Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Doi:10.1016/j.metabol.2003.10.007
Influence of Resistance Exercise Training on Glucose Control in Women With Type 2 Diabetes
L.M. Fenicchia, J.A. Kanaley, J.L. Azevedo Jr, C.S. Miller, R.S. Weinstock, R.L. Carhart, and L.L. Ploutz-Snyder
The objective of the study was to evaluate the effects of acute and chronic resistance training on glucose and insulin responses to a glucose load in women with type 2 diabetes. Subjects consisted of type 2 diabetic women (n ؍ 7) and age-matched controls (n ؍ 8) with normal glucose tolerance. All subjects participated in 3 oral glucose tolerance tests: pretraining, 12 to 24 hours after the first exercise session (acute) and 60 to 72 hours after the final training session (chronic). Exercise training consisted of a whole body resistance exercise program using weight-lifting machines 3 days per week for 6 weeks. Resistance training was effective in increasing strength of all muscle groups in all subjects. Integrated glucose concentration expressed as area under the curve (AUC) was 3,355.0 ؎ 324.6 mmol/L ⅐ min pretraining, improved significantly (P < .01) after the acute bout of exercise (2,868 ؎ 324.0 mmol/L ⅐ min), but was not improved with chronic training (3,206.0 ؎ 337.0 mmol/L ⅐ min) in diabetic subjects. A similar pattern of significance was observed with peak glucose concentration (pre: 20.2 ؎1.4 mmol/L; acute: 17.2 ؎ 1.7 mmol/L; chronic: 19.9 ؎ 1.7 mmol/L). There were no significant changes in insulin concentrations after any exercise bout in the diabetic subjects. There were no changes in glucose or insulin levels in control subjects. An acute bout of resistance exercise was effective in improving integrated glucose concentration, including reducing peak glucose concentrations in women with type 2 diabetes, but not age-matched controls. There were no significant changes in insulin concentrations for either group. Resistance exercise offers an alternative to aerobic exercise for improving glucose control in diabetic patients. To realize optimal glucose control benefits, individuals must follow a regular schedule that includes daily exercise. 2004 Elsevier Inc. All rights reserved. IT IS WELL KNOWN that muscle contraction increases concentration are greater at 12 hours than 72 hours after a bout
glucose uptake in skeletal muscle.1-5 This, in part, forms
of aerobic exercise.13 Perhaps even more relevant is the finding
the basis for recommending exercise for individuals with type
that improvements in glycosylated hemoglobin in diabetic sub-
2 diabetes. Most research studies have investigated the effects
jects is not related to initial maximal oxygen consumption or
of aerobic types of exercise on integrated glucose concentration
improvement in oxygen consumption and thus is not related to
in diabetic patients, because aerobic exercise utilizes large
overall aerobic fitness level. Detraining studies also support the
muscle groups for extended periods of time. However, resis-
notion that improvements in glucose metabolism may be the
tance exercise may provide an equally high, or higher, recruit-
result of repeated acute effects instead of chronic training as
ment of muscle mass over a similar period of time. In fact, a
rapid deterioration of glucose tolerance occurs following the
few studies have shown the benefits of resistance exercise on
cessation of an aerobic training program even though changes
glucose control in individuals with type 2 diabetes or impaired
in maximal oxygen consumption or muscle enzyme profiles
glucose tolerance, and such improvements are of similar mag-
associated with improved fitness persist for weeks.14 Resistanceexercise has not been as thoroughly studied; it is possible that
nitude as seen with aerobic exercise.6,7 Furthermore, it has been
an isolated bout of resistance exercise may be effective at
shown that a whole body resistance training program involving
improving integrated glucose concentration in type 2 diabetic
repeated muscle contractions of the upper and lower body
subjects even in the absence of sustained effects after a chronic
enhances insulin response in healthy individuals.8-10 A single
training program. The effects of an acute bout of resistance
bout of resistance training can significantly enhance insulin
training compared with the effects of chronic resistance train-
clearance in young type 2 diabetics and controls for up to 18
ing in women with type 2 diabetes have not been evaluated thus
far. Therefore, the purpose of this study was to compare the
There has been some controversy regarding whether the
effects of acute and chronic resistance training on integrated
exercise-induced benefits in glucose and insulin control are a
glucose concentration and the insulin response to a glucose
result of multiple single bouts of exercise or whether there is a
load in healthy women and age-matched women with type 2
chronic training benefit.12 Improvements in integrated glucose
From the Department of Exercise Science, Syracuse University,Syracuse; Department of Medicine, State University of New YorkUpstate Medical University, Syracuse; and the VA Medical Center,
Females with type 2 diabetes and age- and height-matched control
women were studied; their descriptive statistics are shown in Table 1. Submitted July 8, 2002; accepted October 10, 2003.
Diabetic subjects had significantly greater body mass, fat mass, fat-free
Supported by the NordicTrack Company.
mass, percent fat, sagittal diameter, and waist circumference than
Address reprint requests to L.L. Ploutz-Snyder, PhD, Exercise Sci-
control women (p Ͻ .05). Four women were premenopausal. All
ence, Rm 201 Womens Building, Syracuse University, Syracuse, NY
subjects provided informed written consent, and the study was ap-
proved by the Institutional Review Boards of Syracuse University and
2004 Elsevier Inc. All rights reserved.
SUNY Upstate Medical University. Subjects were included if they
were not currently and had not participated in resistance training or
aerobic exercise for the previous 6 months. Subjects were defined as
Metabolism, Vol 53, No 3 (March), 2004: pp 284-289
Table 1. Physical Characteristics of the Diabetic and Control
follicular phase (days 1 to 14) of the menstrual cycle in the premeno-
Women Before (pre) and After Six Weeks of Training (post)
pausal women, because the menstrual cycle can affect glucose toler-ance in women.16 A catheter with a 3-way stopcock for blood sampling
was inserted into the antecubital vein; patency was maintained with a
saline flush. The subjects remained seated during the remainder of the
test. A 5-mL baseline blood sample was taken and then a 75-g glucose
drink (Trutol; Custom Laboratories, Baltimore, MD) was administered.
Additional 5-mL blood samples were taken 30, 60, 90, 120, 150, 180,
210, and 240 minutes after consumption of the glucose load. Familiarization Sessions and 3-RM Strength Testing
During the first 2 visits, subjects were oriented to the 9 resistance
exercise machines used for training. The weight pins were removed
from the machines to eliminate resistance during this learning experi-
ence, and the subjects were asked to complete 2 sets of 10 repetitions
on each machine to practice the lifting procedures and breathing
techniques. At the end of the second familiarization visit, 3-RM in-
structions were given,and the 3-RM was estimated on each machine.
*P Ͻ .01 v control; †P Ͻ .05 v control; ‡P Ͻ .01 v pretraining.
On the third familiarization visit, 3-RM evaluated and recorded foreach of the 9 exercises. The 3-RM was used to establish the startingweight for each exercise during training and to document the effec-
having diabetes according to the criteria in the Report of the Expert
tiveness of training. 3-RM is defined as the heaviest weight that a
Committee on the Diagnosis and Classification of Diabetes Mellitus.15
subject can lift through a full range of motion lift 3 times in a row. It
Subjects were excluded if they took medications known to influence
is measured by beginning at a moderate load and increasing the weight
metabolism or total body water (eg, insulin, diuretics, cholesterol-
in 1 kg increments until the subject cannot complete 3 repetitions.
lowering agents, antidepressents, etc) Type 2 diabetes subjects wereincluded if they were taking oral glycemic control medications, but no
changes in any medications were made during the study. Two individ-
Subjects performed supervised weight training exercises 3 noncon-
uals taking glipizide (sulfonylurea), 2 taking troglitazone (thiazo-
secutive days per week for 6 weeks, each session lasting approximately
lidinedione), and 1 taking metformin HCl enrolled in the study. Self-
50 minutes. The weight-training program consisted of 3 sets of 8 to 12
reported chronic alcohol users or smokers were not included in the
repetitions to failure for 8 resistance-type exercises, as well as 3 sets of
study. Additional exclusion criteria for this study were symptomatic
15 abdominal crunches. The 8 exercises performed were chest press,
coronary artery disease, congestive heart failure, peripheral vascular
shoulder press, lat pulldown, leg curl, leg extension, leg press, and
disease, significant hypertension (Ͼ180/100 at rest), renal, hepatic,
triceps extension, all performed on Universal equipment and biceps
pulmonary, adrenal or pituitary disease, or untreated hypo- or hyper-
curls performed using free weights. A 1.5-minute rest was given in
thyroidism or recent orthopedic injury.
between sets to keep subjects’ heart rates down, avoiding a possible
aerobic training effect. The starting weights for each exercise weredetermined as 80% of the subject’s 3-RM. Whenever subjects were
Females with type 2 diabetes and females with normal glucose
able to perform 12 repetitions with proper form, the weight was
tolerance participated in a resistance training program to study the
increased by 5 pounds. Verbal encouragement was given by the exer-
acute and chronic effects of resistance training on changes in integrated
cise supervisor to ensure that the exercises were performed to fatigue
glucose concentration and plasma insulin levels after a glucose load.
while maintaining proper lifting technique.
Responses to a single training session were compared with changesafter chronic training. The type 2 diabetes subjects and controls under-
went the same testing protocol. On the first visit, body composition,
Body composition analysis was performed both pretraining and
height, weight, waist, and sagittal diameter were measured and a
following 6 weeks of resistance training to evaluate changes in lean and
pretraining oral glucose tolerance test (OGTT) was administered. On
fat mass. Body composition was measured in the postabsorptive state
the subsequent 2 visits, subjects were familiarized with the resistance
utilizing a Quantum Bioelectrical Impedance Analysis Machine
exercises used for the training program. After familiarization, a pre-
(BIA101Q; RJL Systems, Clinton Twp, MI).
training 3-repetition maximum strength test (3-RM) was performed foreach exercise. The subjects then participated in resistance training 3
times per week for 6 weeks. A second OGTT was performed 12 to 24hours after the first exercise session (acute) to assess the acute effects
Blood samples were centrifuged for 15 minutes at 2,300 rpm and the
of resistance training on integrated glucose concentration and plasma
serum frozen at Ϫ70°C for later analyses of insulin and glucose. Insulin
insulin levels. To assess the chronic effects of the training program, the
levels were determined using a radioimmunoassay kit (Nichols Diag-
final OGTT was administered 60 to 72 hours after the last training
nostic, San Juan Capistrano, CA), and the glucose content of the blood
session (chronic) to exclude the acute effects of the last training
was measured by the glucose oxidase method (Sigma Diagnostics, St
session. The 3-RM strength test and anthropometric measurements
Louis, MO). For both assays, serum samples were analyzed in dupli-
were repeated posttraining to document changes in strength and body
cate. Pretraining, acute, and chronic samples from an individual subject
were batched and analyzed using the same assay.
All OGTTs were performed following a 12-hour period of fasting
A 2-way analysis of variance (ANOVA) was used to evaluate
and abstention from oral glycemic control medications and during the
treatment effects (pretraining, acute, chronic) and group differences
After the 6-week training program, lean body mass increased
significantly (P Ͻ .01) in the control group, while fat massdecreased significantly in the diabetic group (P Ͻ .01), how-ever, the fat loss was not significantly related to improvementsin glucose AUC (r ϭ .3, P Ͼ .05). There were no othersignificant changes observed, including no changes in totalbody mass (Table 1).
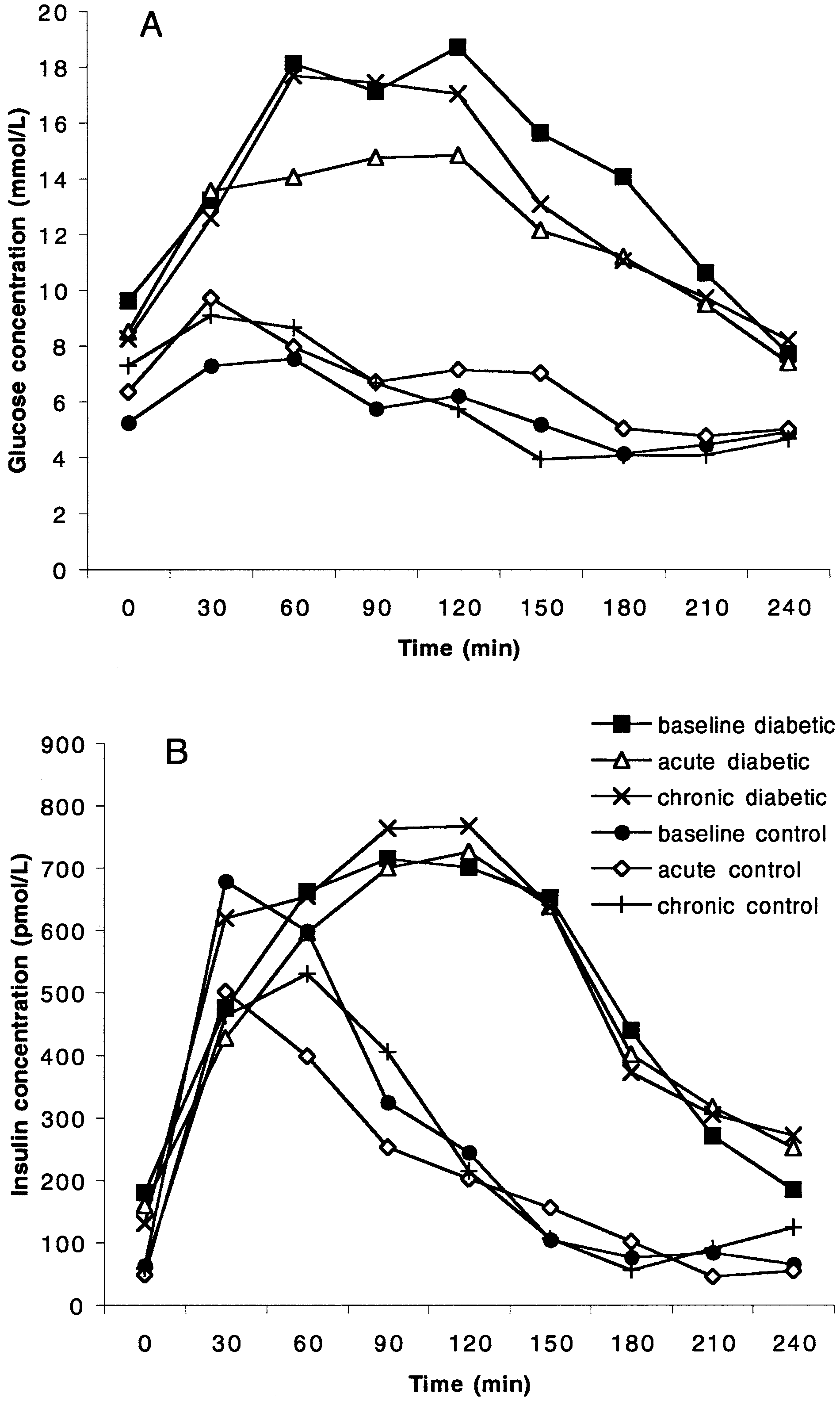
The pattern of glucose responses to the 75g-glucose load is
shown in Fig 2A. At all time points, the diabetic group hadhigher glucose concentrations than the control group. The pre-training fasting glucose concentrations were significantlyhigher in the diabetic group (9.1 Ϯ 1.3 mmol/L) than thecontrol group (5.3 Ϯ 0.7 mmol/L, P Ͻ .05) (time ϭ 0, Fig 2A). Within each subject group, there were no differences among thefasting glucose values (baseline, acute, chronic). The standard
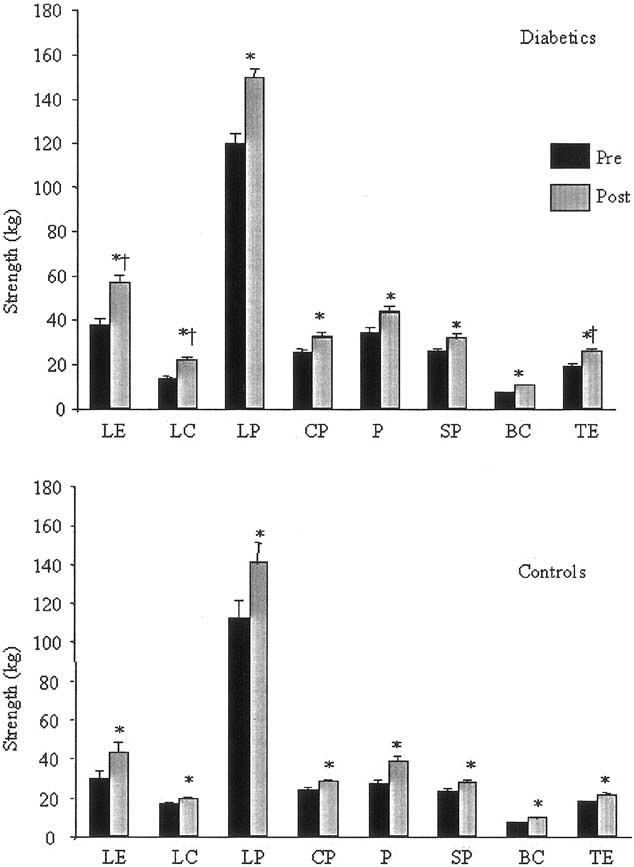
Strength gains for each exercise before and after 6 weeks of training. LE, leg extension; P, pulldown; LC, leg curl; SP, shoulder press; LP, leg press; BC, bicep curl; CP, chest press; TE, tricep exten- sion. Means ؎ SE. *P < .01 v pretraining, †P < .05 diabetics greater improvement than controls, n ؍ 7 diabetics and 8 controls.
(control, diabetic) on fasting glucose and insulin concentrations, peakconcentrations, and 4-hour area under the curve (AUC). Group (dia-betic, control) and treatment (pretraining, posttraining) differences re-lated to body composition and strength gains were also analyzed witha 2-way ANOVA. Significant differences were analyzed using post hocanalyses. Significance was set at P Ͻ .05, and data were presented asmean Ϯ SE. All data were analyzed using Super ANOVA statisticalsoftware (v 1.11, Abacus Concepts, Berkeley, CA). All variables wereexamined for the assumption of normal distribution, and all but 2variables followed a normal distribution (no statistically significantskewness or kurtosis). The fasting values for insulin and glucosefollowed a relatively normal distribution, but had some skewness andkurtosis due to 1 outlier. Because ANOVA is very robust to the normaldistribution assumption, we chose to retain the fasting values of the1-outlier subject.
All subjects, control and diabetic, showed significant
strength increases ranging from 19% to 57% in all exercises(P Ͻ .01) (Fig 1). Diabetic subjects showed significantly
(A) Mean glucose and (B) insulin concentrations over all
greater increases than controls on 3 exercises (leg extension,
time points during OGTT for controls and diabetics, n ؍ 7 diabetics
leg curl, and triceps extension) (P Ͻ .05). and 8 controls.
Before training, fasting insulin concentrations were signifi-
cantly higher in the diabetic group than the control group (P Ͻ.01) (time ϭ 0, Fig 2B). The fasting and postglucose insulinconcentrations are shown in Fig 2B. The insulin concentrationsbegan to rapidly decline 30 to 60 minutes postglucose load inthe control group, while peak insulin concentrations were de-layed and remained elevated for at least 120 minutes in thediabetes group. The peak (highest obtained during the OGTT)values were not significantly different among groups or condi-tions (Fig 5B). There was a group difference in the 4-hour AUCduring the OGTT in the diabetic group (P Ͻ .05) (Fig 5A). There were no significant changes in insulin concentrationsafter acute or chronic exercise in either group.
The most important finding was that integrated glucose con-
centration was improved 12 to 24 hours after just 1 session ofresistance exercise in the absence of any chronic training ef-fects. This is consistent with what has been observed foraerobic exercise. For example, Schneider et al13 showed thatplasma glucose levels were significantly lower at 12 hours than72 hours after aerobic exercise in type 2 diabetic men.
Some previous studies involving strength training and glu-
cose control have also shown improved integrated glucoseconcentration with strength training,6,7 whereas in other stud-ies, integrated glucose concentration did not change.8-11 Thedisparities in effects on glucose tolerance with strength training
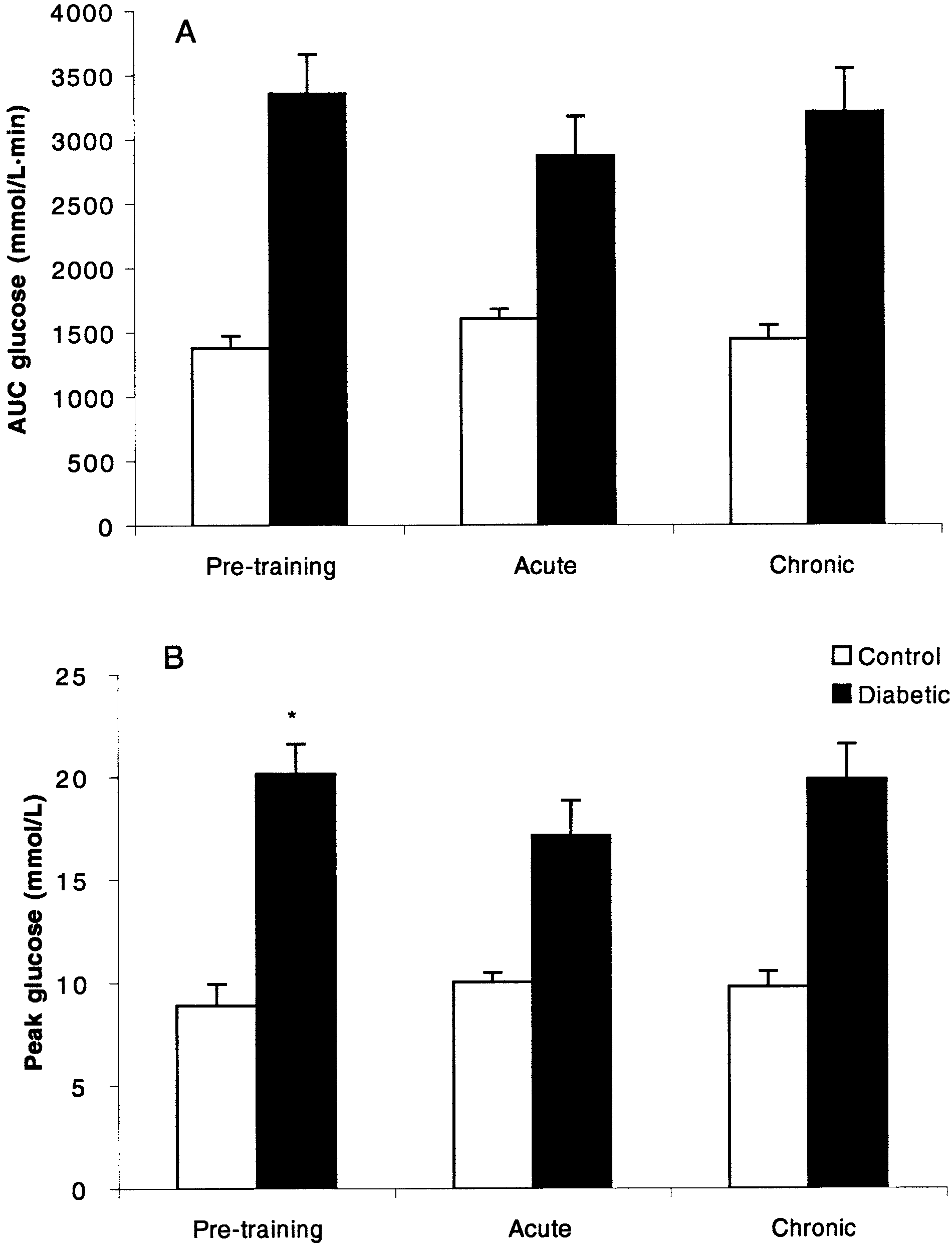
Comparison of effects of pretraining, acute training, and
may relate to the different populations studied. The present
chronic training on glucose concentration (A) 4-hour area under the
study examined middle-aged obese women with type 2 diabetes
curve and (B) peak glucose, which is the highest glucose value reported during the OGTT. Means
who had large postglucose load glycemic excursions with de-
؎ SE. *P < .01 v controls, †P < .01 v pretraining and P < .05 v chronic, ^P < .05 v pretraining and
layed inadequate insulin responses. In previous studies involv-
chronic, n ؍ 7 diabetics and 8 controls.
ing glucose tolerance and strength or aerobic training, individ-uals with higher initial glucose levels also showed more
glucose load resulted in significantly higher peak glucose con-centrations (peak indicates the highest glucose value obtainedduring the OGTT) (P Ͻ .01) and 4-hour AUC (P Ͻ .01) in thediabetic group compared with the control group (Fig 3A). Asignificantly improved integrated glucose concentration (P Ͻ.01) was observed in the diabetic group after the acute bout ofexercise (AUC: 2,868 Ϯ 324.0 mmol/L ⅐ min) compared withpretraining values (3,355.0 Ϯ 324.6 mmol/L ⅐ min), but signif-icant changes after the chronic training were not observed(3,206.0 Ϯ 337.0 mmol/L ⅐ min). A significant decrease wasalso shown in mean peak glucose concentration (pre: 20.2 Ϯ1.4 mmol/L; acute: 17.2 Ϯ 1.7 mmol/L, P Ͻ .05; chronic:19.9 Ϯ 1.7 mmol/L, P Ͻ .05). Glucose concentrations did notchange across time with resistance exercise in the controlgroup. The change in integrated glucose concentration inducedby a single bout of resistance exercise was related to the initialglucose AUC (r ϭ .77, P Ͻ .01) when the whole population isconsidered. Upon further analysis, this relationship was stron-gest among the control subjects (r ϭ .68, P ϭ .06) comparedwith the diabetic subjects (r ϭ .03, P ϭ .48). Generally, thegreater the initial hyperglycemia, the greater the improvement
Relationship between initial glucose AUC and change fol-
with resistance exercises regardless of group (Fig 4). There was
lowing a single acute bout of resistance exercise. Control subjects, E
no significant relationship between glucose AUC before and
and dashed lines; diabetic subjects, F and dotted lines; solid line,
after chronic training (P Ͼ .05). regression line for the whole population.
studies except for one,11 training ranged from 10 to 20 weeksin length, which suggests that longer time periods may berequired to impact insulin levels. It is also possible that theeffects of both acute and especially chronic exercise may beinfluenced by the oral hypoglycemic medications of patients. Inour study and most exercise studies, medications are heteroge-neous for the treatment of diabetes, and because some actperipherally, it is possible that the family of medication useddoes influence the responses to exercise.
It has been shown that the period after aerobic exercise is
characterized by increased insulin sensitivity.19 Our data sug-gest this also applies to resistance exercise; although our datapreclude identification of the precise mechanism; several mech-anisms have been studied by others.19 These include alteredglucose transport,20 improved glucose disposal to restore mus-cle glycogen,21 decreased hepatic glucose output,22 or the un-likely, but possible, explanation that there is slower intestinalabsorption of carbohydrate.
In summary, our data indicate that an acute bout of resistance
exercise is sufficient to improve whole body integrated glucoseconcentration in type 2 diabetic women for at least 24 hourspostexercise. Control subjects with normal glucose controlshowed no exercise-induced changes; in fact, the data show thatthe greatest exercise-induced benefits in glucose control areobserved in the most hyperglycemic subjects (Fig 4). Amongdiabetic subjects, insulin concentrations did not change in thefirst 24 hours after exercise, but glucose concentrations de-creased; we can infer that insulin sensitivity was transiently
Comparison of effects of pretraining, acute training, and
improved during the postexercise period. This may have clin-
chronic training on insulin concentration (A) 4-hour area under the
ical importance, as regular resistance exercise improved glu-
curve and (B) peak insulin, which is the highest insulin value reported
cose control in type 2 diabetics. In addition to improved inte-
during the OGTT. Means ؎ SE. *P < .05 v control, n ؍ 7 diabetics and
grated glucose concentration, resistance training is also known
8 controls.
to offer additional benefits, such as increased strength, main-tained or increased muscle mass even during hypocaloric diet-
dramatic decreases in glucose concentrations with strength
ing, and maintenance of bone density. Furthermore, resistance
training.6,7 It is reasonable to suspect that normal glucose
training may appeal to some patients, particularly the obese,
tolerances in healthy subjects in prior research may preclude
who may have a harder time complying with aerobic exercise
finding a decrease in plasma glucose levels with strength train-
prescriptions due to orthopedic or other limitations. The fre-
ing,8-10,17,18 consistent with Fig 4 in the current study. The
quency and duration of resistance training needed to have a
current study shows a particularly strong relationship between
sustained effect on glycemic control in diabetics will require
initial integrated glucose concentration and exercise-derived
further study, but our data suggest that exercise should be
benefit (r ϭ .77), such that subjects with normal initial glucose
levels showed little response to exercise, and subjects with highinitial glucose levels showed the greatest exercise-induced ben-efit. In our study, a 6-week training program had no effect on
insulin concentrations. Many other studies involving resistance
The technical assistance of Lynn Sauro, Ken Sagendorf, and Robert
training have shown improved insulin levels.6-11 In all of these
Ploutz-Snyder is gratefully acknowledged.
1. Constable SH, Favier RJ, Cartee GD, et al: Muscle glucose
translocation of glucose transporter GLUT4 in skeletal muscle through
transport: interactions of in vitro contractions, insulin, and exercise.
a mechanism distinct from that of insulin. Proc Natl Acad Sci USA
2. Hayashi T, Wojtaszewski JFP, Goodyear LJ: Exercise regulation
5. Wallbert-Henriksson H, Holloszy JO: Activation of glucose
of glucose transport in skeletal muscle. Am J Physiol 273:E1039-
transport in diabetic muscle: Responses to contraction and insulin.
3. Holloszy JO, Hansen PA: Regulation of glucose transport
6. Smutok MA, Reese C, Kokkinos PF, et al: Effects of exercise
into skeletal muscle. Rev Physiol Biochem Pharmacol 128:99-193,
training modality on glucose tolerance in men with abnormal glucose
regulation. Int J Sports Med 15:283-289, 1994
4. Lund S, Holman GD, Schmitz O, et al: Contraction stimulates
7. Smutok MA, Reece C, Kokkinos P, et al: Aerobic vs. strength
training for risk factor intervention in middle-aged men at high risk for
Diabetes Mellitus: Report of the Expert Committee on the Diagnosis
coronary heart disease. Metabolism 42:177-184, 1993
and Classification of Diabetes Mellitus. Diabetes Care 20:1183-1199,
8. Craig BW, Everhart J, Brown R: The influence of high-resistance
training on glucose tolerance in young and elderly subjects. Mech Age
16. Bonen A, Haynes F, Watson-Wright W, et al: Effects of men-
strual cycle on metabolic responses to exercises. J Appl Physiol 55:
9. Miller WJ, Sherman WM, Ivy JL: Effect of strength training on
glucose tolerance and post-glucose insulin response. Med Sci Sports
17. Joseph L, Trappe T, Farrell P, et al: Short-term moderate weight
loss and resistance training do not affect insulin-stimluated gluocse
10. Miller JP, Pratley RE, Goldberg AP, et al: Strength training
disposal in postmenopausal women. Diabetes Care 24:1863-1869, 2001
increases insulin action in healthy 50-65 year old men. J Appl Physiol
18. Ryan AS, Hurlbut DE, Lott ME, et al.: Insulin action after
resistive training in insulin resistant older men and women. J Am
11. Fluckey JD, Hickey MS, Brambrink JK, et al: Effects of resis-
tance exercise on glucose tolerance in normal and glucose-intolerant
19. Goodyear L., Kahn BB: Exercise, glucose transport, and insulin
subjects. J Appl Physiol 77:1087-1092, 1994
sensitivity. Annu Rev Med 49:235-261, 1998
12. Henriksen E: Invited Review: Effects of acute exercise and
20. Kennedy JW, Kirshman MF, Gervino EV, et al: Acute exercise
exercise training on insulin resistance. J Appl Physiol 93:788-796,
induces GLUT4 translocation in skeletal muscle of normal human
subjects and subjects with type 2 diabetes. Diabetes 48:1192-1197,
13. Schneider SH, Amorosa LF, Khachadurian AK, et al: Studies on
the mechanism of improved glucose control during regular exercise in
21. Steensberg A, van Hall G, Keller C, et al: Muscle glycogen
type 2 (non-insulin-dependent) diabetes. Diabetologia 26:355-360,
content and glucose uptake during exercise in humans: Influence of
prior exercise and dietary manipulation. J Physiol 15:273-281, 2002
14. Saltin B, Rowell L: Functional adaptations to physical activity.
22. Segal K, Edano A, Abalos A, et al: Effect of exercise training on
insulin sensitivity and glucose metabolism in lean, obese, and diabetic
15. The Expert Committee on the Diagnosis and Classification of
VANADIUM Atomic number Crystal form Oxidation states Atomic weight Electrical resistivity (20°C) Electronegativity, Pauling CAS number Enthalpy of melting Specific heat (25°C) Boiling point Enthalpy of vaporization Thermal conductivity (25°C) V 3380°C Melting point Ionization potential Specific gravity (20°C) bp/mm (mp) COMPOUNDS C20H18
Yarrow Environmental Solution Yarrow Environmental Solution TM The first version of this Formula, with Yarrow flower essence in a sea salt base, was prepared in 1986 in responseto the Chernobyl nuclear disaster in Europe.The current, enhanced formula, was developed by Patricia Kaminskiin 1995. It features a powerful blend of flower essences and whole plant tinctures in a sea salt base. Pr
 After the 6-week training program, lean body mass increased
significantly (P Ͻ .01) in the control group, while fat massdecreased significantly in the diabetic group (P Ͻ .01), how-ever, the fat loss was not significantly related to improvementsin glucose AUC (r ϭ .3, P Ͼ .05). There were no othersignificant changes observed, including no changes in totalbody mass (Table 1).
After the 6-week training program, lean body mass increased
significantly (P Ͻ .01) in the control group, while fat massdecreased significantly in the diabetic group (P Ͻ .01), how-ever, the fat loss was not significantly related to improvementsin glucose AUC (r ϭ .3, P Ͼ .05). There were no othersignificant changes observed, including no changes in totalbody mass (Table 1).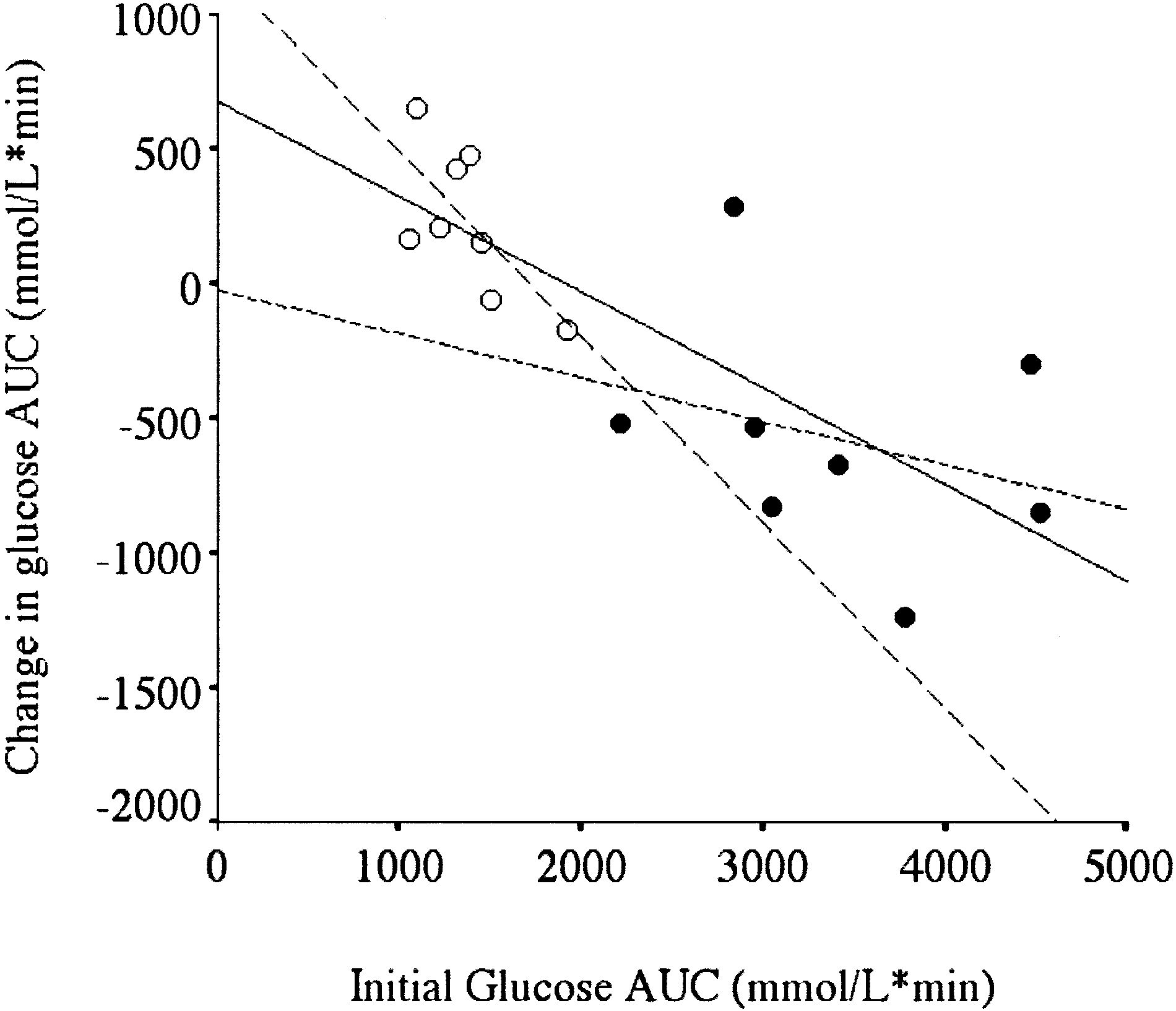
 Before training, fasting insulin concentrations were signifi-
cantly higher in the diabetic group than the control group (P Ͻ.01) (time ϭ 0, Fig 2B). The fasting and postglucose insulinconcentrations are shown in Fig 2B. The insulin concentrationsbegan to rapidly decline 30 to 60 minutes postglucose load inthe control group, while peak insulin concentrations were de-layed and remained elevated for at least 120 minutes in thediabetes group. The peak (highest obtained during the OGTT)values were not significantly different among groups or condi-tions (Fig 5B). There was a group difference in the 4-hour AUCduring the OGTT in the diabetic group (P Ͻ .05) (Fig 5A).
Before training, fasting insulin concentrations were signifi-
cantly higher in the diabetic group than the control group (P Ͻ.01) (time ϭ 0, Fig 2B). The fasting and postglucose insulinconcentrations are shown in Fig 2B. The insulin concentrationsbegan to rapidly decline 30 to 60 minutes postglucose load inthe control group, while peak insulin concentrations were de-layed and remained elevated for at least 120 minutes in thediabetes group. The peak (highest obtained during the OGTT)values were not significantly different among groups or condi-tions (Fig 5B). There was a group difference in the 4-hour AUCduring the OGTT in the diabetic group (P Ͻ .05) (Fig 5A).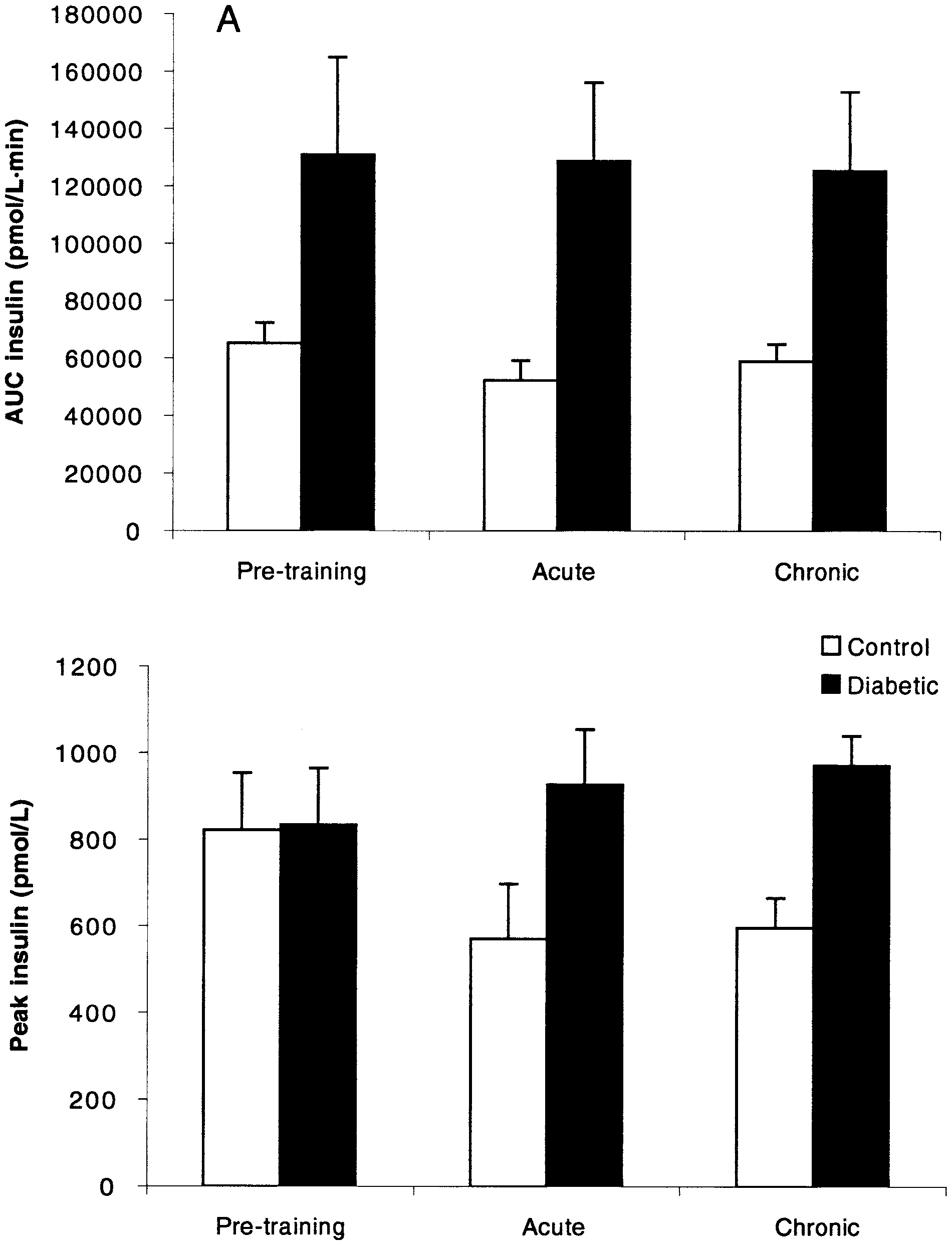 studies except for one,11 training ranged from 10 to 20 weeksin length, which suggests that longer time periods may berequired to impact insulin levels. It is also possible that theeffects of both acute and especially chronic exercise may beinfluenced by the oral hypoglycemic medications of patients. Inour study and most exercise studies, medications are heteroge-neous for the treatment of diabetes, and because some actperipherally, it is possible that the family of medication useddoes influence the responses to exercise.
studies except for one,11 training ranged from 10 to 20 weeksin length, which suggests that longer time periods may berequired to impact insulin levels. It is also possible that theeffects of both acute and especially chronic exercise may beinfluenced by the oral hypoglycemic medications of patients. Inour study and most exercise studies, medications are heteroge-neous for the treatment of diabetes, and because some actperipherally, it is possible that the family of medication useddoes influence the responses to exercise.