Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Microsoft powerpoint - leadershipforumpresentation_6-27-11_kg.ppt
Leadership Forum: Monitoring Psychoactive Medication Use in Children Laurel K. Leslie, MD, MPH Tufts Clinical and Translational Science Institute Tufts Medical Center Floating Hospital for Children Katherine E. Grimes, MD, MPH Children’s Health Initiative/Cambridge Health Alliance Harvard Medical School
Evolving patterns of use; both more meds and
Changes in health and mental health care
system; greater fragmentation, less oversight; change in role and training of prescribers
Limited information about efficacy of combined
Insufficient research on how new psych meds
work or effects on health from long-term use
Changing prescription rates in youth have led to concerns about :
increasing likelihood of co-prescription
adverse effects from drug interactions
Medications prescribed for emotional/behavioral
Also termed “psychoactive” or psychiatric meds;
some meds may impact both physical and mental conditions
Use of more than one psychotropic medication
Use of 4+ meds within or across drug classes
Some Common Classes of Psychotropic Medications Class Name Indications Examples
Psychotropic medication use increased 2-3
Among privately insured very young children
(2-5 years old), psychotropic medication use increased about 2-fold (Olfson et al, 2010)
Polypharmacy increased 2.5-8 fold (Olfson et
Increasing use of newer medications just
coming to market or medications being used “off-label”
multiple vulnerabilities making their care
limited agency in decisions regarding
risk of disparities in access to appropriatemedication and in medication use. As cited in NYT (12/11/2009): Crystal et al, 2009Use by Children in Foster Care
Estimated rates of medication use for children in
foster care range from 13-52% as opposed to 4% in general population. (dosReis et al., 2001; Kansas Health Policy Authority, 2008; Raghavan et al., 2005; Zima et al., 1999)
State-variation in use of 3 + psychotropic
medications for children with Autism Spectrum Disorder in foster care (Rubin et al., 2009)
Random sampling of 472 children in foster care in
Texas found 41% received three or more psychotropic drugs at the same time (Zito et al., 2008)System (Dis-)Coordination Mental Health Judge & Providers Therapist To Parents Probation Clinician(s) Foster Parents Biological CBHI in MA Community Parent(s) Child or Programs Adolescent Adoptive Worker(s) Parent(s) Agencies Teacher(s) & Affiliated School Staff Residential Hospital Intervention Psychiatrist
Delivery system changes have attenuated direct
psychiatric contact and increased prescribing-by-proxy for children and adolescents.
Insurance changes mean few psychiatrists can
see patients for therapy; psychiatric care is likely to be discontinuous (role reduced to “the psychopharm”).
Unfamiliar clinicians are more likely to add to,
rather than reduce, the numbers of medications being given when faced with a symptomatic child. Expanded “indicators” (Penn, 2006).
Limited Information about Meds in Children
Phase I: What are safe doses and common side effects?
Phase III: Is the drug better than standard care? (often ‘placebo’)
Phase IV: What else can we learn from post-marketing studies about medication risks, benefits, and optimal use?
Congress to Begin Investigation into SSI for Children On behalf of Disability Rights Law Center- Alex Boudov, Attorney at Law posted in Supplemental Security Income on Friday, January 21, 2011 Last month, we extensively discussed the many perceived problems with the Social Security Disability and Supplemental Security Income programs for children. Specifically, it is alleged that the allure of the monthly income and free medical care has motivated parents to place their children on psychiatric drugs they do not need because they think that being prescribed such medication is a near-requirement for qualification. In addition, we examined the increase of children qualifying for SSD and SSI based on mental, behavioral and learning disorders, and how that number has increased from 8 to 50 percent of all children receiving SSD or SSI in the past 20 years. Following the detailed news articles that gave rise to our blog posts, several members of Congress took notice of the alleged problems with the children's programs, and have pledged to launch an investigation into them. Currently, the federal children's disability programs have an average annual price tag of $10 billion, and they are quickly growing in both size and cost.
New information about adverse effects
supports ongoing assessment of efficacy vs. risk in psychotropic use
Prescribing trends for distinctly vulnerable groups
Variation in prescribing patterns by clinician
specialty, insurance type, etc. may contribute to health care disparities for certain groups
Identifying the gap between the evidence base for
psychotropics and prescribing practice patterns can help define training needs
Changing Federal Oversight of Medication Use in Children
1994- FDA proposes increasing study of medications in
1997-FDA Modernization Act (FDAMA): market exclusivity incentive if voluntarily conduct studies in children
2002-Best Pharmaceuticals for Children Act (BPCA): mandated 1 year post-marketing surveillance and reporting of adverse events FDA forms Pediatric Advisory Committee
Capturing prescribing trends creates a basis
measurement of the congruence between
provider practice patterns and the evidence base
identification of system enhancement
opportunities (i.e. electronic records) to protect youth from unnecessary risk
information to support clinician training to
ensure that children get the maximal opportunity to benefit from medication
Rosie D. remedy/ Children’s Behavioral
Medicaid-Mental Health Collaboration on
Psychoactive Medications in Children Workgroup
Challenges
Delivery system model (carve-outs) increases
Workforce capacity issues; both the cause and the result
Lack of self-policing among professional groups
Opportunities Increased focus on links between mental health status
and overall child outcomes (i.e. “ACE” study)
Families and purchasers asking for evidence-based
Health care reform (parity?); new quality standards
Conducted a national study of 47 states
1) Examined state policies and best practices
disseminate to other child welfare agencies
Attention to consequences of flags (“any teeth at
trigger feedback by prescriber patterns?
Feedback triggered by patient med use?
Need to monitor if children are getting MH
Multiple possible links to fed government activities
Strategies for increasing awareness of the issue
Importance of creating career opportunities so that
clinically trained child mental health workforce is available to meet the needs of youth and families
Learn what we know about medication use in
Learn what we know about medication use in
Consider how we can better use the data we
have to improve care (Leadership Forum Participants)
Identify some next steps (Leslie and Grimes)
DosReis, S., Zito, J., et al. (2001). Mental health services for youths in
foster care and disabled youths. American Journal of Public Health, 91(7), 1094-1099.
Kansas Health Policy Authority. Medicaid Transformation Report
2008.http://www.khpa.ks.gov/medicaid_transformation/download/2008/KHPA_2008_Medicaid_Transformation.pdf
McClellan, J. & Werry, J. (2003). Evidence-based treatments in child
psychiatry. Journal of the American Academy of Child and Adolescent Psychiatry, 42(12), 1388-400.
Olfson, M., Marcus, S.C., et al. (2002). National trends in the use of
psychotropic medications by children. Journal of American Academy of Child and Adolescent Psychiatry, 41(5), 514-521.
Olfson, M., Crystal, S., et al. (2010). Trends in antipsychotic drug use
by very young, privately insured children. Journal of the American Academy of Child & Adolescent Psychiatry, 49(1), 13-23.
Cascade, E., et al. (2006). Recent Changes in Prescriptions for
Antipsychotics in Children and Adolescents, Psychiatry, 3(9), 18-20.
Raghavan, R., Zima, B., et al. (2005). Psychotropic medication use in a
national probability sample of children in the child welfare system. Journal of Child and Adolescent Psychopharmacology, 15, 97–106.
Rubin D., et al. (2009). State variation in psychotropic medication use
by foster care children with autism spectrum disorder. Pediatrics, 124(2), 305-312.
Vitiello B, Riddle MA, et al. (2003). How can we improve the
assessment of safety in child and adolescent psycho-pharmacology? Journal of the American Academy of Child & Adolescent Psychiatry, 42, 634-641.
Zima, B., Bussing, R., et al. (1999). Psychotropic medication use
among children in foster care: relationship to severe psychiatric disorders. American Journal of Public Health, 89(11), 1732-1735.
Zito, J., Safer, D., et al. (2008). Psychotropic medication patterns
among youth in foster care. Pediatrics, 121(1), 157-163.
Gastroparesis -- This condition occurs when the rate of the electrical wave slows and the stomach contracts less frequently. Now the food just lays in the stomach relying on acid and digestive enzymes to break down the food and on gravity to empty the stomach. There are a number of causes for this condition: Diabetes is the most common known cause. Adrenal and thyroid gland problems can a
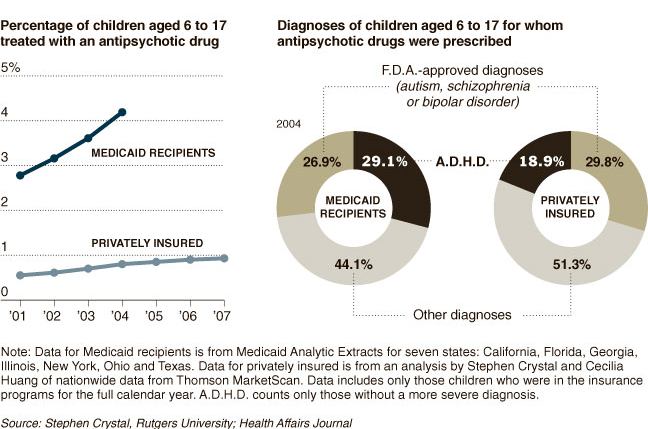 As cited in NYT (12/11/2009): Crystal et al, 2009
Use by Children in Foster Care
As cited in NYT (12/11/2009): Crystal et al, 2009
Use by Children in Foster Care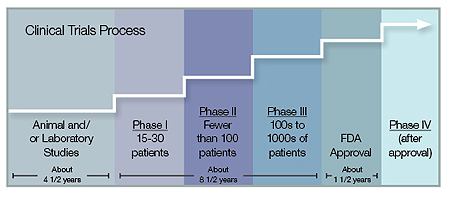 Limited Information about Meds in Children
Phase I: What are safe doses and common side effects?
Phase III: Is the drug better than standard care? (often ‘placebo’)
Phase IV: What else can we learn from post-marketing studies about medication risks, benefits, and optimal use?
Congress to Begin Investigation into SSI for
Limited Information about Meds in Children
Phase I: What are safe doses and common side effects?
Phase III: Is the drug better than standard care? (often ‘placebo’)
Phase IV: What else can we learn from post-marketing studies about medication risks, benefits, and optimal use?
Congress to Begin Investigation into SSI for