Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
1507nd0040
Nephrol Dial Transplant (2000) 15: 975–980
Prevalence and characterization of renal tubular acidosis in patients with osteopenia and osteoporosis and in non-porotic controls
Wolfgang Weger, Peter Kotanko, Martin Weger, Hannes Deutschmann and Falko Skrabal
Department of Internal Medicine, Krankenhaus der Barmherzigen Bru¨der, Graz, Austria
Abstract
trations and capillary pH did not differ between the
Background. Chronic metabolic acidosis may increase
alkali mobilization from the bone and thus promote
Conclusion. Incomplete RTA I may be prevalent in a
the development of osteoporosis. The objective of the
significant proportion of patients suffering from osteo-
current study was to compare urinary acidification in
penia or osteoporosis. The outcome of the frusemide
patients with reduced bone mineral content with that
test suggests either a defect of the H+ATPase in the
in control subjects with normal bone density.
cortical collecting tubule (CCT ) or a defective Na+
Methods. Forty-six subjects (41 females, 5 males) with
reabsorption in the CCT. Prospective studies are
osteopenia or osteoporosis were studied. In none of
needed to further elucidate the impact of incomplete
the subjects were overt metabolic acidosis, derange-
RTA I on the development of reduced bone mineral
ment of potassium homeostasis, or renal insufficiency
present. Distal tubular acidification was studied bymeans of oral ammonium chloride loading test
Keywords: acidosis; metabolic acidosis; osteopenia;
(0.1 g/kg body weight) and the oral frusemide test
osteoporosis; renal tubular acidosis; RTA I
(40 mg). In addition the frusemide test was performedin 20 healthy age- and sex-matched controls (17females, 3 males). Introduction Results. In all control subjects a urinary pH <5.5 was observed following the ingestion of 40 mg frusemide.
In Western industrialized countries an average 70-kg
In contrast, in patients with reduced bone mineral
adult ingests a diet that generates approximately 70
density incomplete renal tubular acidosis type I (RTA
mEq of acid per day. Physiologically, this acid chal-
I ) was diagnosed in 10 of 46 subjects (22%) by oral
lenge is dealt with by the kidneys, which excrete 70
ammonium chloride loading test. Disorders possibly
mEq of acid, 40 mEq/day as ammonium ions and 30
related to RTA I were detected in eight of these 10
mEq as titratable acid [1]. In steady state the renal
patients. Thirty-six patients had a normal urinary pH
acid excretion equals the endogenous acid production
response following oral ammonium chloride loading.
and thus acid–base balance is neutral. A positive body
Oral frusemide, 40 mg, failed to lower urinary pH
acid balance may be induced either by a significant
<5.5 in sixteen patients (35%), these included 10 rise of endogenous acid production that exceeds the
subjects with incomplete RTA I, and six subjects with
renal acid excretion capacity, or by defects of the renal
a normal oral ammonium chloride loading test. An
acid excretion [1]. In response to a positive acid
abnormal frusemide test was found in 35% of patients
with reduced bone mass and in none of the normal
and pH decrease and activate homeostatic mechanisms
controls ( x2=7.39; P<0.01). With the ammonium
to restore acid–base balance. The renal excretion of
chloride test as the gold standard for diagnosis of
4 may more than double, whereas the excretion of
distal RTA, the frusemide test showed a sensitivity of
titratable acid shows only a minor increase [1]. Despite
1.0 (95% CI, 0.69–1.0) and a specificity of 0.89 (95%
these homeostatic mechanisms, the acid balance may
CI, 0.78–0.96) for the diagnosis of distal RTA. Patients
remain positive, triggering a release of alkali from the
with incomplete RTA I were younger than those with-
bone. A prolonged alkali release from the bone will
out incomplete RTA I (42±16 vs 54±14 years; P=
eventually lead to reduction of total bone mass [2].
0.025; mean±SD). Basal serum bicarbonate concen-
Subjects with a reduced renal acid excretory reserve,
e.g. in the setting of incomplete distal renal tubularacidosis (renal tubular acidosis type I (RTA I )), may
Correspondence and offprint requests to: Peter Kotanko MD,
be at extra risk of bone mineral loss especially when
Department of Internal Medicine, Krankenhaus der BarmherzigenBru¨der, Marschallgasse 12, A-8020 Graz, Austria.
ingesting the usual mixed Western diet. Recently we
2000 European Renal Association–European Dialysis and Transplant Association
observed a high prevalence of incomplete distal tubular
>1500 g (n=4), autoimmune thyroid disease (n=3), nephro-calcinosis due to medullary sponge kidney (n=1), and a
acidosis and ‘primary’ osteoporosis [3]. The current
familial history of incomplete RTA I (n=1). The patients
study was undertaken to estimate the prevalence of
with thyroid disease had been prescribed thyroid hormone
incomplete RTA I in subjects with a reduced bone
to achieve normal basal TSH levels. Hypercalciuria was
mineral content as compared to subjects with a normal
defined as a daily urinary excretion of calcium >4 mg/kg
bone density and to further define the mechanism of
body weight. Patients with hypercalciuria had not been
RTA I in this group of patients. A secondary goal was
advised to follow a Ca-restricted diet.
to study the test characteristics of the frusemide test.
The classical causes of secondary osteoporosis (glucocort-
icoid excess, hyperthyroidism, primary hyperparathyroidism)were ruled out by measurement of thyroid hormone (free
Subjects and methods
T3, free T4, basal TSH ), serum calcium and iPTH, and onthe basis of clinical examination and patient history.
In none of the patients were renal insufficiency or overt
Study population and biochemical methods
metabolic acidosis present. The presence of RTA type IV(due to hyporeninaemic hypoaldosteronism) was considered
Sixty-six subjects, 58 females and 8 males, were studied.
unlikely because of normal serum potassium concentrations.
Forty-six subjects (41 females, 5 males) suffered from osteo-
Urinary pH was measured with a KCl electrode (pH-meter
porosis or osteopenia, 20 subjects were matched healthy
E 512, Metrohm, Herisau, Switzerland ). Urinary tract
controls (age 46±7 years; 17 females, 3 males) with a normal
infection was ruled out by urinalysis.
bone mineral density. The patients were referred by primary
In all 46 patients both an oral ammonium chloride
care physicians to our hospital for suspected osteoporosis.
(NH Cl ) loading test and an oral frusemide test was per-
The subjects do not resemble a cohort of patients with
formed; in 20 controls the frusemide test was done. In
osteoporosis and incomplete RTA I described recently [3].
addition, three patients with a positive frusemide test and a
All subjects were on standard hospital diet, which provides
negative NH Cl loading test consented to a fludrocortisone-
on average 120 mmol sodium chloride, 1000 mg of calcium,
and 70 g of protein per day. No dietary extremes (e.g. high-
Prior to the frusemide loading test patients were off
or low-protein diet, low-sodium diet) were given.
In all subjects (patients and controls) bone mineral density
(NSAID) for at least 2 days. The patients were given 40 mg
was assessed at the lumbar site (L2–L5) using dual energy
of frusemide orally and urinary pH was measured 0, 2, 4,
X-ray absorptiometry on a Sophos XLA machine. According
and 6 h after the frusemide dose [6 ]. In case of the fludrocort-
to the criteria proposed by the World Health Organization
isone-modified frusemide test, oral frusemide was preceded
( WHO), osteopenia and osteoporosis were diagnosed by a
on the previous evening by 0.5 mg of fludrocortisone. At
reduced bone mineral density (t-score −1.0 to −2.5, or
least 2 days after the frusemide test the standardized short
t-score <−2.5 respectively) measured by DXA [4]. Any
course oral NH4Cl test was performed [7]. Briefly, patients
radiological evidence of vertebral fractures was also taken as
ingested 0.1 g/kg body weight of NH4Cl in gelatin capsules.
a diagnostic criterion of osteoporosis. Applying these dia-
Blood gas analysis was performed from capillary blood with
gnostic criteria, 20 patients (43%) had osteopenia and 26
an AVL 995 Hb automatic blood gas system (AVL, Graz,
patients (57%) had osteoporosis. The baseline characteristics
Austria) on an hourly basis. The metabolic acidosis induced
of the study population are shown in Table 1.
by the NH4Cl load was documented by a fall of serum
Sixteen patients had disorders possibly associated with
3 concentrations >3 mmol/1 and a pH <7.35. Urinary
impaired renal distal tubular acidification, namely hypercalci-
pH was measured at baseline and 2, 4, and 6 h after the
uria with (n=2) and without nephrolithiasis (n=2), past
completion of NH Cl intake. Failure to lower urinary pH to
history of nephrolithiasis without current hypercalciuria
less than 5.5 is consistent with some form of distal RTA I
(n=3), habitual analgesic abuse with a cumulative amount
[4]. Each subject drank at least 500 ml of water duringthe test. Table 1. Baseline characteristics of the patients with reduced bone mass
The t-test of untransformed data was used for group compar-ison of patients with and without a normal response in the
NH4Cl test. A P value <0.05 was considered as significant.
Data are shown as mean and ±SD. The 95% confidence
interval (CI ) of relative frequencies was derived from the
binomial distribution. Absolute frequencies were compared
4Cl test as the gold standard for the diagnosis
of distal RTA, the diagnostic performance of the frusemide
test was evaluated in terms of sensitivity and specificity. The
failure to lower urinary pH <5.5 both in the NH Cl and
the frusemide test was considered as a true positive ( TP)
result, whereas an appropriate urinary acidification in both
tests was scored as a true negative ( TN ) outcome. False
positive ( FP) and false negative ( FN ) frusemide testswere
Mean±standard deviation; aP=0.025 (two-sided).
TP/(TP+FN ), specificity was defined as TN/( TN+FP) [8].
Incomplete RTA I in osteopenia and osteoporosis
Patients with incomplete RTA I presented on average
12 years younger as compared to patients withoutRTA I (95% CI, 1.6–22.4 years; P=0.025; Table 1).
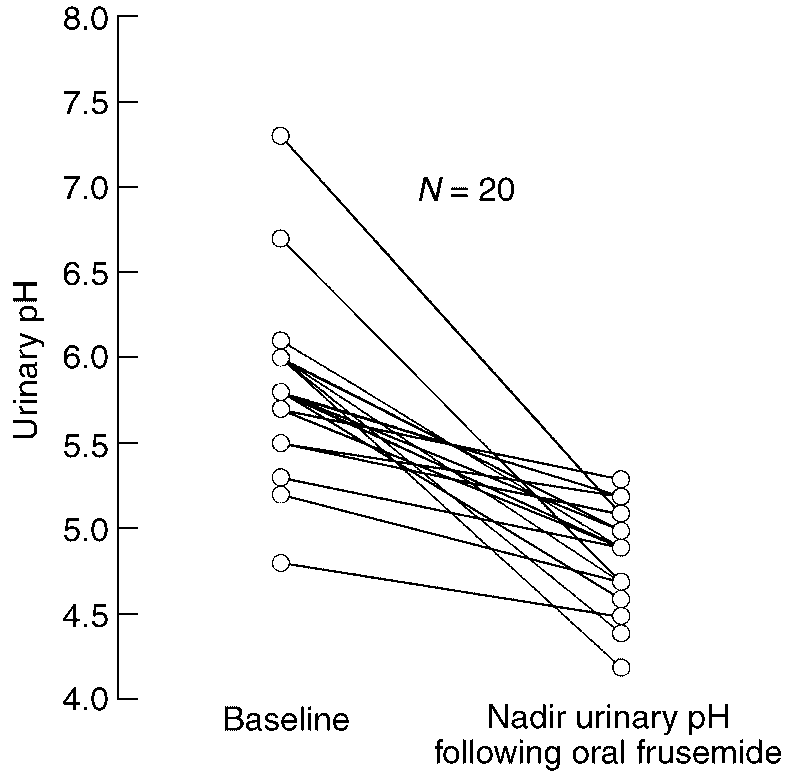
In all control subjects (100%; 95% CI, 83–100%) the
Four of 26 (15%) patients with osteoporosis and six
administration of oral frusemide resulted in a fall of
of 20 patients with osteopenia (30%) had incomplete
the urinary pH below 5.5 (Figure 1).
Overt metabolic acidosis, impaired renal function,
In eight of the 10 subjects with incomplete RTA I,
or disturbances of potassium metabolism were not
the following disorders possibly related to incomplete
observed in the patients studied. In 30 patients (65%)
RTA I were present: nephrolithiasis and hypercalciuria
both NH Cl testing and the oral frusemide test revealed
(n=2), autoimmune thyroid disease (n=2), long-term
normal responses, i.e. a fall of urinary pH <5.5
habitual analgesic abuse (n=2), nephrocalcinosis due
to medullary sponge kidney disease (n=1), and a
Ten patients (22%) failed to lower urinary pH below
familial history of RTA I in one patient. In two
5.5 ( Table 1, Figure 2c) despite the induction of sys-
patients with incomplete RTA I, no associated dis-
temic metabolic acidosis following the ingestion of
orders were revealed. In those six subjects with a
NH Cl. In these 10 patients the diagnosis of incomplete
normal NH4Cl test but an abnormal urinary pH
RTA I was made. All of these patients with incomplete
response to oral frusemide, a past history of nephroli-
RTA I showed also a urinary pH above 5.5 during the
thiasis without current hypercalciuria (n=1), and auto-
frusemide test (Figure 2c). Additionally, six subjects
immune thyroid disease (n=1) were present. In the 30
(13%) with a normal NH4Cl test failed to lower urinary patients with both a normal frusemide and NH Cl
pH <5.5 during the frusemide test (Figure 2b). In
test, hypercalciuria (n=2), habitual analgesic (n=2),
three patients of the latter group a fludrocortisone-
and a past history of nephrolithiasis without current
modified frusemide test resulted in essentially the same
hypercalciuria (n=2) were recognized.
outcome, i.e. the failure to lower urinary pH below 5.5
With the NH Cl test as the gold standard for
(nadir urinary pH, 6.5, 6.0, and 6.1 respectively). An
diagnosis of distal RTA the frusemide test showed a
abnormal frusemide test was significantly more fre-
sensitivity of 1.0 (95% CI, 0.69–1.0) and a specificity
quent in osteopenic/osteoporotic patients as compared
to the control group ( x2=7.39; P<0.01).
Serum bicarbonate, capillary pH, pCO2, serum creat-
inine, and potassium were within the normal range
Discussion
and did not differ between the two groups (Table 1).
In the group of patients with normal NH4CI testing Bone is critically involved in buffering during the
but an abnormal frusemide test (n=6) serum bicarbon-
chronic stages of metabolic acidosis [9,10]. A chronic-
ate (23.5±1.2 mmol/l ), capillary pH (7.4±0.02),
ally positive acid balance, e.g. due to an impairment
and capillary pCO2 (38.3 mmHg), serum creatinine of renal acid excretion, may trigger the release of alkali
(0.9±0.15 mg/dl ), and serum potassium (4.2±
and calcium from the bone and eventually lead to
0.39 mmol/l ) were also not different from those in
reduction of bone mass and osteoporosis. In the past,
subjects (n=30) with normal responses in either dia-
the idea of chronic retention of acid as a possible
cause of osteoporosis, particularly in postmenopausalwomen, was put forward by Sebastian et al. [11]. Sanchez and Libman [12] described both proximal anddistal renal tubular acidosis in eight patients withosteoporosis. Recently we described a high prevalenceof incomplete RTA I in patients with ‘primary’ osteo-porosis [3].
The RTA syndromes encompass a disparate group
of disorders that have in common an inability toexcrete acid that is out of proportion to any reductionin glomerular filtration rate. RTA type I involvesdefects of acid excretion confined to the distal tubule. The hallmark of overt RTA type I is a hyperchloraemicmetabolic acidosis accompanied by a reduced net acidexcretion and the inability to lower urinary pH below5.5 in the face of spontaneous acidaemia or after acidloading. In the complete form of RTA I plasmaHCO−
3 concentration is typically reduced. Incomplete
RTA I may be suspected if in random urine spotsamples urinary pH is Á5.5 [4]. The definite diagnosis
Fig. 1. Urinary pH in response to oral frusemide in 20 healthy
of incomplete RTA I requires the induction of a
controls. All subjects were given an oral dose of 40 mg frusemide.
systemic metabolic acidosis by means of acid loading.
Data represent the baseline and the nadir urinary pH during aperiod of 6 h following oral administration of frusemide.
Among the various acid-loading protocols the NH Cl
Fig. 2. Urinary pH in response to a short-course oral NH Cl loading and to frusemide. All subjects were given 0.1 g
encapsulated NH Cl and an oral dose of 40 mg frusemide. Data represent the base line and the nadir urinary pH during a period of 6 h
following the NH Cl ingestion and frusemide respectively. (a) Results obtained in patients with both normal NH Cl and frusemide testing
(n=30). Note that in nine subjects the individual urinary pH responses to NH Cl loading were similar. (b) Results in six patients with a
normal NH Cl test but an insufficient fall of urinary pH following the frusemide test. (c) Individual urinary pH data in 10 patients with
loading test introduced by Wrong and Davies [13] has
was not observed in these patients which is compatible
recognized wide-spread clinical application. Since dis-
solved NH Cl may cause abdominal discomfort and
Unfortunately, the NH Cl test is frequently accom-
even vomiting we preferred to administer NH Cl in
panied by abdominal discomfort, even when encapsul-
gelatin capsules. In this gelatin form the test was better
ated NH4Cl is used. None of the patients studied by
tolerated and no vomiting was observed. To give
us agreed to a prolonged NH Cl loading test over
reliable results systemic acidosis has to be induced by
RTA I resembles a diagnosis with a variety of
4Cl load. A fall of capillary pH below 7.35 in
conjunction with a fall of serum HCO− concentration
underlying aetiologies. Despite a recognized associ-
>3 mmol/l is considered to reflect a sufficient degree ation of RTA I with disorders such as medullaryof acidaemia [5], which was observed in all test sub-
sponge kidney, hypercalciuria, analgesic nephropathy,
jects. The NH Cl loading test was performed in all 46
and immuno-mediated diseases such as lupus nephritis,
subjects, resulting in an inadequate urinary acid-
Sjo¨gren syndrome, and Graves disease [14], the cause
ification in 10 patients, who therefore were diagnosed
of RTA I in some patients remains obscure. Recently,
having incomplete RTA I. Overt metabolic acidosis
in some of these idiopathic forms of RTA I the absence
Incomplete RTA I in osteopenia and osteoporosis
of H+ATPase in the intercalated cells has been shown
renal function showed that the oral dose of 40 mg may
[15]. In all but two patients of the RTA I group a
be too low in obese subjects; in this subject, 80 mg of
thorough work-up revealed disorders with a recognized
frusemide were necessary to produce a normal urinary
association with RTA I. In addition, in two of the six
acidification. None of the patients studied was over-
patients with an abnormal frusemide test and a normal
weight. It has been suggested recently that the adminis-
NH Cl test disorders possibly related to distal tubular
tration of a mineralocorticoid such as fludrocortisone
acidification disturbances were present. One may
on the evening preceding the frusemide test may reduce
speculate that in some of these patients these disorders
the frequency of false positive results of the frusemide
may have contributed to the blunted urinary pH
test [5]. In our hands, a fall of urinary pH <5.5 was
not observed in the three frusemide-positive and
Acidification in the collecting tubules (CT ) is primar-
NH Cl-negative subjects who agreed to a fludrocorti-
ily achieved via H+ secretion by a luminal H+ATPase
sone-modified frusemide test, supporting the view that
[16 ]. This pump is located in the intercalated cells of
some form of tubular dysfunction is present. In future
the cortex and in the medulla. The H+ secretion by
studies, the additional measurement of urinary citrate
intercalated cells of the cortical collecting tubule (CCT )
and NH+ excretion may provide additional insights
is indirectly influenced by the Na+ reabsorption of the
adjacent principal cells, since the removal of Na+ from
A distal acidification defect was found in 10 of 46
the tubular fluid generates a lumen-negative potential
patients (22%; CI, 11–36%) with reduced bone mineral
which facilitates net H+ secretion by minimizing the
content patients when tested by the NH4Cl test and in
degree of passive proton back-diffusion. Any reduction
as many as 16 of 46 (35%; CI, 21–50%) by the
of Na+ reabsorption in the CCT diminishes the degree
frusemide test. When interpreting these frequencies one
of lumen negativity (a condition called voltage-
has to appreciate that the primary aim of the study
dependent defect) and results in a reduced H+ net
was not to estimate the prevalence rates of RTA I in
secretion and an inability to lower the urinary pH.
patients with osteoporosis or osteopenia. However, it
Application of frusemide provides a means of increas-
is noteworthy that renal acidification was normal in
ing the delivery of sodium to the sites of distal Na+
all 20 subjects with normal bone density. Since the
reabsorption. Following a rise in intraluminal sodium
patients studied were referred to the hospital because
the Na+ reabsorption in the CCT increases [6 ] fol-
of suspected osteoporosis, data are not controlled for
lowed by a decrease of tubular fluid pH. In RTA I a
referral bias. Studies in a randomly selected group of
common problem is thought to be a defect in the
patients with osteopenia or osteoporosis as compared
H+ATPase pump that may be present in the cortex
to matched controls with normal bone densities are
and/or the medulla. Patients with this type of RTA I
needed to obtain an unbiased estimation of the
may or may not respond normally to the administra-
prevalence of renal acidification defects.
tion of frusemide. In situations where the H+ATPase
It is interesting to note that subjects with incomplete
defects are limited to the medullary collecting duct, an
RTA I presented at an earlier age ( Table 1).
acidification of the urine may be expected, since the
Admittedly, this observation may arise from patient
medullary H+ secretion is essentially Na+ independent
selection due to referral bias, but it is attractive to
[17]. In contrast, a defective H+ secretory pathway in
speculate that subjects with incomplete RTA I are
the CCT is expected to cause an inability to lower the
prone to a more rapid loss of bone mineral and
urinary pH following frusemide application. The
therefore present at a younger age. Clearly, an addi-
response of urinary pH to frusemide may be blunted
tional prospective study in an age- and sex-matched
by the presence of amiloride-type diuretics [18],
group of patients with and without incomplete RTA I
NSAIDs, and volume contraction. Therefore we took
is needed to define the rate of bone loss in patients
care to perform the tests in clinically euvolaemic
patients being off diuretics and NSAIDs for at least 2
In conclusion, incomplete RTA I, both primary and
days. The outcome of the frusemide test in the 10
secondary, is prevalent in patients suffering from
patients with incomplete RTA I studied by us suggests
reduced bone mineral content. Because of a reduced
either a defect of the H+ATPase in the CCT or a
renal acid excretory reserve in these subjects the inges-
defective Na+ reabsorption in the CCT, whereas a
tion of nutrients stimulating the endogenous acid pro-
defective H+ secretion in the medullary collecting
duction (e.g. a diet rich in proteins) may induce a
positive acid balance which eventually promotes the
A dose of 40 mg frusemide given orally was chosen
release of alkali and calcium from the bone.
since none of the patients studied had renal insuffi-
Acknowledgements. This study was supported by the Fonds zur
ciency (the maximum serum creatinine concentration
Forderung der wissenschaftlichen Forschung, Austria, SFB 007
in the study population was 1.1 mg/dl ) and since we
wanted to avoid significant volume depletion. Inpatients with renal insufficiency a dose of 80 mg
References
frusemide has been advocated in order to overcomethe accompanying resistance to frusemide [19].
1. Alpern RJ, Sakhaee K. The clinical spectrum of chronic meta-
Circumstantial evidence from a non-osteoporotic
bolic acidosis: homeostatic mechanisms produce significant
female with a body weight of 111.5 kg and normal
morbidity. Am J Kidney Dis 1997; 29: 291–302
2. Myburgh KH, Noakes TD, Roodt M, Hough FS. Effects of
11. Sebastian A, Harris ST, Ottaway JH, Todd KM, Morris RC jr.
exercise on the development of osteoporosis in adult rats. J Appl
Improved mineral balance and skeletal metabolism in post-
menopausal woman treated with potassium bicarbonate. N Engl
3. Weger M, Deutschmann H, Weger W, Kotanko P, Skrabal F.
Incomplete renal tubular acidosis in ‘primary’ osteoporosis.
12. Sanchez A, Libman J. Trastornos de los mecanismos renales de
acidificacion en pacientes osteoporoticos. Medicina Buenos AiresOsteoporos Int 1999; 10: 325–329
4. Assessment of fracture risk and its application to screening for
13. Wrong O, Davies HEF. The excretion of acid in renal disease.
postmenopausal osteoporosis. Report of WHO study group. World Health Organization Technical Report Series 1994; 843:
14. Konishi K, Hayashi M, Saruta T. Renal tubular acidosis with
autoantibody directed to renal collecting-duct cells. N Engl
5. Walter SJ, Shirley DG, Unwin RJ, Wrong OM. Assessment of
urinary acidification. Kidney Int 1999; 55: 2092 (abstract)
15. Joo KW, Jeon US, Han JS et al. Absence of H+ATPase in the
6. Batlle D. Segmental characterisation of defects in collecting
intercalated cells of renal tissues in classical distal renal tubular
tubule acidification. Kidney Int 1986; 30: 546–554
acidosis. Clin Nephrol 1998; 49: 226–231
7. Garella S, Salem MM. Clinical acid-base disorders. In: Davison
16. Levine DZ, Jacobson HR. The regulation of renal acid excretion:
AM, Cameron JS, Grunfeld JP, Kerr DNS, Ritz E, Winearls
new observations from studies of distal nephron segments.
CG, ed. Oxford Textbook of Clinical Nephrology. Oxford
University Press, London: 1998: 311–358
17. Lombard WE, Kokko JP, Jacobson HR. Bicarbonate transport
8. Griner PF, Mayewski RJ, Mushlin AI, Greenland P. Selection
in cortical and outer medullary collecting tubules. Am J Physiol
and interpretation of tests and procedures. Ann Intern Med
18. Batlle D, Flores G. Underlying defects in distal renal tubular
9. Barzel US. The effect of excessive acid feeding on bone. Calcif
acidosis: new understandings. Am J Kidney Dis 1996; 27: 896–915
19. Rose H, O’Malley K, Pruitt A. Depression of renal clearance
10. Green J, Kleeman CR. Role of bone in regulation of systemic
of furosemide in man with azotemia. Clin Pharmacol Ther 1976;
acid–base balance. Kidney Int 1991; 39: 9–26
Received for publication: 1.3.99Accepted in revised form: 9.2.00
Unexpected high serum levels of tacrolimus aftera single topical application in an infantResearch Institute for Environmental Health at the Heinrich-Topical tacrolimus has been found to be effective andsafe for the treatment of atopic dermatitis in adults andSupported by the Elterninitiative Kinderkrebsklinik e. V., Du¨sseldorf, andchildren.We report an infant with severe combinedDeutsche
Ripken Foundation to back 5 ballparks in city Working with community groups, the Swing for the Future campaign plans to build first at old Memorial Stadium site Teri Joyner (left), director of the Park Heights Boys and Girls Club, and Ken Darden, the Baltimore Metropolitan Boys and Girls Club's president and chief executive, look forward to improvements at the C.C. Jackson Recreation C
 Incomplete RTA I in osteopenia and osteoporosis
Patients with incomplete RTA I presented on average
12 years younger as compared to patients withoutRTA I (95% CI, 1.6–22.4 years; P=0.025; Table 1).
Incomplete RTA I in osteopenia and osteoporosis
Patients with incomplete RTA I presented on average
12 years younger as compared to patients withoutRTA I (95% CI, 1.6–22.4 years; P=0.025; Table 1).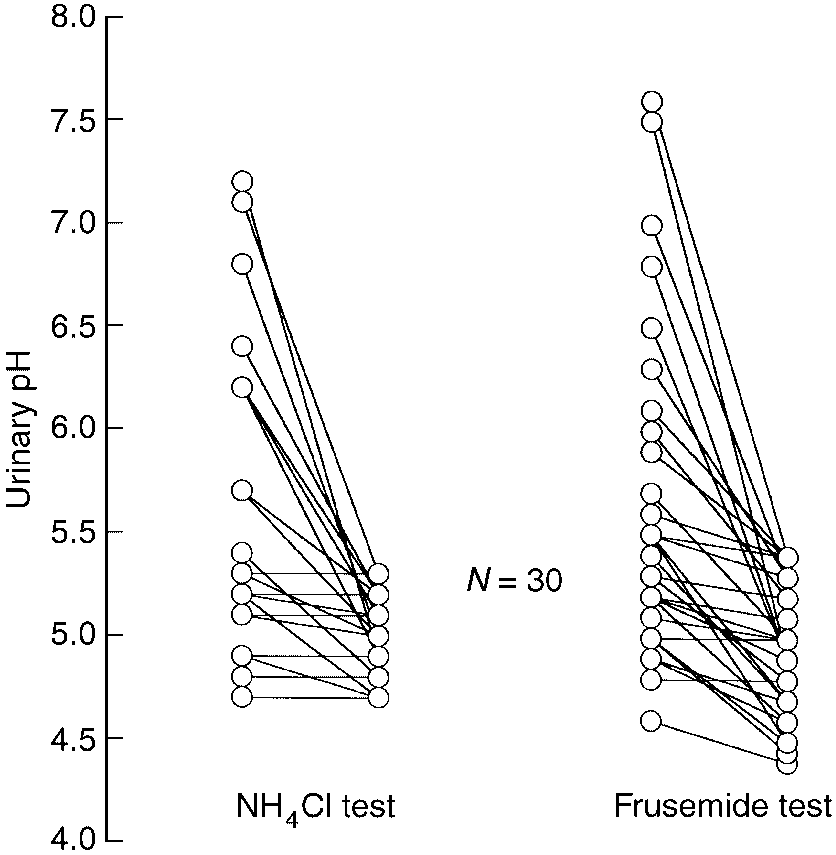
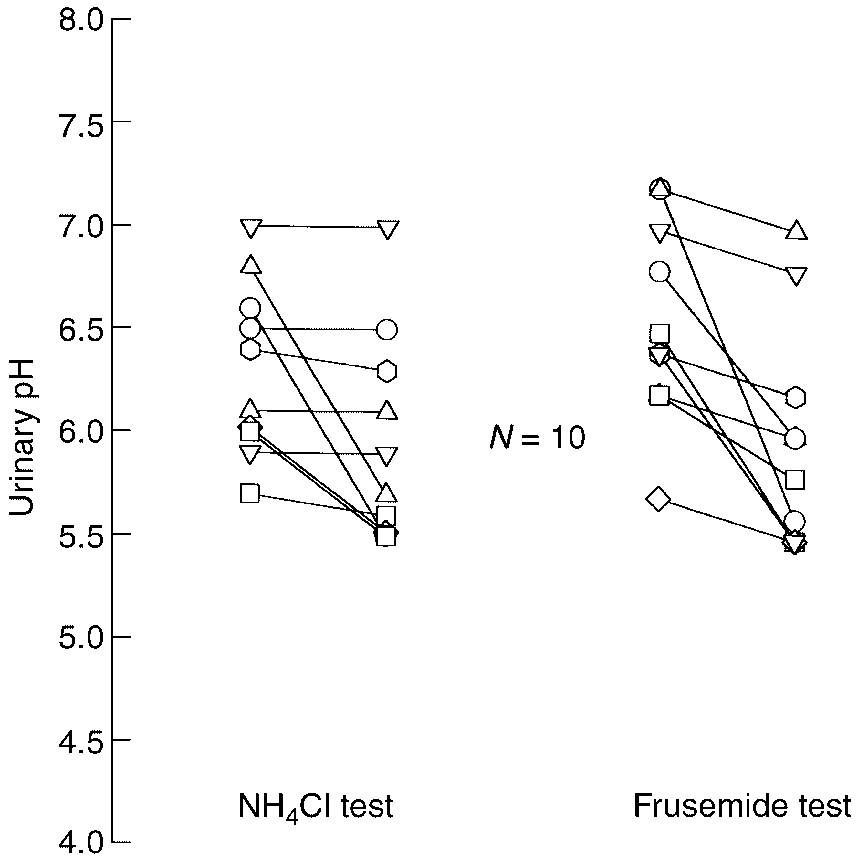
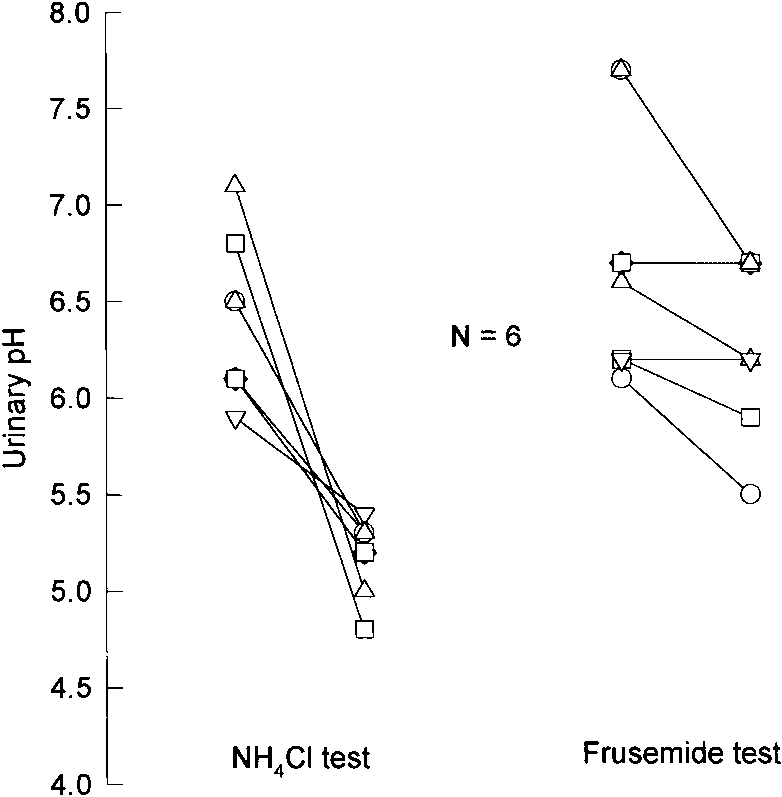 Fig. 2. Urinary pH in response to a short-course oral NH Cl loading and to frusemide. All subjects were given 0.1 g
Fig. 2. Urinary pH in response to a short-course oral NH Cl loading and to frusemide. All subjects were given 0.1 g