Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
260185.qxd
Richard J. Porter ┬Ę R. Hamish McAllister-Williams Allan H. Young
Acute effects of venlafaxine and paroxetine on serotonergic transmission in human volunteers
Received: 11 January 1999 / Final version: 17 May 1999
Abstract Rationale: Antidepressant drugs are thought
receptor function in man (Smith et al. 1991) and has con-
to enhance serotonergic neurotransmission through post-
sistently been shown to be blunted in depressive illness
receptors. This effect is delayed in ani-
(Power and Cowen 1992). This abnormality appears to
mals and may be paralleled by a delay in the onset of a
resolve following successful treatment (Upadhyaya et al.
clinical response in humans. In humans, the growth
1991) and there is evidence that specific antidepressant
hormone (GH) response to intravenous L-tryptophan
healthy volunteers and depressed subjects (Price et al.
and the prolactin response is blunted. Both are therefore
1990). However, the time course of this enhancement
and its relationship to the onset of antidepressant action
tion. Clomipramine has previously been found to en-
hance the GH and prolactin responses to IV L-TRP after
It has been suggested that delay in the onset of clini-
only 2 h. Objective: The purpose of this study was to use
cal response in antidepressant therapy may be due to a
this method to investigate the effects of newer antide-
delay in the increase in transmission through postsynap-
receptors and that this delay is due to the in-
hods: Twelve healthy male volunteers took part in a ran-
fluence of negative feedback mediated by somatoden-
dom order, double blind study, in which 18.75 mg venla-
receptors (Blier and de Montigny 1994).
faxine, 5 mg paroxetine or placebo was administered 3 h
This conflicts, however, with the results of Anderson
before infusion of L-TRP. Results: Pretreatment with
and Cowen (1986) which show that the tricyclic anti-
venlafaxine significantly enhanced the growth hormone
depressant clomipramine increases the GH response to
(GH) response to the infusion compared with pretreat-
IV L-TRP only 2 h after pretreatment in healthy volun-
ment with placebo. There was no significant difference
teers. The acute effects of other antidepressants on neu-
between the GH response following paroxetine com-
roendocrine responses to IV L-TRP have not, however,
pared with placebo or with venlafaxine. Conclusions:
The data suggest enhancement of transmission through
We sought to investigate the acute effects on the GH
agents with more selective profiles than clomipramine:paroxetine, a selective serotonin re-uptake inhibitor and
Key words L-Tryptophan ┬Ę Receptor ┬Ę Serotonin ┬Ę
venlafaxine, a specific serotonin and noradrenaline re-
Growth hormone ┬Ę Prolactin ┬Ę Human volunteer ┬Ę
The GH response to the intravenous infusion of L-TRP
Twelve healthy male volunteers, aged 18ŌĆō40 years (mean 28.1, SD
appears to be a useful measure of postsynaptic 5-HT1A 5.7), gave their informed consent to the study which was approved
by the local Ethics Committee. They had no history of significant
R.J. Porter ┬Ę R.H. McAllister-Williams ┬Ę A.H. Young (Ō£ē)
psychiatric or physical illness and had been on no medication for
Department of Neuroscience and Psychiatry,
University of Newcastle, Royal Victoria Infirmary,
Subjects were tested on three occasions, at least 3 weeks apart,
having taken pretreatment medication at 0700 hours on the morn-
e-mail: A. H.Young@ncl.ac.uk, Fax: 44-191-227-5108
ing of testing. Pretreatment medication consisted of placebo, par-
oxetine 5 mg or venlafaxine 18.75 mg administered orally in abalanced order, double-blind, cross-over design. Following anovernight fast, subjects attended the research laboratory at0900 hours, when an intravenous cannula was inserted. This waskept patent with heparinised saline. Subjects fasted throughout theexperiment, remained semi-supine and were not allowed to sleep. After 1 h, an infusion of L-TRP (in aqueous solution 10 g/l) wasgiven, at a dose of 100 mg/kg, over 25 min. Blood samples weretaken every 15 min from 30 min before the infusion (ŌĆō30 min,ŌĆō15 min and time 0) and every 15 min from 5 min until 95 min af-ter completion of the infusion (+5 min, +20 min etc.).
Blood samples were taken into EDTA tubes and centrifuged to re-move plasma. This was stored at ŌĆō20┬░C. Plasma was also ultra-fil-tered and stored until assay. Samples were analysed for prolactin,GH and cortisol by standard radioimmunoassay. Free TRP was
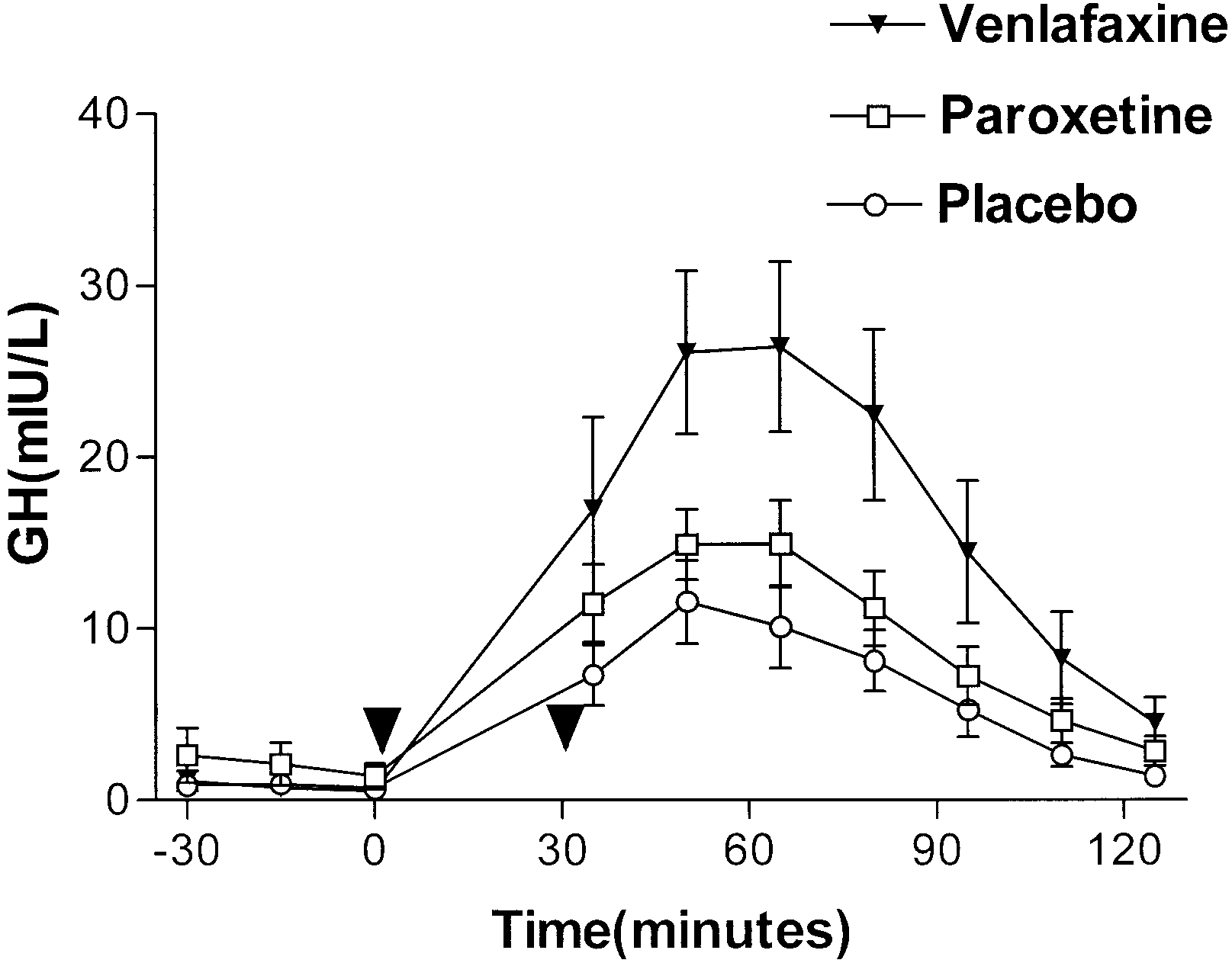
Fig. 1 Effect of pretreatment with paroxetine or venlafaxine or
measured using high performance liquid chromatography (Mar-
placebo on GH response to IV infusion of L-TRP. GH levels
shall et al. 1987). Intra- and inter-assay coefficients of variation
(mIU/l) are plotted as mean┬▒SEM against time. The time of the
for prolactin were 5.7% and 6.4%, respectively, for GH 2.6% and
infusion is indicated by bold arrows. Ō¢╝ Venlafaxine, Ō¢Ā paroxe-
7.4% and free TRP 3.4%, 4.4% and total TRP 3.3% and 4.4%.
and data are therefore missing for this trial. Data fromthis subject are included in the post hoc comparison of
SPSS for Windows Release 7 (SPSS, Chicago, Ill., USA) was
paroxetine versus placebo, but not in the repeated mea-
used for statistical analysis. In all cases the Kolmogorov-Smirnovtest was used to exclude any significant departure from a normal
sures ANOVA, in which data from the remaining nine
distribution. The biochemical and hormonal data were analysed
using a two-way repeated measures analysis of variance (AN-OVA), with drug (paroxetine/venlafaxine/placebo) and time aswithin subject variables. The reported P values of all ANOVAsused the Huynh-Feldt correction factor when the sphericity as-
sumption was not met. For clarity, uncorrected degrees of freedomare reported.
One set of data was excluded (venlafaxine trial) because
Hormonal responses were also analysed using the trapezoid ar-
of high baseline GH values (>10 mIU/l), since GH inhib-
ea under the curve (AUC) method. This was measured from theaverage of the three baseline measures taken prior to infusion of
its its own secretion (Checkley 1980). This subjectŌĆÖs
TRP. AUCs and average baseline measures were analysed by one-
baseline GH values after paroxetine and placebo were
way repeated measures ANOVA with drug as a within-subjects
within accepted limits. ANOVA is therefore reported on
factor. Both AUCs and baselines were then analysed for three sep-
data from eight subjects. ANOVA showed a significant
arate comparisons (paroxetine versus placebo, venlafaxine versus
placebo and paroxetine versus venlafaxine) using post-hoc paired
t-tests (two-tailed). These data are quoted as means┬▒SEM.
(F=4.79; df=2,14; P=0.026), a significant drug by timeinteraction (F=2.80; df=18,126; P=0.021) and a signifi-cant effect of time (see Fig. 1 and Table 1). ANOVA of
AUCs showed a significant effect of drug (F=0.038;df=2,14; P=0.038). Post-hoc analysis of AUC measures
Two subjects failed to complete the second trial because
showed a significant difference between venlafaxine and
of intolerance of side effects (nausea and vomiting) and
placebo (venlafaxine 1676┬▒338; placebo 598┬▒146; t=
because the analysis was within subjects the data from
2.71; df=1,7; P=0.030; 95% CI 138-2019) but no signifi-
the first trial was not used (order of administration ŌĆō par-
cant difference between AUC for paroxetine versus pla-
oxetine/venlafaxine and venlafaxine/paroxetine). One
cebo (paroxetine 786┬▒214; placebo 600┬▒117; t=0.64;
subject did not complete the third trial, when venlafaxine
df=1,9; P=0.537; 95% CI-469-842) or venlafaxine ver-
had been administered, (paroxetine/placebo/venlafaxine)
sus paroxetine (venlafaxine 1676┬▒338; paroxetine 961┬▒
Table 1 Effects of venlafaxine, paroxetine and placebo pretreatment on responses to L-TRP infusion: summary of analysis of variance results. Significant findings are shown in bold Table 2 Effect of pretreatment with venlafaxine and paroxetine
of missing data for two subjects from the venlafaxine arm of the
on mean baseline measures and responses (calculated as trapezoid
study, paired t-tests for comparisons with venlafaxine used mean
area under the curve) to L-TRP infusion for all subjects. Because
AUCs which were different from those given in the table
Table 2 for mean values). There was no effect of drug onmean baseline values (F=0.59; df=2,16; P=0.540).
The main finding of the study is that pretreatment with18.75 mg venlafaxine 3 h before infusion, significantlyenhanced the GH response to infusion of L-TRP com-pared with placebo. There was no significant effect ofparoxetine compared with placebo and no significant ef-fect of either drug on prolactin responses.
The GH response to L-TRP has been shown to be at-
1991). Although pindolol has ╬▓-antagonistic properties
Fig. 2 Effect of pretreatment with paroxetine or venlafaxine or
in dynamic tests of noradrenergic function (Aellig 1976),
placebo on prolactin response to IV infusion of L-TRP. Prolactin
propranolol, a ╬▓-antagonist which has a much lower af-
levels (mIU/l) are plotted as mean┬▒SEM against time. The dura-
tion of the infusion is indicated by bold arrows. Ō¢╝ Venlafaxine,
increases rather than decreases the GH response to
L-TRP (Upadhyaya et al. 1990). This suggests that theeffect of pindolol in inhibiting the GH response to L-TRPis not mediated via ╬▓-adrenoceptor blockade but proba-
227; t=1.75; df=1,9; P=0.123; 95% CI ŌĆō1681ŌĆō250) (see
Table 2 ). ANOVA showed no effect of drug on mean
sponse was not attenuated by the non-selective 5-HT an-
baseline values (F=0.29; df=2,14; P=0.653).
tagonist metergoline (McCance et al. 1987). The expla-nation for this may lie in a relative lack of effective an-tagonism of 5-HT
been demonstrated in functional studies in animals(Koenig et al. 1987). These findings therefore support a
ANOVA showed no significant effects of drug or signifi-
cant drug by time interaction, but a significant effect of
time (Fig. 2, Table 1). There was no effect of drug on
There is evidence that the PRL response to L-TRP in-
AUCs (F=2.02; df=2,16; P=0.172) and post-hoc compar-
fusion may have a dopaminergic component (van Praag
ison of AUCs showed no significant differences between
et al. 1987). Pindolol causes markedly less attenuation of
the conditions (see Table 2 for mean values). There was
the PRL response than the GH response to L-TRP (Smith
no effect of drug on mean baseline values (F=0.66;
et al. 1991). L-TRP competes with tyramine for transport
across the blood-brain barrier (Wurtman 1982) and mayreduce dopamine synthesis by reducing brain tyramine. This is supported by evidence that an intravenous infu-
sion of 5 g L-TRP causes a reduction in post probenecidcerebrospinal fluid (CSF) concentrations of the dopa-
ANOVA showed a significant effect of time but no drug
mine metabolite homovanillic acid (HVA) (van Praag et
effect or drug by time interaction (see Table 1). There
al. 1987). The PRL response to L-TRP may therefore be
was no effect of drug on AUCs (F=0.36; df=2,16;
mediated in part by a reduction in dopamine synthesis,
P=0.625) and post-hoc comparison of AUCs showed no
which releases PRL secretion from tonic inhibition by
significant difference between the three conditions (see
Venlafaxine is a potent serotonin reuptake inhibitor
faxine is unlikely to be a major factor at the dose em-
and a noradrenaline reuptake inhibitor. The active metab-
ployed. It has been suggested that venlafaxine may pro-
olite O-desmethyl-venlafaxine (ODV) has similar prop-
duce an earlier onset of clinical response than other anti-
erties and both are weak dopamine reuptake inhibitors.
depressants (Montgomery 1995) and that this may relate
(Muth et al. 1991). The time to maximum concentration
to early downregulation of ╬▓b adrenoceptors (Moyer et
of venlafaxine is approximately 2 h and for ODV ap-
al. 1992). However, more recent research suggests that
proximately 4 h (Morton et al. 1995). At 3 h (the time
early ╬▓-adrenoceptor downregulation may only occur in
between administration and infusion in this study) the
the pineal gland, which lacks serotonergic innervation,
concentrations of each could therefore be expected to be
and that generally venlafaxine does not produce this ef-
nearly maximal. Preliminary reports in humans suggest
fect (Nalepa et al. 1998). While venlafaxine is a potent
that at lower doses of venlafaxine (75 mg/day), there is
serotonin re-uptake inhibitor in vivo (Beique et al.
little effect on noradrenergic reuptake (Debonnel et al.
1996), it has comparatively less potency than paroxetine
1998). At the dose used in this study (18.75 mg), norad-
in blocking serotonin reuptake in vitro (Bolden-Watson
renergic reuptake inhibition may not therefore be a sig-
and Richelson 1993). A recent study in rat brain shows a
relatively low binding (2000 times less than paroxetine)
This may also be the case in the study of Anderson
of venlafaxine to the 5-HT transporter. It has been sug-
and Cowen (1986), which demonstrated that the GH re-
gested, therefore, that a different mechanism of function-
sponse to L-tryptophan infusion was enhanced by pre-
al 5-HT re-uptake inhibition may be involved (Beique et
treatment with clomipramine. Clomipramine differs from
al. 1998). This might be important in determining the
venlafaxine in that it does possess anticholinergic and
antihistaminergic properties (Hall and Ogren 1981).
While its metabolite, desmethylclomipramine, is a potent
Both L-tryptophan and L-5-hydroxytryptophan (5-
noradrenaline reuptake inhibitor, clomipramine is not
HTP) have been found to depress raph├® neuron firing in
(Carlsson et al. 1969a, 1969b). At the time of infusion in
animals (Gallager and Aghajanian 1976). Electrophysio-
the Anderson and Cowen study, little desmethylclomip-
logical studies also suggest that acute administration of
ramine would have been present (Jones and Luscombe
SSRIs inhibit firing of serotonergic neurones (Chaput et
1976), suggesting that noradrenergic reuptake inhibition
al. 1986; Haj├│s et al. 1995) and a recent study shows that
would be unlikely to contribute significantly to the re-
this is also the case for venlafaxine (Gartside et al.
1997). However, both 5-HTP (Gartside et al. 1992) and
Paroxetine did not significantly increase either the
antidepressants (Fuller 1994) increase cortical extracel-
GH or prolactin response to IV L-TRP. As discussed, at
lular 5-HT following acute treatment, an increase which
the doses employed, clomipramine (Anderson and
is proportionally smaller in the cortex than in the raph├®
Cowen 1986) and venlafaxine were probably acting pri-
nuclei (Artigas 1993). It could be argued that this is sec-
marily via effects on serotonin reuptake. It would there-
ondary to an unphysiological ŌĆ£spillingŌĆØ of 5HT from in-
fore be expected that paroxetine would have similar ef-
traneuronal stores into the synapse, in the absence of cell
fects. We chose dosages which were 25% of the usual
firing. However, the acute increase in extracellular 5-HT
daily starting dose (paroxetine 20 mg, venlafaxine
seen following treatment with 5-HTP (Gartside et al.
75 mg). In both cases, the starting dose is usually an ef-
1992) and antidepressants (Rutter and Auerbach 1993) is
fective antidepressant dose. A small dose was used be-
cause we were concerned that the side effects of the infu-
2-(di-n-propylamino)tetralin, which shuts down seroto-
sion would be amplified by the pretreatments. In fact,
nin neuronal firing. The rise in extracellular 5-HT fol-
even at the low doses employed, some subjects were un-
lowing 5-HTP also appears to be calcium dependant, fur-
able to tolerate the protocol. Clearly, a significant effect
ther suggesting a dependence upon neuronal firing
of paroxetine might have been seen at higher doses. In
(Gartside et al. 1992). Since L-tryptophan is the precur-
addition, the mean time to peak plasma concentrations of
sor to 5-HTP, we would argue that the response to the in-
paroxetine is 5 h (Holliday and Plosker 1993). Peak plas-
fusion and its enhancement by venlafaxine are not sim-
ma levels were therefore probably not reached at the
ply due to leakage of 5-HT and inhibition of its reuptake.
time of infusion. It is notable that the GH response to IV
Our results suggest that venlafaxine, in common with
L-TRP following venlafaxine was not significantly great-
clomipramine, enhances transmission through postsyn-
er when directly compared with that following paroxe-
receptors after only 3 h. Whether this effect
tine. Using a larger number of subjects, a significant en-
in humans is specific to these drugs, or occurs with other
hancement by paroxetine compared with placebo or pos-
classes of antidepressants and what is the exact mecha-
sibly of venlafaxine compared with paroxetine, may
nism by which this occurs, is unclear at present.
The finding of a significant enhancement with venla-
Acknowledgements This study was supported by a grant from
faxine as opposed to paroxetine at roughly equivalent
Wyeth Laboratories. We thank D. Nelson and M. Leitch for bio-chemical measurements.
doses may relate to various putative differences in theirpharmacological and clinical profile. However, we be-lieve that the noradrenaline reuptake inhibition of venla-
Hall H, Ogren S (1981) Effects of antidepressant drugs on differ-
ent receptors in the brain. Eur J Pharmacol 70:393ŌĆō407
Holliday SM, Plosker GL (1993) Paroxetine: a review of its phar-
Aellig WH (1976) ╬▓-Adrenoceptor blocking activity and duration
macology, therapeutic use in depression and therapeutic poten-
of action of pindolol and propranolol in healthy volunteers. Br
tial in diabetic neuropathy. Drugs Aging 3:278ŌĆō299
Hoyer D (1988) Functional correlates of serotonin 5-HT recogni-
Anderson IM, Cowen PJ (1986) Clomipramine enhances prolactin
and growth hormone responses to L-tryptophan. Psychophar-
Jones RL, Luscombe DK (1976) Plasma levels of clomipramine
and its N-desmethyl metabolite following oral clomipramine
Artigas F (1993) 5-HT and antidepressants: new views from mi-
crodialysis studies. Trends Pharmacol Sci 14:262
Koenig JI, Gudelsky GA, Meltzer HY (1987) Stimulation of corti-
Beique JC, de Montigny C, Blier P, Debonnel G (1996) Blockade
costerone and beta-endorphin secretion in the rat by selective
of 5-HT and NE reuptake by venlafaxine: in vivo electrophysi-
5-HT receptor subtype activation. Eur J Pharmacol 137:1ŌĆō8
ological studies in the rat. Soc Neurosci Abstr 22:180
Marshall EF, Kennedy WN, Eccleston D (1987) Whole blood se-
Beique JC, Lavoie N, de Montigny C, Debonnel G (1998) Affini-
rotonin and plasma tryptophan using high-pressure liquid
ties of venlafaxine and various reuptake inhibitors for the sero-
chromatography with electrochemical detection. Biochem
tonin and norepinephrine transporters. Eur J Pharmacol 349:
McCance SL, Cowen PJ, Waller H, Grahame-Smith DG (1987)
Blier P, de Montigny C (1994) Current advances and trends in the
The effects of metergoline on endocrine responses to L-trypto-
treatment of depression. Trends Pharmacol Sci 15:220ŌĆō 226
Bolden-Watson C, Richelson E (1993) Blockade by newly-devel-
Montgomery SA (1995) Rapid onset of action of venlafaxine. Int
oped antidepressants of biogenic amine uptake into rat brain
Morton W, Sonne S, Verga M (1995) Venlafaxine: a structurally
Carlsson A, Corrodi H, Fuxe K, H├Čkfelt T (1969a) Effects of
unique and novel antidepressant. Ann Pharmacother 29:387ŌĆō
some antidepressant drugs on depletion of intraneuronal brain
catecholamine stores caused by 4-alpha-dimethyl-metatyra-
Moyer JA, Andree TH, Haskins JT, Husbands G, Muth EA (1992)
The preclinical pharmacological profile of venlafaxine: a nov-
Carlsson A, Corrodi H, Fuxe K, H├Čkfelt T (1969b) Effect of anti-
el antidepressant agent. Clin Neuropharmacol 15:435B
depressant drugs on the depletion of intraneuronal brain 5-hy-
Muth E, Moyer J, Haskins J, Andree T, Husbands G (1991) Bio-
droxytryptamine stores caused by 4-alpha-dimethyl-metatyra-
chemical, neurophysiological and behavioural effects of Wy-
45233 and other identified metabolites of the antidepressant
Chaput Y, Blier P, de Montigny C (1986) In vivo electrophysiolog-
ical evidence for the regulatory role of autoreceptors on sero-
Nalepa I, Manier DH, Gillespie DD, Rossby SP, Schmidt DE, Sul-
tonergic terminals. J Neurosci 6:2796ŌĆō2801
ser F (1998) Lack of beta adrenoceptor desensitisation in brain
Checkley SA (1980) Neuroendocrine tests of monoamine function
following the dual noradrenalin and serotonin reuptake inhibi-
in man: a review of basic theory and its application to the
tor venlafaxine. Eur Neuropsychopharmacol 8:227ŌĆō232
study of depressive illness. Psychol Med 10:35ŌĆō53
Power AC, Cowen PJ (1992) Neuroendocrine challenge tests: as-
Debonnel G, Blier P, Saint-Andre E, Hebert C, de Montigny C
sessment of 5-HT function in anxiety and depression. Mol As-
(1998) Comparison of the effects of low and high doses of
venlafaxine on serotonin and norepinephrine reuptake process-
Price LH, Charney DS, Delgado PL, Goodman WK, Krystal JH,
es in patients with major depression and healthy volunteers.
Woods SW, Heninger GR (1990) Clinical studies of 5-HT
function using IV L-tryptophan. Prog Neuro-Psychopharmacol
Fuller RW (1994) Uptake inhibitors increase extracellular seroto-
nin concentration measured by brain microdialysis. Life Sci
Smith CE, Ware CJ, Cowen PJ (1991) Pindolol decreases prolactin
and growth hormone responses to intravenous L-tryptophan.
Gallager DW, Aghajanian GK (1976) Inhibition of firing of raphe
neurones by tryptophan and 5-hydroxytryptophan: blockade
Upadhyaya AK, Deakin JF, Pennell I (1990) Hormonal response
by inhibiting serotonin synthesis with Ro-4-4602. Neurophar-
to L-tryptophan infusion: effect of propranolol. Psychoneuro-
Gartside SE, Cowen PJ, Sharp T (1992) Effect of 5-hydroxy-L-
Upadhyaya AK, Pennell I, Cowen PJ, Deakin JF (1991) Blunted
tryptophan on the release of 5-HT in rat hypothalamus in vivo
growth hormone and prolactin responses to L-tryptophan in
as measured by microdialysis. Neuropharmacology 31:9ŌĆō14
depression; a state-dependent abnormality. J Affect Disord
Gartside SE, Umbers V, Sharp T (1997) Inhibition of 5-HT cell
firing in the DRN by non-selective 5-HT reuptake inhibitors:
van Praag HM, Lemus C, Kahn R (1987) Hormonal probes of cen-
tral serotonergic activity: do they really exist? Biol Psychiatry
mechanisms. Psychopharmacology 130:261ŌĆō268
Haj├│s M, Gartside SE, Sharp T (1995) Inhibition of median and
Wurtman RJ (1982) Nutrients that modify brain function. Sci Am
dorsal raph├® neurones following administration of the selective
serotonin reuptake inhibitor paroxetine. Naunyn-Schmiede-bergŌĆÖs Arch Pharmacol 351:624ŌĆō629
Los Actos de Habla, una competencia comunicativa clave para el desarrollo de personas y organizaciones La perspectiva del lenguaje como un g├®nero de acci├│n, nos permite desarrollar competencias relevantes en aspectos claves de nuestras interrelaciones en la empresa, partiendo por la comprensi├│n de la esencia misma de una empresa en t├®rminos de redes de conversaciones para la creaci├
Benefits Checklist Prescription Drug Assistance Programs Ōü« Partnership for Prescription Assistance (www.pparx.com) ’éĘ Eligibility information is entered and available options are generated. ŌüŁ Yes ŌüŁ No Reason________________________________________________________________________________________________________________________________________________________________________________
 oxetine 5 mg or venlafaxine 18.75 mg administered orally in abalanced order, double-blind, cross-over design. Following anovernight fast, subjects attended the research laboratory at0900 hours, when an intravenous cannula was inserted. This waskept patent with heparinised saline. Subjects fasted throughout theexperiment, remained semi-supine and were not allowed to sleep.
oxetine 5 mg or venlafaxine 18.75 mg administered orally in abalanced order, double-blind, cross-over design. Following anovernight fast, subjects attended the research laboratory at0900 hours, when an intravenous cannula was inserted. This waskept patent with heparinised saline. Subjects fasted throughout theexperiment, remained semi-supine and were not allowed to sleep.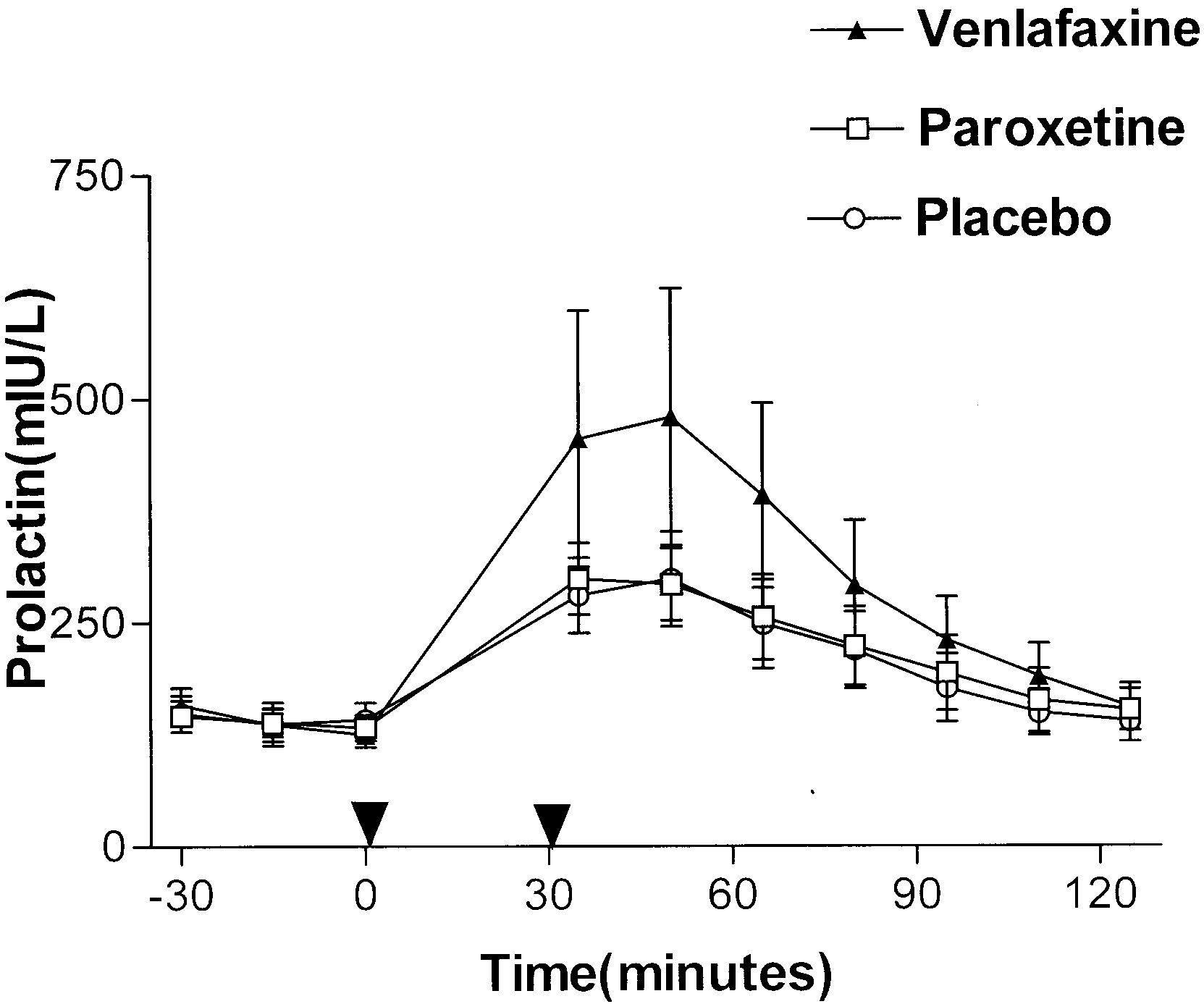 Table 2 Effect of pretreatment with venlafaxine and paroxetine
Table 2 Effect of pretreatment with venlafaxine and paroxetine