Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Dafne bi scenarios
Implementing the most clinically effective background insulin regimen Stephanie A Amiel & Anita Beckwith
IN BLUE the main points raised in Comparisons with once‐daily or twice‐daily basal insulin regimen: † indicates p value = non significant; * differences are adjusted for baseline variable Variable Once Daily P value Twice daily P value Pre‐DAFNE Post‐DAFNE Pre‐DAFNE Post‐DAFNE Patients n(%), on basal insulin regimes (for whom data available @ 1 year) Severe hypogycaemia Severe hypogycaemia P Pre‐DAFNE Post‐DAFNE ‐ 1yr value† value‡
BD Isophane works well - DAFNEEvening isophane best given at bedtime (late) -
Fanelli et al., Ann Intern Med. 2002;136:504-14
Logically rules for Isophane should work for Levemir
Levemir probably most reproducible absorption day to day
and this is very appreciated by patients. May be useful if
fasting glucoses very variable with full DAFNE regimen on
PRE-DAFNE Most practices are using analogues19/20 using Lantus, of which 1 uses bd dose routinely and 6 use od and bd and one converts od to bd pre course. Only 6 routinely reduce doses that
18/20 do use Levemir also, of which 6 use it od at
3/20 routinely use Lantus pre breakfast; 1/20 pre-
With bd Levemir, 8 prescribe “12 hourly”; 9 “pre- Consensus that bd is preferable and most agree initially 50@50 split. Pre-course: Many do support move to bd Lantus or LevemirShould do this especially if patient is exerciser or shift workerDuring or Post-course: often convert remaining od users to bd because Changing in the course allows the patient to learn from own data BUT reduces opportunity for patient to learn about dose adjustmentChanging pre-course requires educator to trust DAFNE and be able to convince patient to trust DAFNE and then allows full exploitation of the daily dose adjustments for all 5 daysChanges from Lantus need to happen Friday night before the courseAll other changes Sunday night before the courseCalculate BI referring to Berger regimenSome like to introduce large change more slowly and incrementally over 2 weeks prior to course, but this may need significant extra time from the educator and should not usually be necessary if we assume DAFNE
Patient forget second dose after years of one onlySuggested solutions: set up mobile ‘phone alarm; keep BI pen in the toothglass with the toothbrush (or paste!)
Overlap from previous insulin affecting dose decision Which insulin to use? Argument for splitting the insulin the patient is using BUT no logic/evidence for splitting a 24 hr insulin and lantus not licenced for bd use.
Worries about Lantus and cancer in that setting Many therefore use isophane or, if there is evidence for nocturnal hypoglycaemia pre-analogue use, bd
Consensus that Levemir is weaker than Lantus and Isophane and may need to increase to 28 – 34 Changing from a ‘conventional’ basal/bolus regime: Option 1 (isophane or Levemir): ‘Berger regime’: 12u at bedtime and 12u in the morning, as above.
Starting from Sunday bed-time, with a suggested QA dose for
Adapt starting doses according to insulin sensitivity. Option 2 (Lantus): Consider leaving dose of Lantus unchanged, or approx 24u/24hrs (adapt according to sensitivity). Main benefits from Lantus (ie reduced fasting BG) may be achieved from taking it at bedtime, rather than in the morning.
If planning to convert from Lantus to isophane or Levemir, consider the ‘washout’ period for Lantus and plan to change 2-3 days prior to the course. Pre- and post-course changes It is important to realise that these scenarios are designed for discussion of dose adjustment and all solutions would need to be adjusted for the individual patient The team’s solution: do nothing. Long duration of diabetes, let patient discover problems of regimen during weekThe group’s discussion. Total daily dose, divide 50/50 into BI and QA. Result Levemir 8 units bd and 1:1 QA for meals from Sunday nightDiscussion: should probably reduce total dose by ~20% if distributing more physiologically BUT need more levemir than LantusWHAT HAD BEEN DONE REALLY: Converted to Lantus 16 units bedtime DISCUSSION: Group very anxious about doubling BI BUT:1. The start QA:BI ratio is 75/25 not 50/502. The low breakfast dose and high evening meal dose strongly suggests too much basal in the morning and not enough at night3. With bd 8 units you are just giving the same background replacement during the day as during the night4. With 16 units of Lantus you are both trusting DAFNE (need for background insulin throughout the 24 hours) AND Lantus (active dose will be absorbed steadily through the 24 hours, so patient will NOT suddenly get a much bigger active dose at night5. Probably reasonable to have checked a 3am glucose before making Team suggested no change and group agreed. All rather surprised after vigour of previous discussionRe-arrange Humulin I to 12 units bd if patient not obviously insulin resistant or 16 units bd if he is; and 1:1 or 1.5:1 QA. From MONDAY AM because he will have taken 30 units Sunday morning and may hypo overnight if 12 units then taken later that dayTeam solution : convert to 24 units of Lantus, 48 hours beforeGroup: We agreed, although some preferred gradual reduction over 2 weeks prior to course. NB this does mean more work and Team discussion: convert to Insulatard 12 am and bedtime and 1:1 QA night before course starts
The action taken is given in the 2nd
Scenario 1(a) Scenario 1(b) The conversion to split levemir from LantusWould normally require an increase in total doseBut not initially because Lantus effect will still bePresent on day one. Eventual dose 9 units bdScenario 2 (a) Scenario 2 (b) Run out of once daily basal and effects of exercise and alcohol. Needs bd to allowFlexibility. Prof Amiel suggested this patient must have been a man!Scenario 3 This patient has not yet been managed Group agreed there was clear evidence for a dawn And that converting to bd BI would not address this.Insulatard would likely make it worseSuggested that patient be asked to wake early (initially 6 am as this would be fairly convenient but may need to be earlier if already high by then, test and takeQA (initially 2 units but increase as required to achieve fasting target glucose) and go back to sleep until usual morning alarm. If this works it would prove dawn phenomenon and a pump would be required unless patient preferred to continue to wake to take extra QA 1. A lot of teams still using daily Lantus but agree advantages of bd BI regimen, especially flexibility2. IN discussion about which BI, there was felt to be an evidence base for isophane, no licence (or logic?) for Lantus and we should advise either isophane or levemir (if evidence of nocturnal hypo or high fasting glucoses on bd isophane in past; or if fasting glucoses very variable on isophane) as first line, using Lantus if patient very attached to 3. This is because DAFNE provides the evidence base
Lijst privé-tewerkstellingagentschappen erkend door het Brussels Hoofdstedelijk Gewest - bijwerking op 09/09/2010Ordonnantie van 26 juni 2003 betreffende het gemengd beheer van de arbeidsmarkt in het Brussels Hoofdstedelijk GewestDruk op Ctrl + F om een onderneming op te zoeken terbeschik- terbeschik- terbeschik- bemiddeling bemidde- kingstelling kingstelling Toegekend U
Environment and Crime in the Inner City: Does Vegetation Reduce Crime? Environment and Behavior 2001; 33; 343 The online version of this article can be found at:http://eab.sagepub.com/cgi/content/abstract/33/3/343Environmental Design Research Association can be found at: Environment and Behavior Additional services and information for Email Alerts: http://eab.sagepub.com/c
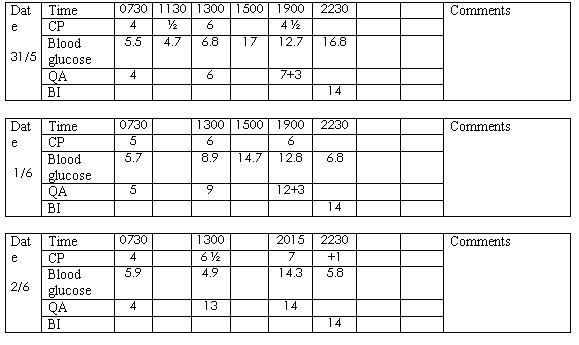 Scenario 1(a)
Scenario 1(a)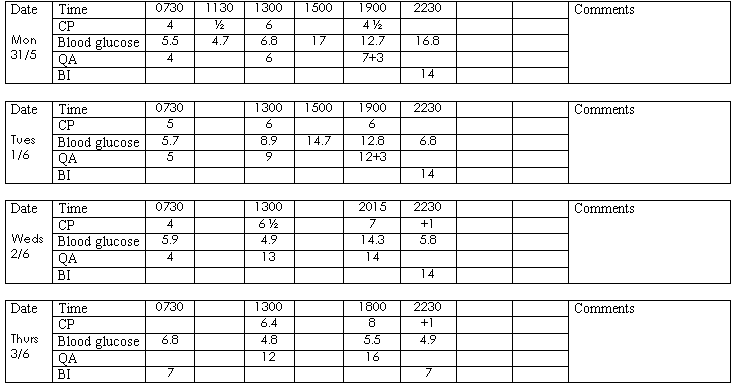 Scenario 1(b)
Scenario 1(b)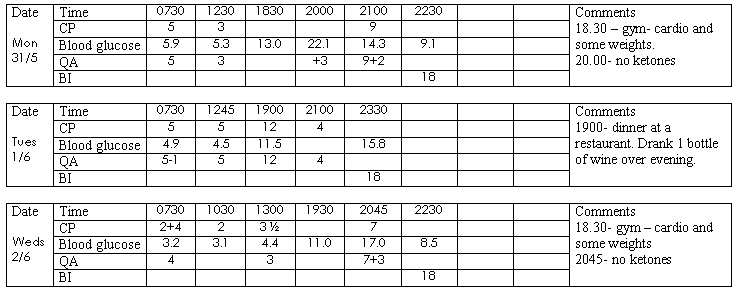 Scenario 2 (a)
Scenario 2 (a)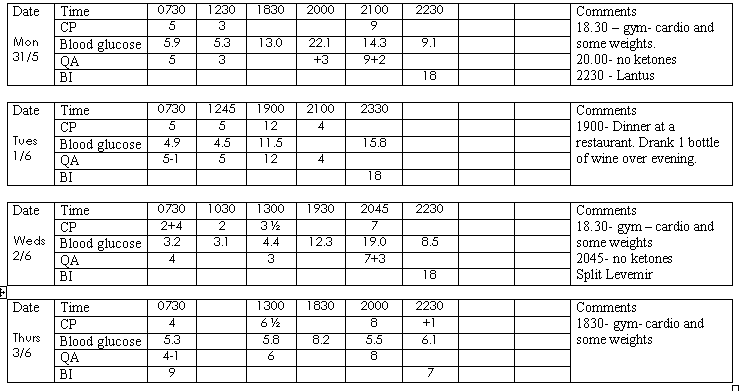 Scenario 2 (b)
Scenario 2 (b)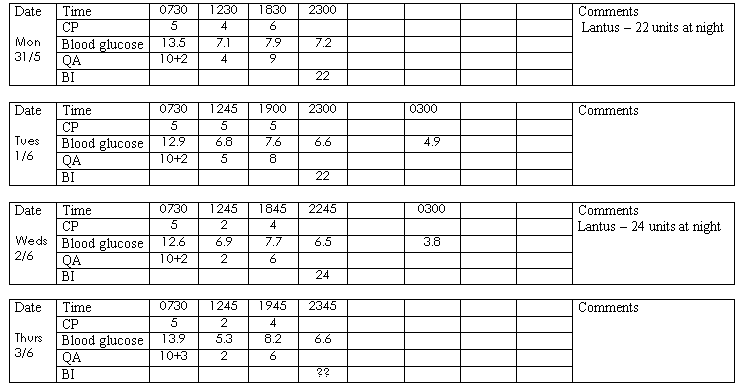 Scenario 3
Scenario 3