Wednesday, December 21 A Message from Cardiology Associates, LLC
Happy Holidays! The December newsletter addresses the cardiac
complications that can occur with chemotherapy. Understanding the
adverse effects of chemotherapy is important for physicians who take
care of cancer survivors. The ability for doctors to assess risk factors,
appropriately monitor for heart disease, and initiate therapy early can
make a big difference in the outcome of patients' lives. About the author
Dr. Stuart Gould sees patients in our Olney office and at Montgomery
General Hospital. Dr Gould completed his post-graduate training at Thomas Jefferson Hospital in
Philadelphia, PA, including an additional year as chief medical resident. He practices consultative
cardiology and has special interests in cardiovascular imaging. Chemotherapy Cardiotoxicity CASE PRESENTATION
• WB is a 68-year-old female with a history of
breast cancer who underwent TAC (Taxotere,
immediately after chemotherapy showed normal
left ventricular function and an ejection fraction of
• She then completed localized radiation therapy
and started on Arimidex. Eighteen months after
completion of her chemotherapy, she presented
to the cardiology office with two weeks of
dyspnea, orthopnea, and weight gain.
• Echocardiogram showed severely depressed left
ventricular function with an ejection fraction of
15-20%. She was admitted to the hospital for
diuresis and started on a heart failure regimen. DISCUSSION
The development of effective therapeutic options for cancer patients has come so far over the
past several decades. Like any treatment, physicians need to be mindful of the harmful side
effects of drugs. Certain chemotherapeutic agents are known to cause cardiac toxicity, but
fortunately cardiac complications are rare. Since the myocardium has limited regenerative
capability, it is susceptible to damage from chemotherapy. Once myocyte injury has occurred,
the heart is less likely to adapt to other stressors such as hypertension and ischemia. The multi-
target theory of heart damage explains why the onset of heart failure may be delayed for some
time after the completion of chemotherapy. Anthracycline agents (i.e. doxorubicin) and non-
anthracycline agents (i.e. trastuzumab) are effective agents used to treat breast cancer, among
other cancers, but also can lead to cardiac complications. The cardiac adverse effects include
arrhythmias, heart failure, ischemia, and pericardial disease. Trastuzumab toxicity appears to be
reversible with cessation of therapy, whereas doxorubicin appears to lead to more permanent
myocardial damage. Many of these cardiac complications can be exacerbated by concomitant
radiation therapy. Physicians adjust timing of drugs, combinations of agents, and cumulative
dosages to minimize cardiac risks. The challenge for doctors is to determine who is at risk for
developing chemotherapy induced cardiotoxicity and how to best monitor these patients.
Heart failure thought to be from anthracycline toxicity can present sub-acutely up to one year
post-termination of chemotherapy. The peak onset of symptoms usually occurs at three months,
but symptomatic heart failure can present as late as one decade after treatment. Risk factors
associated with chemotherapy cardiotoxicity include high cumulative dose, age older than 70,
age less than 18 at initiation of treatment, hypertension, pre-existing coronary artery disease,
female sex, and mediastinal irradiation (TABLE 1). Assessment of cardiac risks factors should be
part of the pre-treatment assessment to limit the chances of cardiac toxicity. Cardiac function
needs to be evaluated before, during, and for some time after treatment. Traditionally,
radionuclide tests with multi- gated acquisition scans (MUGA) have been performed with high
reproducibility. It still may be the preferred method in patients with large body habitus where
echocardiographic images may be limited. Nonetheless, echocardiography overall is the better
test in most patients given its widespread availability and no radiation exposure. It is important
to note that the same noninvasive modality must be used pre- and post- treatment for direct
No official guidelines have been established to help physicians detect early signs of cardiotoxicity
in adults. Some studies have suggested diastolic dysfunction evaluated by echocardiography may
provide an early sign of toxicity. Exercise or dobutamine stress echocardiography has also shown
to be a potential alternative to find subclinical heart failure. Few studies have shown that
measuring troponin or BNP levels may help in early detection of cardiomyopathy, especially in
patients receiving high dose chemotherapy. Without guidelines, surveillance is left to the
physician's discretion. For cancer survivors, subclinical cardiac dysfunction can be detected with
noninvasive imaging (i.e. echocardiography) if mindful surveillance is performed even months to
years after cessation of treatment. This is especially important for pediatric patients who
received cardiotoxic chemotherapy, since the incidence of cardiac complications increases over
Treatment options to prevent toxicity are limited. Dexrazoxane can reduce the free radicals that
are thought to injure myocardial cells. Its use is considered in patients receiving high doses of
anthracyclines, however, it has also been shown to reduce the anticancer effects of
chemotherapeutic agents. A few small trials have shown some promise in administering beta-
blockers or ACE inhibitors prophylactically for their cardio-protective effects. However, more
studies need to be done before it is adopted into routine practice. Once heart failure develops or
there are early signs of left ventricular dysfunction, then the classic heart failure regimen should
commence with early administration of beta-blockers and ACE inhibitors. An ischemic evaluation
should also be done either with stress testing or cardiac catheterization to ensure that the
cardiomyopathy is non-ischemic and truly related to chemotoxicity. Stopping the assumed
offending agent should be weighed against the benefits of continuing medication to treat the
cancer. Patients who are receiving chemotherapy and/or mediastinal radiation therapy may want
to seek the assistance of a cardiologist to help identify cardiac risk factors prior to treatment
and surveillance for cardiotoxicity after treatment. Early detection is paramount with cancer and
cardiac disease in order to be able to provide effective treatments.
Nine months after diagnosis of chemotherapy-induced cardiomyopathy, repeat echocardiogram
showed improvement of left ventricular function with an ejection fraction of 50-55%. Patient is
feeling great, attending cardiac rehabilitation, and volunteering at the hospital. Her current
medical regimen includes Toprol XL 100mg daily, Lisinopril 40mg daily, and Arimidex.
Healy, BR and Swain SM. Clin Cancer Res 2008;14:14-24.
Yeh, ETH, et al. Circ 2004; 109: 3122-3131.
Carver, JR et al. J Clin Oncol 25:3991-4008. Please Join Our Mailing List
We are offering you this monthly newsletter as a way to provide cardiovascular news and
update you on developments within our field. For your convenience, we are distributing our
newsletter via e-mail. Visit our site at ( click the Referring Physician
Newsletter link at the upper left corner of our home page. You will receive an e-Newsletter every
month featuring an article or a case report from one of our physicians and links to other sources
featuring new trends in the field of cardiology.
Our focus will be on real questions and issues that we encounter in our day-to-day medical
practice. In fact, if there is a topic that is of particular interest to you (or a question that is
related to any of our articles) please e-mail your inquiries to our Project Manager, Nazar Snihur
at (Of course, we will not share your e-mail address outside of our
Our Locations Annapolis Cardiology Office Annapolis Vascular Office Bowie Office Irving Street 4800N Kent Island Office K Street Office Olney Office
You have received this message because your email address is part of our electronic mailing list.
If you wish to be removed from our mailing list, please visit our page and enter
your email address for removal from our system.
P O BOX 51283, RAEDENE, 2124 PBO No. 9300531845 OFFICE TELEPHONE: 011.7282292 Chairman: Mrs Sheila Haydock, Tel: 011.488.3548/728.5403 Office Manager/PRO: Mrs Sandra Colombick, Tel: 011.728.2292 Treasurer: Mrs Marlene Karpen, Tel: 011.436.1832 Secretary: Mrs Yvonne Thomé, 011.680.9147 Hello everyone Time is just galloping by and it is almost time for the next ANNUAL GENERAL
Revelation of the amino acid residues essential for ligand-binding selectivity of cytokinin receptors from arabidopsis and maize by computational approach. Institute of Plant Physiology, Russian Academy of Sciences, Botanicheskaya 35, 127276 Moscow, Russia; Department of Chemistry, Lomonosov Moscow State University, Leninskie Gory 1/3, 119991 Moscow, Russia; Cytokinin receptors diffe








 Wednesday, December 21
Wednesday, December 21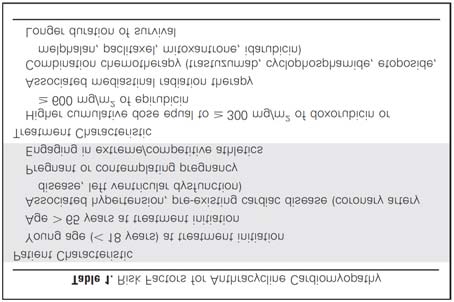 radiation therapy. Physicians adjust timing of drugs, combinations of agents, and cumulative
dosages to minimize cardiac risks. The challenge for doctors is to determine who is at risk for
developing chemotherapy induced cardiotoxicity and how to best monitor these patients.
radiation therapy. Physicians adjust timing of drugs, combinations of agents, and cumulative
dosages to minimize cardiac risks. The challenge for doctors is to determine who is at risk for
developing chemotherapy induced cardiotoxicity and how to best monitor these patients.
 Nine months after diagnosis of chemotherapy-induced cardiomyopathy, repeat echocardiogram
showed improvement of left ventricular function with an ejection fraction of 50-55%. Patient is
feeling great, attending cardiac rehabilitation, and volunteering at the hospital. Her current
medical regimen includes Toprol XL 100mg daily, Lisinopril 40mg daily, and Arimidex.
Nine months after diagnosis of chemotherapy-induced cardiomyopathy, repeat echocardiogram
showed improvement of left ventricular function with an ejection fraction of 50-55%. Patient is
feeling great, attending cardiac rehabilitation, and volunteering at the hospital. Her current
medical regimen includes Toprol XL 100mg daily, Lisinopril 40mg daily, and Arimidex.