcome. However, this requires the availability of an adequate
amount of soft tissue. Temporary crowns help to contour and stabilize the soft tissue for
subsequent definitive rehabilitation after an appropriate healing time (11). Various options are
available for successfully replacing the upper anterior teeth:
(a) customized tissue contouring abutments
2. Delayed immediate implants placed 6 to 8 weeks post extraction with
(a) immediate impression taking and insertion of the definitive crown after
(b) soft tissue contouring with provisional crowns followed by later definitive
For these four options, long-term results are presented on the basis of case reports.
1. (a) Immediate implants with customized tissue contouring abutments
A female patient aged 68 years was referred for implants. 12, 11 and 22 showed grade 2
loosening. On probing, the pocket depth around all teeth was 11 mm causing exudation of pus
and recurrent periodontal abscesses. The patient presented with a deep bite. The non-
removable bridge she had been rehabilitated with was partly supported by implants.
Following periodontal pretreatment to control the acute infection, fixed bridgework was
recommended for the time the implants would need to heal. 21 was trimmed to accommodate
a crown with the neighboring teeth 22, 11 and 12 as pontics. Metal rests were bonded on 13
and 23 palatally in terms of a Maryland bridge
without prior trimming. The metal bridge was
veneered with plastic. One week later 12, 11
and 22 were extracted in local anesthesia and
implants were placed despite the deep pockets.
The inflammatory periodontal lesions had
recommendations the implants, i.e. FRIALIT-2 Synchro screws with a Cellplus surface
(Dentsply/Friadent, Mannheim, Germany), were placed palatally (Fig. 1).
Implant diameters were 4.5 mm for 12, 5.5 mm
for 11 and 4.5 mm for 22. Implant length was
15 mm throughout. All implants were anchored
in the cortical bone of the nasal floor (Fig. 2 ).
The implants were closely spaced in the bone with an inter-implant distance of no more than 1
to 1.5 mm. Implants with a smaller diameter did not achieve primary stability and had to be
replaced by larger ones. Alternatively, the periodontal lesions could have been curetted to the
point of healing. However, this would have caused substantial resorption of the mucosa and
the alveolar process. Despite a pocket depth of 11 mm around 21, 9 mm around 12 and 9 mm
around 22, the implants were seated down to the limbus. As tissue contouring abutments of
adequate length to support the mucosa together with the papillae to the level of the
mucogingival junction were not available, ProTect abutments were customized to the right
size. All implants achieved primary stability.
On the day of implant placement impressions were taken and the lab technician fabricated
plastic-coated, highly polished tissue contouring abutments matching the ovoid diameters of
the teeth. While he was at work, transfer copings were attached for 1 to 2 hours to maintain
stable mucosal conditions and prevent mucosal collapse.
When ready, the customized tissue contouring abutments were put in place, the Maryland
bridge was bonded with Panavia® (Kuraray Dent) and antibiotics were administered.
The customized tissue contouring abutments were checked for stability at weekly intervals
and the mucosa was examined for alterations, shape and color. As the small inter-implant
distances prevented papilla regeneration, the original tissue contouring abutments were
replaced by other customized highly polished, plastic-veneered abutments with the diameters
reduced by platform switching. With these, papilla-like soft tissue developed within the
mucosa and persisted to the time of definitive management. Platform switching was also used
for the definitive restoration, i.e. the 4.5 mm implant in 12 was fitted with a 3.8mmD
abutment and the 5.5 mm implant in 11 with a 4.5 mmD abutment. Both of these abutments
were custom-designed. By the time of definitive management, the mucogingival junction was
only slightly lower than around the natural tooth 21. The 3 implant-supported electroplated
crowns were mounted on customized final abutments and retained with a horizontal screw.
An electroplated crown was also used on 21 to avoid a translucency mismatch.
At the follow-up visits scheduled at regular
intervals in the subsequent 2 years, the
vestibular probing depths dropped to 7 mm
around 12, 8 mm around 11 and 6 mm around
22. Compared to 21, which was vital, the
reduction of the mucogingival junction was
negligible. The papillae between the implant-
1. (b) Immediate implants with definitive crowns
This patient, a 38-years-old female, presented
with a root canalled, loosened (grade 2) 22.
significantly abnormal. After duly considering
all alternative treatments the patient opted for
definitive crown. 22 was extracted in local
anesthesia. For implant placement Schulte´s
recommendations for tooth extraction, implant
inclination and positioning to support the facial
cortical plate were followed. Immediately after
(Dentsply/Friadent, Mannheim, Germany) with
a grit-blasted acid-etched surface, a diameter of
4.5 mm and a length of 15 mm was placed, an
impression was taken, a tissue contouring abutment was mounted on the implant and the
patient was sent home for the day (Figs. 4-5).
In the meantime, the lab technician fabricated a horizontally screw-retained electroplated
crown, which was veneered with ceramic. Rather than glaze-baked, the crown surface was
polished mechanically to leave some scope for subsequent esthetic and functional crown
finishing, i.e. baking the ceramic on metal, which increases the compressive force applied to
the papilla and promotes papilla repair.
In the evening of the same day, the horizontally screw-retained electroplated crown matched
in shape to 22 was mounted. The mucosa had meanwhile been stabilized by the tissue
contouring abutment. On account of the compressive force generated by the permanent crown
the supracoronal tissue briefly became anemic. The anemic reaction ought to subside within 8
to 10 minutes. If it does not, the compromised nutritive supply of the soft tissue is bound to
Crown contacts were avoided during maximal intercuspidation, protrusion and lateral shift.
The patient was recalled weekly and instructed to clean the tooth gently and not to bite or
chew with it. The crown was checked for stability throughout the healing time of the implant.
It was never taken off. The mucosa was sound without any loss in height or papillary volume.
After about 3 months, the crown was removed
and finalized esthetically and functionally in
mucosa was at the same level as that around
the neighboring teeth. The distances of the
papilla from the contact points, the incisal edge and the implant base were also unchanged.
All of the soft tissue had successfully been preserved (Fig. 6):
2. (a) Delayed immediate implants with immediate impression taking and insertion of the
This 34-years-old female, who had lost 22 and was provided with a removable temporary
partial, came for implant treatment. The tooth had been extracted elsewhere about 8 weeks
ago. Even during this short interval, substantial hard and soft tissue loss had occurred by
clinical evidence. The patient reported that the extraction had been very difficult and that she
Treatment alternatives were discussed with her
and implant-supported restoration combined
The neighboring teeth were caries-free. The
alveolar process was exposed through a palatal
incision in local anesthesia. The bone atrophy,
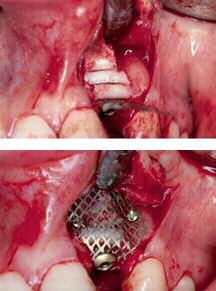
which had already been noted on palpation, was confirmed intra-operatively (Fig. 7).
indicated the need for an implant with a
diameter of 3.8 mm and a length of 15 mm. A
blasted and acid-etched surface was chosen.
The bone from the intended implant site was
removed with a trephine. Implant placement
itself was uneventful. One third of the implant
surface was not buried in the host bone.
prosthodontic work, an impression was taken
immediately after implant placement. This left the lab technician more than 3 months´ time
for fabricating the crown. After impression taking the area of bone loss was grafted with bone
harvested from the retromolar region and with bone chips from the bone collector and the
trephine. The graft was covered with a titanium mesh secured with screws before primary
Healing was uneventful and the implant was uncovered after about 3 months. The titanium
mesh was removed through the original incision. The quality of the alveolar process had
substantially improved. The originally exposed implant surface was now covered by bone.
The final abutment had a collar height of 0.5 mm and the crown, which had meanwhile been
fabricated in the lab, was immediately mounted and retained with a horizontal screw. With
interdental and inter-implant sutures in place, the wound was allowed to heal.
After about 4 weeks, the bland mucosa had
become attached to the implant. At 2 years
peri-implant mucosal conditions were stable
despite the loss of about 1 mm in mucosal
height compared to the neighboring tooth. The
This patient, a 34-years-old female, presented
with loosening of 11 and 12. (Fig. 10a) As
these teeth were not salvageable because of
periodontal abscesses, they were extracted and
the patient was temporized with a removable
partial. Implants were placed about 8 weeks
mucoperiosteal flap was raised through a
palatal incision spanning 11 and 12. Alveolar bone loss was apparent both vertically and
horizontally. Two FRIALIT-2 Synchro implants were placed, i.e. a 4.5 mmD in 12 and a 5.5
mmD in 11. Both implants were 15 mm long. They were not fully buried in bone, but left
exposed about 2 mm above the alveolar process for augmentation with a bone substitute. The
vertical 2-mm defect and the horizontal defect were grafted with BIO-OSS® (Geistlich,
Wohlhusen, Switzerland). The grafts were covered with a resorbable membrane (Vycryl,
Ethicon, Norderstedt, Germany), which was secured with the occlusal screws of the implants.
Following submucosal vestibuloplasty the wound was closed with tension-free sutures. The
patient was prescribed an anti-inflammatory (diclofenac) and an antibiotic (clindamycin) to
prevent swelling and infection. Healing was uneventful. About 3 months later the implants
were uncovered through the original incision, tissue contouring abutments were mounted on
them and stabilized with inter-implant sutures. The mucoperiosteal flap was repositioned and
sutured against the abutments. For adequate mucosal support extra-high tissue contouring
abutments were chosen. Loading by the denture was not allowed for about 1 week. About 8
days later, an impression was taken and temporary crowns were inserted on the same day.
These were originally intended to be left in place for about 3 to 6 months for satisfactory soft
tissue contouring. However, the soft tissue support provided by the crowns was found to be
inadequate. As the patient spent some time abroad, she was prevented from showing up for
crown recontouring. As a result, definitive rehabilitation was done after about 1 year. The
inadequate soft tissue support had caused mucosal loss both vertically and horizontally.
Electroplated crowns retained with horizontal screws were chosen for definitive restoration.
The shoulder of the final abutments for the FRIALIT-2 implants was reduced to 0.5 mm for
recontouring the mucosa to match the natural ovoid crown shape. In addition, the abutments
were extended in length to counteract the leverage on the crowns. A small ischemic area just
above the crown margin was seen after the crowns were mounted. This disappeared within
approximately 8 to 10 minutes. Definitive management was completed by readjusting the
ceramic crowns to provide more support for the papillae and the soft tissue.
At about 2 years after crown insertion the soft tissue was stable. (Fig. 10b)
Gomez-Roman G, Schulte W., d’Hoedt B, et al. The Frialit-2 Implant System: Five-
year clinical experience in single-tooth and immediately postextractions applications.
Int. J Oral Maxl/ofac Implants. 1997; 12:299:309
Wöhrle PS. Single-tooth replacement in the esthetic zone with immediate
provisionalization: fourteen consecutive case report. Pract Periodont Aesth Dent.
Romanos G., Sofortbelastung von enossalen Implantaten im Seitenzahnbereich des
Unterkiefers, Tierexperimentelle und klinische Studien, Quintessenz Verlags GmbH
Tarnow DP, Magne AW, Fletcher P: The effect from the distance front the contact
point to the crest of one on the presence or absence of interproximal dental papilla. J
Saadoun AP, Le Gall MG: Periodontal implications in implant treatment planning for
aesthetic results. Pract Periodontics Aethest Dent 655-664, 1998.
Tarnow DP, Cho SC, Wallace S: The effect of inter-implant distance on the height of
inter-implant hone crest. J Periodontol 71(4):546-549, 2000
Hartmann, H-J. Sofortimplantation mit Sofortbelastung, Identity 5, 2004, 14-16,
Hartmann, H.-J., Ästhetische Frontversorgung mit sofortbelasteten Implantaten, DZW,
Lazzara RJ, Immediate Implant placement into extraction sites: surigal and restorative
advantages, Int J Periodontics Restorative Dent. 1989; 9(5): 332-43.
Hugo O, Prothetische Sofortversorgung nach einzeitiger Chirurgie – Experiment oder
etabliertes Verfahren. Oralchirurgie Journal, 5. J, März 2005, Heft 1 20-24
Bragger U, Pasquali L, Kornman KS: Remodeling of interdental alveolar bone after
periodontal flap procedures assessed by means of computer assisted densitometric
image analysis (CADIA). J Clin Periodontol 15(9):558-564, 1988.
Students Exhibit 3 – 5141.33 HEAD LICE GUIDELINES ON HEAD LICE PREVENTION AND CONTROL FOR SCHOOL DISTRICTS AND CHILD CARE FACILITIES, 2006 Division of Communicable Disease Control California Department of Health Services These guidelines are provided to assist local health departments, elementary schools, preschools, and child care facilities in developing policies a
If no history – then may be diagnosed by finding a significant arrhythmia, cardiacenlargement on X-ray; cyanosis or clubbing, persistent jugular venous distention or adiastolic or presystolic murmur. Systolic murmurs may be functional. Blood volume increases 5O% by 30th week of gestationSystemic vascular resistance decreasesRisk of both hypercoagulability and hemorrhageCounsel regarding: mate

 and 23 palatally in terms of a Maryland bridge
without prior trimming. The metal bridge was
veneered with plastic. One week later 12, 11
and 22 were extracted in local anesthesia and
implants were placed despite the deep pockets.
The inflammatory periodontal lesions had
recommendations the implants, i.e. FRIALIT-2 Synchro screws with a Cellplus surface
(Dentsply/Friadent, Mannheim, Germany), were placed palatally (Fig. 1).
Implant diameters were 4.5 mm for 12, 5.5 mm
for 11 and 4.5 mm for 22. Implant length was
15 mm throughout. All implants were anchored
in the cortical bone of the nasal floor (Fig. 2 ).
The implants were closely spaced in the bone with an inter-implant distance of no more than 1
to 1.5 mm. Implants with a smaller diameter did not achieve primary stability and had to be
replaced by larger ones. Alternatively, the periodontal lesions could have been curetted to the
point of healing. However, this would have caused substantial resorption of the mucosa and
the alveolar process. Despite a pocket depth of 11 mm around 21, 9 mm around 12 and 9 mm
around 22, the implants were seated down to the limbus. As tissue contouring abutments of
adequate length to support the mucosa together with the papillae to the level of the
mucogingival junction were not available, ProTect abutments were customized to the right
size. All implants achieved primary stability.
On the day of implant placement impressions were taken and the lab technician fabricated
plastic-coated, highly polished tissue contouring abutments matching the ovoid diameters of
the teeth. While he was at work, transfer copings were attached for 1 to 2 hours to maintain
stable mucosal conditions and prevent mucosal collapse.
and 23 palatally in terms of a Maryland bridge
without prior trimming. The metal bridge was
veneered with plastic. One week later 12, 11
and 22 were extracted in local anesthesia and
implants were placed despite the deep pockets.
The inflammatory periodontal lesions had
recommendations the implants, i.e. FRIALIT-2 Synchro screws with a Cellplus surface
(Dentsply/Friadent, Mannheim, Germany), were placed palatally (Fig. 1).
Implant diameters were 4.5 mm for 12, 5.5 mm
for 11 and 4.5 mm for 22. Implant length was
15 mm throughout. All implants were anchored
in the cortical bone of the nasal floor (Fig. 2 ).
The implants were closely spaced in the bone with an inter-implant distance of no more than 1
to 1.5 mm. Implants with a smaller diameter did not achieve primary stability and had to be
replaced by larger ones. Alternatively, the periodontal lesions could have been curetted to the
point of healing. However, this would have caused substantial resorption of the mucosa and
the alveolar process. Despite a pocket depth of 11 mm around 21, 9 mm around 12 and 9 mm
around 22, the implants were seated down to the limbus. As tissue contouring abutments of
adequate length to support the mucosa together with the papillae to the level of the
mucogingival junction were not available, ProTect abutments were customized to the right
size. All implants achieved primary stability.
On the day of implant placement impressions were taken and the lab technician fabricated
plastic-coated, highly polished tissue contouring abutments matching the ovoid diameters of
the teeth. While he was at work, transfer copings were attached for 1 to 2 hours to maintain
stable mucosal conditions and prevent mucosal collapse.

 When ready, the customized tissue contouring abutments were put in place, the Maryland
bridge was bonded with Panavia® (Kuraray Dent) and antibiotics were administered.
The customized tissue contouring abutments were checked for stability at weekly intervals
and the mucosa was examined for alterations, shape and color. As the small inter-implant
distances prevented papilla regeneration, the original tissue contouring abutments were
replaced by other customized highly polished, plastic-veneered abutments with the diameters
reduced by platform switching. With these, papilla-like soft tissue developed within the
mucosa and persisted to the time of definitive management. Platform switching was also used
for the definitive restoration, i.e. the 4.5 mm implant in 12 was fitted with a 3.8mmD
abutment and the 5.5 mm implant in 11 with a 4.5 mmD abutment. Both of these abutments
were custom-designed. By the time of definitive management, the mucogingival junction was
only slightly lower than around the natural tooth 21. The 3 implant-supported electroplated
crowns were mounted on customized final abutments and retained with a horizontal screw.
An electroplated crown was also used on 21 to avoid a translucency mismatch.
At the follow-up visits scheduled at regular
intervals in the subsequent 2 years, the
vestibular probing depths dropped to 7 mm
around 12, 8 mm around 11 and 6 mm around
22. Compared to 21, which was vital, the
reduction of the mucogingival junction was
negligible. The papillae between the implant-
1. (b) Immediate implants with definitive crowns
This patient, a 38-years-old female, presented
with a root canalled, loosened (grade 2) 22.
significantly abnormal. After duly considering
all alternative treatments the patient opted for
definitive crown. 22 was extracted in local
When ready, the customized tissue contouring abutments were put in place, the Maryland
bridge was bonded with Panavia® (Kuraray Dent) and antibiotics were administered.
The customized tissue contouring abutments were checked for stability at weekly intervals
and the mucosa was examined for alterations, shape and color. As the small inter-implant
distances prevented papilla regeneration, the original tissue contouring abutments were
replaced by other customized highly polished, plastic-veneered abutments with the diameters
reduced by platform switching. With these, papilla-like soft tissue developed within the
mucosa and persisted to the time of definitive management. Platform switching was also used
for the definitive restoration, i.e. the 4.5 mm implant in 12 was fitted with a 3.8mmD
abutment and the 5.5 mm implant in 11 with a 4.5 mmD abutment. Both of these abutments
were custom-designed. By the time of definitive management, the mucogingival junction was
only slightly lower than around the natural tooth 21. The 3 implant-supported electroplated
crowns were mounted on customized final abutments and retained with a horizontal screw.
An electroplated crown was also used on 21 to avoid a translucency mismatch.
At the follow-up visits scheduled at regular
intervals in the subsequent 2 years, the
vestibular probing depths dropped to 7 mm
around 12, 8 mm around 11 and 6 mm around
22. Compared to 21, which was vital, the
reduction of the mucogingival junction was
negligible. The papillae between the implant-
1. (b) Immediate implants with definitive crowns
This patient, a 38-years-old female, presented
with a root canalled, loosened (grade 2) 22.
significantly abnormal. After duly considering
all alternative treatments the patient opted for
definitive crown. 22 was extracted in local

 anesthesia. For implant placement Schulte´s
recommendations for tooth extraction, implant
inclination and positioning to support the facial
cortical plate were followed. Immediately after
(Dentsply/Friadent, Mannheim, Germany) with
a grit-blasted acid-etched surface, a diameter of
4.5 mm and a length of 15 mm was placed, an
impression was taken, a tissue contouring abutment was mounted on the implant and the
patient was sent home for the day (Figs. 4-5).
In the meantime, the lab technician fabricated a horizontally screw-retained electroplated
crown, which was veneered with ceramic. Rather than glaze-baked, the crown surface was
polished mechanically to leave some scope for subsequent esthetic and functional crown
finishing, i.e. baking the ceramic on metal, which increases the compressive force applied to
the papilla and promotes papilla repair.
In the evening of the same day, the horizontally screw-retained electroplated crown matched
in shape to 22 was mounted. The mucosa had meanwhile been stabilized by the tissue
contouring abutment. On account of the compressive force generated by the permanent crown
the supracoronal tissue briefly became anemic. The anemic reaction ought to subside within 8
to 10 minutes. If it does not, the compromised nutritive supply of the soft tissue is bound to
Crown contacts were avoided during maximal intercuspidation, protrusion and lateral shift.
The patient was recalled weekly and instructed to clean the tooth gently and not to bite or
chew with it. The crown was checked for stability throughout the healing time of the implant.
It was never taken off. The mucosa was sound without any loss in height or papillary volume.
After about 3 months, the crown was removed
and finalized esthetically and functionally in
mucosa was at the same level as that around
the neighboring teeth. The distances of the
anesthesia. For implant placement Schulte´s
recommendations for tooth extraction, implant
inclination and positioning to support the facial
cortical plate were followed. Immediately after
(Dentsply/Friadent, Mannheim, Germany) with
a grit-blasted acid-etched surface, a diameter of
4.5 mm and a length of 15 mm was placed, an
impression was taken, a tissue contouring abutment was mounted on the implant and the
patient was sent home for the day (Figs. 4-5).
In the meantime, the lab technician fabricated a horizontally screw-retained electroplated
crown, which was veneered with ceramic. Rather than glaze-baked, the crown surface was
polished mechanically to leave some scope for subsequent esthetic and functional crown
finishing, i.e. baking the ceramic on metal, which increases the compressive force applied to
the papilla and promotes papilla repair.
In the evening of the same day, the horizontally screw-retained electroplated crown matched
in shape to 22 was mounted. The mucosa had meanwhile been stabilized by the tissue
contouring abutment. On account of the compressive force generated by the permanent crown
the supracoronal tissue briefly became anemic. The anemic reaction ought to subside within 8
to 10 minutes. If it does not, the compromised nutritive supply of the soft tissue is bound to
Crown contacts were avoided during maximal intercuspidation, protrusion and lateral shift.
The patient was recalled weekly and instructed to clean the tooth gently and not to bite or
chew with it. The crown was checked for stability throughout the healing time of the implant.
It was never taken off. The mucosa was sound without any loss in height or papillary volume.
After about 3 months, the crown was removed
and finalized esthetically and functionally in
mucosa was at the same level as that around
the neighboring teeth. The distances of the

 papilla from the contact points, the incisal edge and the implant base were also unchanged.
All of the soft tissue had successfully been preserved (Fig. 6):
2. (a) Delayed immediate implants with immediate impression taking and insertion of the
This 34-years-old female, who had lost 22 and was provided with a removable temporary
partial, came for implant treatment. The tooth had been extracted elsewhere about 8 weeks
ago. Even during this short interval, substantial hard and soft tissue loss had occurred by
clinical evidence. The patient reported that the extraction had been very difficult and that she
Treatment alternatives were discussed with her
and implant-supported restoration combined
The neighboring teeth were caries-free. The
alveolar process was exposed through a palatal
incision in local anesthesia. The bone atrophy,
which had already been noted on palpation, was confirmed intra-operatively (Fig. 7).
indicated the need for an implant with a
diameter of 3.8 mm and a length of 15 mm. A
blasted and acid-etched surface was chosen.
The bone from the intended implant site was
removed with a trephine. Implant placement
itself was uneventful. One third of the implant
surface was not buried in the host bone.
prosthodontic work, an impression was taken
papilla from the contact points, the incisal edge and the implant base were also unchanged.
All of the soft tissue had successfully been preserved (Fig. 6):
2. (a) Delayed immediate implants with immediate impression taking and insertion of the
This 34-years-old female, who had lost 22 and was provided with a removable temporary
partial, came for implant treatment. The tooth had been extracted elsewhere about 8 weeks
ago. Even during this short interval, substantial hard and soft tissue loss had occurred by
clinical evidence. The patient reported that the extraction had been very difficult and that she
Treatment alternatives were discussed with her
and implant-supported restoration combined
The neighboring teeth were caries-free. The
alveolar process was exposed through a palatal
incision in local anesthesia. The bone atrophy,
which had already been noted on palpation, was confirmed intra-operatively (Fig. 7).
indicated the need for an implant with a
diameter of 3.8 mm and a length of 15 mm. A
blasted and acid-etched surface was chosen.
The bone from the intended implant site was
removed with a trephine. Implant placement
itself was uneventful. One third of the implant
surface was not buried in the host bone.
prosthodontic work, an impression was taken

 immediately after implant placement. This left the lab technician more than 3 months´ time
for fabricating the crown. After impression taking the area of bone loss was grafted with bone
harvested from the retromolar region and with bone chips from the bone collector and the
trephine. The graft was covered with a titanium mesh secured with screws before primary
Healing was uneventful and the implant was uncovered after about 3 months. The titanium
mesh was removed through the original incision. The quality of the alveolar process had
substantially improved. The originally exposed implant surface was now covered by bone.
The final abutment had a collar height of 0.5 mm and the crown, which had meanwhile been
fabricated in the lab, was immediately mounted and retained with a horizontal screw. With
interdental and inter-implant sutures in place, the wound was allowed to heal.
After about 4 weeks, the bland mucosa had
become attached to the implant. At 2 years
peri-implant mucosal conditions were stable
despite the loss of about 1 mm in mucosal
height compared to the neighboring tooth. The
This patient, a 34-years-old female, presented
with loosening of 11 and 12. (Fig. 10a) As
these teeth were not salvageable because of
periodontal abscesses, they were extracted and
the patient was temporized with a removable
partial. Implants were placed about 8 weeks
mucoperiosteal flap was raised through a
palatal incision spanning 11 and 12. Alveolar bone loss was apparent both vertically and
horizontally. Two FRIALIT-2 Synchro implants were placed, i.e. a 4.5 mmD in 12 and a 5.5
mmD in 11. Both implants were 15 mm long. They were not fully buried in bone, but left
exposed about 2 mm above the alveolar process for augmentation with a bone substitute. The
vertical 2-mm defect and the horizontal defect were grafted with BIO-OSS® (Geistlich,
Wohlhusen, Switzerland). The grafts were covered with a resorbable membrane (Vycryl,
Ethicon, Norderstedt, Germany), which was secured with the occlusal screws of the implants.
Following submucosal vestibuloplasty the wound was closed with tension-free sutures. The
patient was prescribed an anti-inflammatory (diclofenac) and an antibiotic (clindamycin) to
prevent swelling and infection. Healing was uneventful. About 3 months later the implants
were uncovered through the original incision, tissue contouring abutments were mounted on
them and stabilized with inter-implant sutures. The mucoperiosteal flap was repositioned and
sutured against the abutments. For adequate mucosal support extra-high tissue contouring
abutments were chosen. Loading by the denture was not allowed for about 1 week. About 8
days later, an impression was taken and temporary crowns were inserted on the same day.
These were originally intended to be left in place for about 3 to 6 months for satisfactory soft
tissue contouring. However, the soft tissue support provided by the crowns was found to be
inadequate. As the patient spent some time abroad, she was prevented from showing up for
crown recontouring. As a result, definitive rehabilitation was done after about 1 year. The
inadequate soft tissue support had caused mucosal loss both vertically and horizontally.
Electroplated crowns retained with horizontal screws were chosen for definitive restoration.
The shoulder of the final abutments for the FRIALIT-2 implants was reduced to 0.5 mm for
recontouring the mucosa to match the natural ovoid crown shape. In addition, the abutments
were extended in length to counteract the leverage on the crowns. A small ischemic area just
above the crown margin was seen after the crowns were mounted. This disappeared within
approximately 8 to 10 minutes. Definitive management was completed by readjusting the
ceramic crowns to provide more support for the papillae and the soft tissue.
At about 2 years after crown insertion the soft tissue was stable. (Fig. 10b)
Gomez-Roman G, Schulte W., d’Hoedt B, et al. The Frialit-2 Implant System: Five-
year clinical experience in single-tooth and immediately postextractions applications.
Int. J Oral Maxl/ofac Implants. 1997; 12:299:309
Wöhrle PS. Single-tooth replacement in the esthetic zone with immediate
provisionalization: fourteen consecutive case report. Pract Periodont Aesth Dent.
Romanos G., Sofortbelastung von enossalen Implantaten im Seitenzahnbereich des
Unterkiefers, Tierexperimentelle und klinische Studien, Quintessenz Verlags GmbH
Tarnow DP, Magne AW, Fletcher P: The effect from the distance front the contact
point to the crest of one on the presence or absence of interproximal dental papilla. J
Saadoun AP, Le Gall MG: Periodontal implications in implant treatment planning for
aesthetic results. Pract Periodontics Aethest Dent 655-664, 1998.
Tarnow DP, Cho SC, Wallace S: The effect of inter-implant distance on the height of
inter-implant hone crest. J Periodontol 71(4):546-549, 2000
Hartmann, H-J. Sofortimplantation mit Sofortbelastung, Identity 5, 2004, 14-16,
Hartmann, H.-J., Ästhetische Frontversorgung mit sofortbelasteten Implantaten, DZW,
Lazzara RJ, Immediate Implant placement into extraction sites: surigal and restorative
advantages, Int J Periodontics Restorative Dent. 1989; 9(5): 332-43.
immediately after implant placement. This left the lab technician more than 3 months´ time
for fabricating the crown. After impression taking the area of bone loss was grafted with bone
harvested from the retromolar region and with bone chips from the bone collector and the
trephine. The graft was covered with a titanium mesh secured with screws before primary
Healing was uneventful and the implant was uncovered after about 3 months. The titanium
mesh was removed through the original incision. The quality of the alveolar process had
substantially improved. The originally exposed implant surface was now covered by bone.
The final abutment had a collar height of 0.5 mm and the crown, which had meanwhile been
fabricated in the lab, was immediately mounted and retained with a horizontal screw. With
interdental and inter-implant sutures in place, the wound was allowed to heal.
After about 4 weeks, the bland mucosa had
become attached to the implant. At 2 years
peri-implant mucosal conditions were stable
despite the loss of about 1 mm in mucosal
height compared to the neighboring tooth. The
This patient, a 34-years-old female, presented
with loosening of 11 and 12. (Fig. 10a) As
these teeth were not salvageable because of
periodontal abscesses, they were extracted and
the patient was temporized with a removable
partial. Implants were placed about 8 weeks
mucoperiosteal flap was raised through a
palatal incision spanning 11 and 12. Alveolar bone loss was apparent both vertically and
horizontally. Two FRIALIT-2 Synchro implants were placed, i.e. a 4.5 mmD in 12 and a 5.5
mmD in 11. Both implants were 15 mm long. They were not fully buried in bone, but left
exposed about 2 mm above the alveolar process for augmentation with a bone substitute. The
vertical 2-mm defect and the horizontal defect were grafted with BIO-OSS® (Geistlich,
Wohlhusen, Switzerland). The grafts were covered with a resorbable membrane (Vycryl,
Ethicon, Norderstedt, Germany), which was secured with the occlusal screws of the implants.
Following submucosal vestibuloplasty the wound was closed with tension-free sutures. The
patient was prescribed an anti-inflammatory (diclofenac) and an antibiotic (clindamycin) to
prevent swelling and infection. Healing was uneventful. About 3 months later the implants
were uncovered through the original incision, tissue contouring abutments were mounted on
them and stabilized with inter-implant sutures. The mucoperiosteal flap was repositioned and
sutured against the abutments. For adequate mucosal support extra-high tissue contouring
abutments were chosen. Loading by the denture was not allowed for about 1 week. About 8
days later, an impression was taken and temporary crowns were inserted on the same day.
These were originally intended to be left in place for about 3 to 6 months for satisfactory soft
tissue contouring. However, the soft tissue support provided by the crowns was found to be
inadequate. As the patient spent some time abroad, she was prevented from showing up for
crown recontouring. As a result, definitive rehabilitation was done after about 1 year. The
inadequate soft tissue support had caused mucosal loss both vertically and horizontally.
Electroplated crowns retained with horizontal screws were chosen for definitive restoration.
The shoulder of the final abutments for the FRIALIT-2 implants was reduced to 0.5 mm for
recontouring the mucosa to match the natural ovoid crown shape. In addition, the abutments
were extended in length to counteract the leverage on the crowns. A small ischemic area just
above the crown margin was seen after the crowns were mounted. This disappeared within
approximately 8 to 10 minutes. Definitive management was completed by readjusting the
ceramic crowns to provide more support for the papillae and the soft tissue.
At about 2 years after crown insertion the soft tissue was stable. (Fig. 10b)
Gomez-Roman G, Schulte W., d’Hoedt B, et al. The Frialit-2 Implant System: Five-
year clinical experience in single-tooth and immediately postextractions applications.
Int. J Oral Maxl/ofac Implants. 1997; 12:299:309
Wöhrle PS. Single-tooth replacement in the esthetic zone with immediate
provisionalization: fourteen consecutive case report. Pract Periodont Aesth Dent.
Romanos G., Sofortbelastung von enossalen Implantaten im Seitenzahnbereich des
Unterkiefers, Tierexperimentelle und klinische Studien, Quintessenz Verlags GmbH
Tarnow DP, Magne AW, Fletcher P: The effect from the distance front the contact
point to the crest of one on the presence or absence of interproximal dental papilla. J
Saadoun AP, Le Gall MG: Periodontal implications in implant treatment planning for
aesthetic results. Pract Periodontics Aethest Dent 655-664, 1998.
Tarnow DP, Cho SC, Wallace S: The effect of inter-implant distance on the height of
inter-implant hone crest. J Periodontol 71(4):546-549, 2000
Hartmann, H-J. Sofortimplantation mit Sofortbelastung, Identity 5, 2004, 14-16,
Hartmann, H.-J., Ästhetische Frontversorgung mit sofortbelasteten Implantaten, DZW,
Lazzara RJ, Immediate Implant placement into extraction sites: surigal and restorative
advantages, Int J Periodontics Restorative Dent. 1989; 9(5): 332-43.