Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Adhd: the tip of the iceberg
ADHD: The Tip of the Problems and Summary This chapter can serve as a review for the reader, and can be reproduced for personal use by family members or teachers. Figure 1. The extended spectrum of problems experienced by people with ADHD. The classically discussed symptoms of ADHD are only the tip of the iceberg. We’ve Been Missing the Point “Johnny is very active! He never stops moving. He gets distracted by any little noise, and has the attention span of a flea. Often, he acts before he thinks. His sister, Jill, is often in a fog. Sometimes, she’s just so spaced!”
That is how we typically consider children with Attention Deficit Hyperactivity Disorder (ADHD). OK, not so bad. But that is often only the tip of the iceberg. Here is another likely description of the whole picture for a child with ADHD:
“I can’t take it any more!! We scream all morning to get out of the house. Homework takes hours. If I don’t help him with his work, he’s so disorganized that he’ll never do well. If I do help him, he screams at me. Since he never finishes anything, everyone thinks he doesn’t care. No matter how much we beg or punish, he keeps doing the same stupid things over and over again. He never considers the consequences of his actions, and doesn’t seem to care if they hurt me. It’s so easy for him to get overwhelmed. Sometimes, he just wants to ‘turn the noise off.’ He is so inflexible, and then blows up over anything. It gets me so angry that I scream back, which makes everything even worse. Now that he’s getting older, the lies and the cursing is getting worse, too. I know he has trouble paying attention, but why does he have all of these other problems as well?”
It is not a coincidence that children with ADHD often manifest so much more than the classic triad of inattention, impulsivity, and hyperactivity. When we focus merely on these typically defined symptoms, we fail to deal with the whole vista of difficult problems experienced by patients and their families. This spectrum includes a wide range of “executive dysfunction” (such as poor self-control and foresight), additional co-morbid disorders (such as anxiety, depression or conduct disorders), and family stresses. These are summarized in Figure 1.
Redefining ADHD as “Executive Dysfunction”
ADHD needs to be redefined to include a wide range of “executive dysfunction.” As Russell Barkley explains (see Resources), this dysfunction stems from an inability to inhibit behavior so that demands for the future can be met. In other words, people with ADHD are so drawn to the present that the future does not even “show up on their radar screen.” There is no future or past; only “NOW.”
So, what are Executive Functions?
When you step on a snake, it bites. No verbal discussion occurs within the snake’s brain. No recall of whether striking back worked in the past. No thought as to where this action will lead to in the future. No inhibition. Stepped on. Bite back. Humans, fortunately, have the option to modulate their behavior.
No single part of the human brain is solely in charge of this modulation. It does appear, however, that our frontal and pre-frontal lobes function largely as our “Chief Executive Officer (CEO).” Orchestrating language and memory functions from other parts of the brain, these frontal centers consider where we came from, where we want to go--and how to control ourselves in order to get there.
Most importantly, the ability to inhibit (“putting on the brakes”) is central to effective executive function. Successful execution of a plan largely involves putting brakes on distracting activities. These brakes--courtesy of our pre-frontal inhibitory centers--allow us the luxury of time during which we can consider our options before reacting.
This lack of inhibition is a double problem for people with ADHD. First, without these brakes, they will be viewed as unable to adequately inhibit distractions, inhibit impulsive reactions, or inhibit physically acting upon these stimuli (hyperactivity). Second, patients with ADHD do not inhibit their behavior long enough for the other executive functions below to adequately develop either. Executive functions identified by Barkley include:
Self-talk refers to the ability to talk to ourselves--a mechanism by which we work through our choices using words. Toddlers can be heard using self-talk out loud. Eventually, this ability becomes internalized and automatic. However, ADHD patients have not inhibited their reactions long enough for this skill to fully develop. Working memory refers to those ideas that we can keep active in our minds at a given moment. For example, in order to learn from mistakes, you have to be able to juggle not just the present situation, but also keep in mind past times when certain strategies did or did not work. Working memory hopefully also includes keeping future goals in mind (such as remembering that we want to get into a good college, not just do the most intriguing activity currently available). Without the ability to inhibit, people with ADHD never get to develop good function of their working memory. Foresight (predicting and planning for the future) will be deficient when inadequate working memory teams up with a poor ability to inhibit the present distractions. People with ADHD cannot keep the future in mind. They are prisoners of the present; the future catches them off guard. In fact, surprisingly poor foresight is perhaps the greatest difficulty in their lives. Sense of time is an executive function that is usually extremely poor in ADHD. Shifting from Agenda A to Agenda B is a difficult task requiring good executive function. Pulling yourself out of one activity and switching to another--transitioning--is innately difficult, and requires effort and control. Separating emotion from fact requires time to reflect. Each event has an objective reality, and an additional “emotional tag” which we attach to it. For example, a traffic jam may occur, causing us to be late for work. That is the objective fact. How we react, though, is up to the emotional tag of significance that we place on it. Do we stay calm, and make plans to finish up a little later. Or, do our emotions cause us to see the traffic as a personal, unfair attack--causing us to seethe and curse. Without the gift of time, we never get to separate emotion from fact. This leads to poor ability to judge the significance of what is happening to us.
In short, then, the ability to modulate behavior comes largely from our pre-frontal lobes, which function primarily as inhibitory centers. Without the luxury of inhibitory brakes, ADHD patients do not get to fully utilize any of their frontal lobe “executive functions.”
What are the different kinds of problems in ADHD?
Redefining ADHD as inadequate inhibition explains a wide spectrum of difficulties experienced by people with the syndrome. This expanded spectrum of symptoms can create an environment of havoc. For more details, see the important works by Barkley, Greene, and Silver listed below under Resources.
1. Symptoms of Executive Dysfunction a. Classical Symptoms of ADHD
ADHD is typically defined as a triad of inattention, impulsivity, and hyperactivity. Figure 2 is a simplified version of the DSM-IV criteria for ADHD. These are the symptoms that receive the most attention from doctors, and all come from an inability to inhibit.
• Distractible <=Inadequate inhibition of extraneous stimuli.
• Impulsive <=Inadequate inhibition of internal stimuli.
• Hyperactive <=Physically checking out those stimuli.
b. Other Symptoms of Executive Dysfunction
If we do not address the following additional executive function issues, we are only dealing with a small part of the problem. These are not just “incidental” symptoms. They are hard to live with—ask either the patient or his family.
• Lack of foresight!!! (“Johnny, you’ll never get into a good college if you all
you do is play videogames. Why do you keep shooting yourself in the foot?”) Foresight--the ability to predict the results of our behaviors--is a major adaptive ability of humans. We can run imaginary simulations of the future on our brain’s computer. Lack of use of this ability can be the most devastating part of ADHD. Mothers--often endowed with great foresight-- are crushed as they watch their child repeatedly head down counter-productive paths.
• Poor hindsight/Trouble learning from mistakes (“Johnny, how many times
do you have to be punished for the same thing.”) Unable to inhibit the present, Johnny cannot stop to consider lessons from the past.
• Live at the “mercy of the moment.” (“Johnny is always swept away by whatever is happening to him right then and there.”) ADHD behaviors make sense once we realize that they are based on reactions taking only the present moment into account. It is not that Johnny doesn’t care about the future; it is that the future and the past don’t even exist. Such is the nature of the disability. By way of analogy, imagine riding down a river with a leaking canoe. You would be so overwhelmed by the need to bail out water that you would not see the upcoming cliff. It's not that you don't "care" about falling over a cliff--it's that you don't even get to consider it.
• Life in the next 4 seconds. If you want to make sense out of inexplicable behaviors by someone with ADHD, just ask yourself: “What behavior makes sense if you only had 4 seconds left to live?” For example, if you only had 4 seconds to live, it would make sense to lie in order to expediently get out of a problem…After all, who cares about a future reputation when there is no future?!”
• Poor organization (“Johnny, you never told me that there is a paper due
tomorrow! And, why do we have to fight over getting out of the house every morning!”)
• Trouble returning to task (“Johnny, you never complete anything. You just
• Poor sense of time (“Johnny, what have you been doing all afternoon? You
can’t spend one hour on the first paragraph!”)
• Time moves too slowly (“Mommy, you are taking forever to go shopping!”)
• Poor ability to utilize “self-talk” to work through a problem (“Johnny, what
were you thinking?! Did you ever think this through?”)
• Poor sense of self awareness (Johnny’s true answer to the above question is
probably “I don’t have a clue. I guess I wasn’t actually thinking.”)
• Poor internalization and generalization of rules (“Johnny, why do I need to
keep reminding you that playing videogames comes after you finish your homework.)
• Poor reading of social clues (“Johnny, you’re such a social klutz. Can’t you
see that the other children think that’s weird.”)
• Inconsistent work and behavior. (“Johnny, if you could do it well yesterday,
why is today so horrible.) With 100% of their energy, they may be able to control the task that most of us can do with 50% of our focus. But who can continually muster 100% effort? As the joke goes: ADHD children do something right once, and we hold it against them for the rest of their lives.
• Trouble with transitions (“Johnny, why do you curse at me when I’m just
• Hyper-focused at times (“When Johnny is on the computer, I can’t get him
off. And once his father gets his mind on something, off he goes!”)
• Poor frustration tolerance (“Johnny, why can’t you even let me help you get
• Frequently overwhelmed (“Mommy, just stop. I can’t stand it. Just stop.
• Gets angry frequently and quickly (“Johnny, you get flooded with emotion so
quickly. Why are you always angry with me? Even though you usually apologize, it still hurts me.”)
• Push away those whose help they need the most (“Mommy, stop checking my
• “Hyper-responsiveness” (“Mommy, you know I hate sprinkles on my
donuts! You never do anything for me! I hate you!”) Barkley uses the term hyper-responsiveness to indicate that people with ADHD have excessive emotions. Their responses, however, are appropriate to what they are actually feeling. So next time you see someone “over-reacting,” realize that they are actually “over-feeling,” and must feel really awful at that moment.
• Inflexible/explosive reactions (“Johnny, you’re stuck on this. No, I can’t just
leave you alone. Johnny, now you’re incoherent. Johnny, just stay away. I can’t stand it when you break things!”) Greene (see Resources) goes into extensive explanation about the inflexible/explosive child.
• Feels calm only when in motion (“He always seems happiest when he is
busy. Is that why he stays at work so late?”)
• Thrill seeking behavior (“He seems to crave stimulation at any cost. In fact,
he feels most ‘on top of his game’ during an emergency.”)
• Trouble paying attention to others (“My husband never seems to listen when
I talk to him. He just cannot tolerate sitting around with me and the kids. He doesn’t “pay attention” to his family any more than he “paid attention” in school.”) As the patient gets older, people in his life will increasingly expect more time and empathy to be directed their way. Yet, the behaviors above of ADHDers may interfere with their demonstration of these traits, despite their passions.
• Trouble with mutual exchange of favors with friends. Without establishing a
reliable “bank account” of kept promises, friendships can be hard to make.
• Sense of failure to achieve goals (“Somehow, I never accomplished all that I
thought I could or should have.”) This deep disappointment is commonly what brings adults with ADHD to seek help.
• Lying, cursing, stealing, and blaming others become frequent components of
ADHD; especially as the child gets older. According to some particularly depressing data by Russell Barkley, here is how ADHD children compare to typical children:
ADHD Children (%) Typical Children (%)
[Barkley RA, Fischer M, et al. The Adolescent outcome: An 8-year prospective follow up. Journal of the American Academy of Child and Adolescent Psychiatry, 29, 546-557.]
• In short, the symptoms of ADHD become less “cute” as the children switch
from elementary to secondary schools. The “good” news comes from understanding that these problems are commonly part of the syndrome we call ADHD. They are nobody’s fault--not yours, and not your child’s. This understanding points the way towards coping with these issues.
2. Co-Morbid Disorders Associated with ADHD
In addition to the executive dysfunctions above, there are a myriad of co-morbid disorders which frequently accompany the diagnosis of ADHD in the patient and/or her family. These disorders may often be misdiagnosed as ADHD, or they may co-existwith true ADHD. In addition, many people are “subsyndromal,” and have just parts of the following diagnosis. John Ratey (see Resources) refers to these as “shadow syndromes.” The presence of these disorders must be investigated whenever the diagnosis of ADHD is being considered.[Medications for the co-morbid disorders in children are used frequently “off-label,” and information is quite limited. Recommendations need to be taken as subject to change and debate. Full discussion of the usefulness, monitoring, drug interactions, etc. of these medications is beyond this paper. The reader is referred to ADHD with Comorbid Disorders by Pliszka (see Resources), which forms the basis of the following medical recommendations. Medical treatment of the associated disorders is perhaps best done in consultation with a neurologist or psychiatrist.]a. Learning Disabilities (LD)
Twenty to thirty percent of patients with ADHD have LD. A review of the diagnostic
criteria for ADHD (figure 2) will show that an Organizational Disability is virtually built into the syndrome of ADHD by definition. Following directions, sequencing problems and dysgraphia are also particularly common. Learning disabilities should be suspected whenever a student does not “live up to his/her potential.” They are identified with history, exam and psycho-educational testing. As well explained by Larry Silver (see Resources), learning disabilities can either exacerbate or mimic ADHD. After all, how long can someone focus on something that she does not understand?
b. Disruptive Behavioral Disorders
50% of ADHD children have Disruptive Behavioral Disorders. Even in the absence of a
full diagnosis, the lives of many (if not most) children with ADHD are afflicted by lying, cursing, taking things that do not belong to them, blaming others, and being easily angered.This frequency is not surprising given the executive dysfunction hypothesis. Full definitions can be found in the Diagnostic and Statistical Manual-IV. Medications such as mood stabilizers (eg. Depakote), Catapress, and Risperdal can sometimes help with impulsivity and aggression.
• Oppositional Defiant Disorder (ODD). Whereas ADHD children do not
comply because of inattention or impulsivity, ODD children are unwilling to conform (even with an intriguing task). They may be negative, deliberately annoying or argumentative, angry and spiteful.
• Conduct Disorder (CD). Children with CD are more frequently overtly
hostile and law breaking, with lack of remorse, not seen in ADHD alone. These people violate the rights of others, such as with physical cruelty to others or animals, stealing, etc.
• Antisocial Personality Disorder. People with Antisocial Personality
Disorder have a pervasive pattern of severe violation of the rights of others, typically severe enough to merit arrest.
c. Anxiety Disorder
Anxiety Disorder occurs in up to 30% of children with ADHD, but half of the children
never tell their parents! Patients are beset most days by painful worries not due to any imminent stressor. Children may appear edgy, stressed out, tense, or sleepless. There may be panic attacks or an incomplete (or negative) response to stimulants.
• Change of environment; behavioral approaches; exercise; meditation.
• buspirone (Buspar)—helps anxiety but not panic attacks.
• Tricyclics—helps some with anxiety; great for panic attacks.
• Stimulants may help if anxiety is a secondary problem, but may also worsen
d. Obsessive Compulsive Disorder (OCD)
Obsessive thoughts and compulsive actions may occur in up to one third of ADHD
patients. If ADHD is living in the present, then OCD is living in the future. Although difficult to live with, the future goal directed behavior of OCD may help overcome the organizational problems of ADHD. SSRI’s are the current mainstay of medical treatment.
e. Major Depression
Depression occurs in 10-30% of ADHD children and in 47% of ADHD adults. Although
pure ADHD patients get depressed briefly, they flow with the environment (changing within minutes). In contrast, depressed children stay depressed for long periods. The symptoms include loss of joy, sadness, pervasive irritability (not just response to specific frustrations), withdrawal, self-critical outlook, and vegetative symptoms (abnormal sleep or appetite).
• Selective Serotonin Uptake Inhibitors (SSRIs) such as Luvox, Paxil, Prozac,
• bupropion (Wellbutrin)—helps depression and ADHD.
• venlafaxine (Effexor)—helps depression and maybe ADHD.
• Tricyclics (Tofranil, Pamelor) do not appear to work in children for
f. Bipolar Depression
Bipolar depression occurs in up to 20% of ADHD children. These children show
depression cycling with abnormally elevated, expansive, grandiose, and pressured moods. Children may cycle within hours. Other hallmarks include severe separation anxiety and often precociousness as children; extreme irritability; extreme rages that last for hours; very goal directed behavior; and little sleep requirement. They may demonstrate hypersexuality; gory dreams; extreme fear of death; extreme sensitivity to stimuli; often oppositional or obsessive traits; heat intolerance; craving for sweets; bedwetting; hallucinations; possible suicidal tendencies or substance abuse. Often symptoms are shown only at home. See The Bipolar Child by Papolos (under Resources). Also see the articl
Consider bipolar when a diagnosis of “ADHD” is accompanied by above symptoms or:
• strong family history of bipolar disorder or substance abuse.
• prolonged temper tantrums and mood swings. Sometimes the angry,
violent, sadistic, and disorganized outbursts last for hours (vs. less then 30 minutes in ADHD).
• bipolar rages are typically from parental limit setting; in ADHD, rages are
• explosive and “intentionally” aggressive or risk seeking behavior.
• separation anxiety, bad dreams, disturbed sleep; or fascination with gore.
• morning irritability which lasts hours (vs. minutes in ADHD).
• carbamazepine (Tegretol) clearly helps bipolar and aggressive symptoms
at least in adults (no controlled studies in children).
• lithium (not clear that it works in children who cycle so rapidly; does not
• Plus cautious use of stimulants or antidepressants for ADHD symptoms.
• Stimulants and antidepressants may trigger mania.
• Plus risperidone for psychotic symptoms and aggression.
g. Tics and Tourette’s (motor & vocal tics, ADHD, OCD, LD)
Seven percent of ADHD children have tics; but 60% of Tourette’s patients have ADHD.
• clonidine (Catapress) / guanfacine (Tenex)—help impulsivity & tics.
• bupropion —helps ADHD but might worsen tics.
• stimulants—helps ADHD but often worsen (or improve) tics.
• tricyclics—mild ADHD help but tic “neutral.” Cardiac concerns.
h. Asperger’s Syndrome
ADHD and Asperger’s syndrome can cluster together. Symptoms include impaired
ability to utilize social cues such as body language, irony, or other “subtext” of communication; restricted eye contact and socialization; limited range of encyclopedic interests; perseverative, odd behaviors; didactic, monotone voice; “concrete” thinking; over-sensitivity to certain stimuli; and unusual movements.
i. Sensory Integration (SI) Dysfunction
SI dysfunction is the inability to process information received through the senses. The
child may be either oversensitive or undersensitive to stimuli. Or, the child may not be able to execute a coordinated response to the stimuli. SI may mimic or co-exist with ADHD. SI is typically evaluated by an occupational therapist. See Kranowitz’s book (Resources). Some types of SI include:
• Hypersensitive to touch: sensitive to clothes or getting dirty; withdraw to
• Hyposensitive to touch: wallow in mud; rub against things; unaware of pain.
• Hypersensitive to movement: avoid running, climbing, or swinging.
• Hyposensitive to movement: rocking; twirling; unusual positions.
• May also respond abnormally to sights, sounds, smells, tastes or textures.
• May be clumsy; have trouble coordinating (bilateral) movements; or have
3. Familial Issues. a. Family members with their own neuro-psychiatric problems
Family members may have their own ADHD, OCD, depression, anxiety, etc. In fact, a
child with ADHD has a forty percent chance that one of his parents have ADHD. Such difficulties affect the family’s ability to cope with the ADHD child, and may need to be addressed independently.
b. Stress--created by the child--cycling back to further challenge the patient.
Children or adults with ADHD can create chaos throughout the entire family, stressing
everyone in the process. The morning routine and homework are frequent (and lengthy!) sources of dissension. Other siblings are often resentful of the time and special treatment given to the ADHD child. Mothers, who frequently consider their child’s homework to be their own, find it stressful that “their” homework never seems to get completed. Fathers come home to discover a family in distress, and that they are expected to deal not only with a child who is out of control, but also with the mother who is understandably now losing it, too. Parents may argue over the “best strategy,” a difficult problem since no strategies are even close to perfect. The unpleasantness of life around someone with ADHD leads to a pattern of avoidance which only furthers the cycle of anger. In turn, all of this family turmoil creates a new source of pressures and problems for the already stressed ADHD patient to deal with.Non-Medical Treatments for ADHD
First, we need to identify and treat any of the above symptoms. We need to recognize that “ADHD” is short-hand for this entire biologically based spectrum. Otherwise, parents will think that they have a child with ADHD who just also happens to be difficult and/or appear mean spirited.
Non-medical treatment usually requires academic and organizational support. Learning disabilities need to be identified and treated. Computers can help with handwriting and spelling difficulties, graph paper can help with the spacing of math problems, and clip-art can help with art projects. Organizational support includes close supervision of all tasks by parents; checking assignment pads by teachers; small, structured settings; one to one attention when possible; good eye contact; having the child repeat directions ;and possibly two sets of school books (one for school, one for home).
Behavioral reward approaches can also ameliorate symptoms. Children with ADHD are like moths: they are drawn to the brightest light. Unfortunately, sometimes the brightest light is a bug zapper. Our goal is to make sure that the brightest light is a productive one. If the light is bright enough, they will go there. It is fortunate--but not an accident--that children with ADHD can be easily enticed by quick rewards. Afterall, they are creatures of the moment. No doubt, it would be better if the children were adequately motivated by their own internal “high ideals.” But for those ADHD children who do not see how doing thirty math problems right now will lead to a better world, external rewards may be needed.
Reward systems rely on children's natural desire to please their parents. If a child's basic relationships with her parents are so full of anger and resentment that she no longer finds pride in pleasing her parents, then those basic relationships need some healing first, before behavioral modification programs are likely to be successful. Set aside a period of special time (up to 30 minutes) where the goal is simply to exist together pleasantly in the same room. The child gets to choose the (reasonable) activity, and the parent gets to
enjoy being near their child without provoking a world war. Avoid saying anything critical--even if it would be helpful. Keep questions and comments (even positive ones) to a minimal level. After all, interruptions are still annoying. The goal here is to put your account of good/bad interactions into a positive balance, making it more likely for the child to want to please you. That sets the stage for smoother discipline in the future. Dr. David Rabiner (s and Dr. Russell Barkley (see Resources) provide a full explanation of this technique.
Typical behavioral plans are token systems which motivate via strongly enticing rewards; and if needed, by punishments. Such programs are explained in detail by both Barkley and Silver (see Resources). Barkley’s guiding principles for behavioral approaches include:
• Clearly defined and reviewed before difficulty arises
• Acted upon without extensive moralizing
• Recognition that the ADHD person has a disability.
• Do not personalize the ADHD person’s actions.
• Be forgiving to the child and yourself.
• Use tangible, physical methods to externalize problem areas.
• Explicitly state out loud the problem and consequences at the time of
• Use timers and planners to break down time into manageable,
• Brainstorm ideas on index cards or word processor. Then, physically
Just STOP!
Some people’s brains are too inflexible and explosive to respond consistently to such systems. This occurs more commonly in the pre-teen and teen years. Nothing good can come from a “discussion” held by out of control people. Once that fact is recognized, some families may be ready for Plan B: try to prevent incoherent “meltdowns” before they occur--by allowing a cooling off period at the first sign of their appearance. Sometimes this involves being coached or cajoled through the difficult situation. Other times, we need to be left alone to regain composure. Once cool heads prevail all around, calm discussion of the issue can productively ensue. An attitude of negotiation must prevail on all sides. Sometimes, we are better off just “picking our fights.” These approaches are empathically explained in Ross W. Greene’s excellent book, The Explosive Child.
In summary, STOP!!! Remember, the hallmark of ADHD is trouble stopping--trouble putting on the brakes. Thus, it is not surprising that the first step in dealing with ADHD is to STOP. You will notice that the sections on anger management, problem solving skills, and general behavior techniques all begin with the need to STOP. Only then does executive function to resurface. Typically, when calm and unthreatened, even the ADHD brain will make the correct choice. The need to first STOP applies to both the child and ourselves! See sections on Anger and Problem Solving.
In addition, regular exercise is also frequently reported as useful.
Medical Treatments for ADHD
When behavioral approaches are insufficient, medication is frequently warranted; and in fact, often gives the patient the tools to successfully follow behavioral plans. Medications for ADHD usually involve the stimulation of frontal lobe function. Specifically, they increase firing of noradrenergic pathways. Remember, the frontal lobes function primarily by way of inhibition. Thus, to use an analogy, stimulants “slow you down” by equipping the bicycle with adequate brakes. Importantly, they do not work by “gumming up the gears.” ADHD patients bump into less trouble because they are now a high performance bike capable of appropriate braking, not because they are too tired to get going. Stimulants allow putting on the brakes against distractions, impulsivity, over-reactions, and frustrations. They give the executive functions a fighting chance.
Stimulants
Stimulant medications are the mainstay of medical treatment for ADHD. No other class of medicine works as well or as safely. Many of the executive dysfunctions will improve, although other approaches may be needed if there are co-morbid symptoms.
Although usually well tolerated, the most common side effects are insomnia, loss of appetite, and rebound irritability. Precipitation of tics, headaches, abdominal distress, and other less common side effects can also occur.
• methylphenidate (Ritalin and Concerta)
• pemoline (Cylert) is rarely used now because of potential hepatotoxicity.
Non-Stimulants
• Novel antidepressant with dopamine agonist and noradrenergic
• May decrease hyperactivity and aggression and improve cognition.
• nortriptyline (Pamelor) or imipramine (Tofranil)
• Consider if stimulants are ineffective; or with co-morbid tics.
• Do not help any co-morbid depression in children.
• clonidine (Catapress) or guanfacine (Tenex)
• Centrally acting alpha-adrenergic agonists.
• Helps impulsivity/aggression and tics but less useful for attention.
• Controversy over apparent safety when used with stimulants.
• SSRIs (Luvox, Paxil, Prozac, and Zoloft)
• Anecdotal evidence in treatment of ADHD.
• Sometimes exacerbate symptoms (a process called “disinhibition”)
• Can be helpful with associated symptoms.
• Noradrenergic and serotinergic properties.
• Limited adult studies suggest effectiveness for ADHD.
• Useful with co-morbid Intermittent Explosive Disorder.
Top Principles
1. Keep a sense of humor. Seek to enjoy, not to scream.
2. Celebrate the ADHD person’s humor, creativity, and passion.
4. You do not have a standard child. You can view the issue as a disability. Or, you can
view it as wonderful uniqueness. Or, you can view it as both. The perspective of “standard,” though, is not an option. This "disability outlook" will help because it eliminates blame; sets reasonable expectations thereby minimizing anger; and points the way for parents/teachers to see themselves as "therapists" not victims.
5. Recognize that attention issues in the child are only the tip of the iceberg that the
6. The “patient” in ADHD is the whole family.
7. Remember that children with ADHD have two time frames: “Now,” and “Huh.”
There is no future. There is no past. There is only now.
8. Do you want to understand the ADHDers actions? Just ask yourself: “What
behavior would make sense if you only had 4 seconds to live?”
9. Instead of punishing wrong behavior, set a reward for the correct behavior you would
rather replace it with. Rewards should be immediate, frequent, powerful, clearly defined, and consistent.
10. Plan ahead. Give warnings before transitions. Discuss in advance what is expected.
Have the child repeat out loud the terms he just agreed to.
11. Don’t argue; nag; or attempt unsolicited and spontaneous transplants of your wisdom
to your child. Instead, either a) decide that the issue is aggravating but not significant enough to warrant intervention; or b) make an appointment with your child to discuss the issue.
12. Head off big fights before they begin. Seek to diffuse, not to inflame. When tempers
flare, allow everyone to cool off. Serious discussion can only occur during times of composure.
13. Especially with teens, negotiate, negotiate, and negotiate. Parents need to model
negotiation, not inflexibility. Don’t worry about losing control: the parent always gets to decide when negotiation is over and which compromise is accepted. Remember: negative behaviors usually occur because the ADHDer is spinning out of control, not because he is evil. While evil behavior would need to be aggressively squelched, the much more common overwhelmed behavior needs to calmly defused.
14. Pick your fights. Is the issue at hand worth chipping away at your relationship with
your child? Can your child really control the offending behavior at this moment?
15. Although it is not the child’s “fault,” he will still ultimately be the one to take the
17. You will make it through this; you have no choice.
18. “The children who need love the most will always ask for it in the most unloving
ways.” [Words of a teacher quoted by Russell Barkley.]
19. If it is working, keep doing it. If not, do something else.
20. Barkley implores you to forgive your child and yourself nightly. You didn’t ask to
live with the effects of ADHD any more than did your child.
21. Review this text, and others, periodically. You are going to forget this stuff, and
different principles will likely be needed at different stages. A good way to remember to review is by subscription to some of the free monthly newsletters on ADHD (see resources).
22. Steven Covey (The Seven Habits of Highly Effective People) suggests imagining
your child delivering your eulogy. What do you want him to say about you? Keep those bigger goals in mind as you choose your interactions/reactions to your child.
23. This is not a contest with your child. The winner is not the one with more points. The
winner is the one whose child still loves them when they graduate from high school.
Conclusion: “Doctor, Will it all be OK?”
In summary, we miss the point when we address only the triad of inattention, impulsivity, and hyperactivity. These symptoms are only the tip of the iceberg. Much greater problems have usually been plaguing the family, but often no-one has understood that the associated symptoms described above are part and parcel of the same neurologically based condition. Without this recognition, families have thought that their ADHD child also was “incidentally” uncooperative and apparently self-absorbed. Unless we recognize that these extended symptoms are part of the same spectrum, parents will not mention them; and doctors will never deal with them.
Given all of this, it is reasonable to ask: “Will this go away?” Personally, I would re-phrase the question as, “Will it be OK?” The answer can be “yes,” but we must recognize that this is often the “fifty year plan.” In other words, these children can be wonderfully successful adults, while they continue to work on these issues over their lifetime. Meanwhile, we “just” need to patiently steer them in the positive direction.
Finally, we must also keep in mind that some of the iceberg is fantastic and enviable. While the rest of us are obsessing about the future, or morosing about the past, people with ADHD are experiencing the present. ADHDers can be a lot of fun; dullness is never a problem. Their “Why not?” attitude may free them to take chances that the rest of us may be afraid to take. Their flux of ideas may lead to creative innovations. And most importantly, their extreme passion can be a source of inspiration and accomplishment to the benefit of us all.
Resources for ADHD
Accurate information, and selected links for other sites and books.
Leads patients to everything they need on all out-patient pediatric neurology.
CHADD (Children and Adults with Attention Deficit Disorders)
Excellent, all-inclusive support group with local chapters.
Taking Charge of ADHD; Russell Barkley; Guilford Press.
Particularly for associated behavioral, executive problems. Essential reading for understanding ADHD.
Dr. Larry Silver’s Advice to Parents with ADHD; Larry Silver; American Psychiatric Press, Inc.
Particularly for associated learning disabilities.
Resources for Co-morbid Diagnoses
ADHD with Comorbid Disorders; Steven Pliszka, Caryn Carlson, James Swanson; Guilford Press.
Encyclopedic review of the literature on drug and behavioral treatments.
Asperger’s Syndrome: A Guide for Parents and Professionals; Tony Attwood; Jessica Kingsley Pub.
Excellent diagnostic and treatment resource.
The Bipolar Child; Demitri Papolos; Broadway Books.
Excellent diagnostic and treatment resource.
The Explosive Child; Ross W. Greene; Harper Collins.
For inflexible-explosive children who do not respond well to typical reward systems.
The Out-of-Sync Child; Carol Stock Kranowitz; Skylight Press.
Diagnosis and treatment of Sensory Integration disorders.
1020 Green Acres Rd #5 - Eugene, OR 97408 * Phone: (541) 345-7970 * www.deltaoaksvet.com Dilated cardiomyopathy Dilated cardiomyopathy, DCM Affected Animals: The dogs most frequently diagnosed with DCM are large and giant purebred dogs, including Scottish deerhounds, Doberman pinschers, boxers, Saint Bernards, Afghan hounds, Newfoundlands, and old English sheepdogs. Recently, both E
Letter to Branches For instant updates: http//:www.cwu.org email: info@cwu.org 150 The Broadway, Wimbledon, London, SW19 1RX Tel: 020 8971 7200 Fax: 020 8971 7300 General Secretary: Billy Hayes (www.billyhayes.co.uk) No. 527/09 To: All Branches Dear Colleagues Swine Flu - HPA Advice on Exclusion from Workplaces and Schools This LTB is being issued further to LTB 394/09 dated 5 May 2
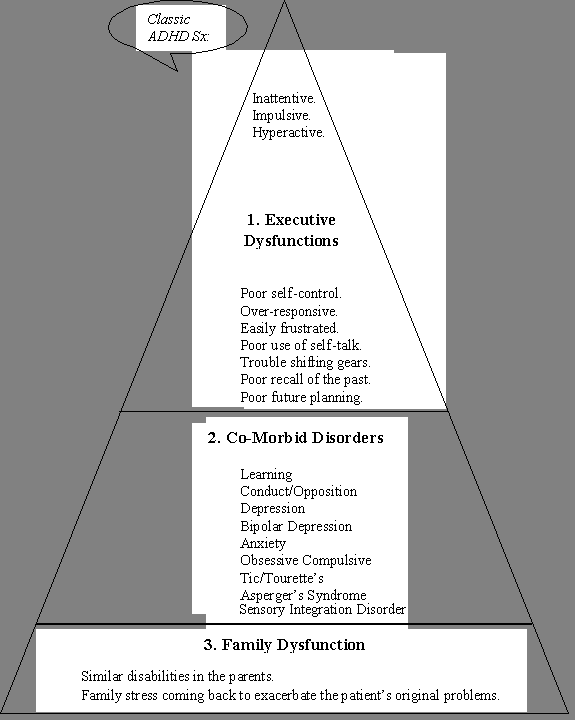 Figure 1. The extended spectrum of problems experienced by people with ADHD.
Figure 1. The extended spectrum of problems experienced by people with ADHD.