Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Impact of sex, age, race, ethnicity and aspirin use on bleeding symptoms in healthy adults
Journal of Thrombosis and Haemostasis, 9: 100–108
Impact of sex, age, race, ethnicity and aspirin use on bleedingsymptoms in healthy adults
A . C . M A U E R , * N . A . K H A Z A N O V , * N . L E V E N K O V A , * S . T I A N , * E . M . B A R B O U R , * C . K H A L I D A , J . N . T O B I N * and B . S . C O L L E R **The Rockefeller University, New York, NY; and Clinical Directors Network, Inc. (CDN), New York, NY, USA
To cite this article: Mauer AC, Khazanov NA, Levenkova N, Tian S, Barbour EM, Khalida C, Tobin JN, Coller BS. Impact of sex, age, race, ethnicity
and aspirin use on bleeding symptoms in healthy adults. J Thromb Haemost 2011; 9: 100–8.
Keywords: bleeding disorders, bleeding history, gender differ-
Summary.Background: Comparing a patientÕs bleeding symp-
toms with those of healthy individuals is an importantcomponent of the diagnosis of bleeding disorders, but little is
known about whether bleeding symptoms in healthy individualsvary by sex, race, ethnicity, age, or aspirin use. Objectives,
Obtaining a detailed bleeding history is an important compo-
Patients/Methods: We developed a comprehensive, ontology-
nent of the medical evaluation to determine whether a person:
backed, Web-based questionnaire to collect bleeding histories
(i) has a bleeding diathesis; (ii) is at increased risk of excessive
from 500 healthy adults. The mean age was 43 years (range 19–
hemorrhage in response to invasive procedures and/or surgery;
86 years), 63% were female, 19% were Hispanic, 37% were
and/or (iii) should undergo laboratory evaluation and/or
African-American, 43% were Caucasian, 8% were Asian, and
referral to a specialist [1–3]. Moreover, correlation of clinical
4% were multiracial. Results: 18 of the 36 symptoms captured
hemorrhage with genetic, biochemical and/or functional data
occurred with < 5% frequency, and 26% of participants
related to platelets or coagulation factors can provide impor-
reported no bleeding symptoms (range 0–19 symptoms).
tant information for a better understanding of the basic
Differences in sex, race, ethnicity, aspirin use and age accounted
mechanisms of hemostasis. However, despite a number of early
for only 6–13% of the variability in symptoms. Although men
attempts to standardize bleeding history questionnaires (re-
reported fewer symptoms than women (median 1 vs. 2,
viewed by Coller and Schneiderman [1]), no generally recog-
P < 0.01), there was no difference when sex-specific questions
nized standards for collecting a bleeding history emerged until
were excluded (median 1 for both men and women, P = 0.50).
recently, when Rodeghiero et al. developed bleeding question-
However, women reported more easy bruising (24% vs. 7%,
naires and scoring systems for the evaluation of patients with
P < 0.01) and venipuncture-related bruising (10% vs. 3%,
von Willebrand disease (VWD). By assigning point values to
P = 0.02). The number of symptoms did not vary by race or
the severity of various bleeding symptoms, they demonstrated
age, but epistaxis was reported more frequently by Caucasians
that a bleeding score is valuable for confirming the diagnosis of
than by African-Americans (29% vs. 18%, P = 0.02), and
VWD [4–6] and predicting the risk of future hemorrhagic
epistaxis frequency decreased with age (odds ratio 0.97 per year,
events in type 1 [5] and type 2B [7] VWD. Several groups have
P < 0.01). Paradoxically, infrequent aspirin users reported
used the Vicenza bleeding score as is or with modifications to
more bruising and heavy menses than frequent users (21% vs.
8%, P = 0.01, and 56% vs. 38%, P = 0.03, respectively).
The value of such approaches depends on comparing the
Conclusions: Our findings provide a contemporaneous and
bleeding histories of affected and healthy individuals. The
comprehensive description of bleeding symptoms in a diverse
literature, however, reports marked variability of hemorrhagic
group of healthy individuals. Our Web-based system is freely
symptoms among apparently healthy individuals (Table 1).
For instance, reported symptom frequencies range from 2% to85% for epistaxis, from 20% to 44% for menorrhagia, from0% to 11% for postoperative bleeding, from 0% to 35% forbleeding after tooth extraction, and from 11% to 61% for
Correspondence: Andreas C. Mauer, 1230 York Ave, Box 309, New
gingival bleeding [11–17]. At present, it is unclear whether these
variations reflect differences in the questionnaires used, the
Tel.: +1 212 327 7633; fax: +1 212 327 7493.
methods of administration, the sex, race, ethnicity, age, or
frequency of use of medications with antiplatelet effects of the
Received 20 August 2010, accepted 5 October 2010
populations sampled, or other factors.
Ó 2010 International Society on Thrombosis and Haemostasis
Bleeding symptoms in healthy individuals 101
Although only women face the hemostatic challenges of
menstruation, pregnancy, and childbirth, there is only limited
information on whether other bleeding symptoms differ
between men and women. We found only a single study,
which was limited to the evaluation of differences in epistaxis
frequency between Caucasians and Asians [18], that assessed
whether individuals of different racial backgrounds experience
bleeding symptoms with different frequencies. As Hispanic
ethnicity is viewed as distinct from race [19], we also searched
for, but did not find, reported differences in bleeding symptoms
between individuals of Hispanic and non-Hispanic ethnicity. Although it is recognized that some bleeding symptoms such as
epistaxis occur more frequently in childhood than adulthood
[1], we could not identify information on whether bleedingsymptoms differ among adults of different ages. Moreover, as
older individuals have had more time to sustain hemorrhagic
symptoms, it is possible that age is an important factor in
interpreting the bleeding history. Aspirin has significant
antiplatelet properties, but the association between aspirin
use and bleeding symptoms in a contemporaneous healthy
population has not been systematically assessed with a
To address these questions, we designed and deployed a
comprehensive, Web-based bleeding history questionnaire in a
study that aimed to: (i) establish the frequencies of bleeding
symptoms in a diverse population of healthy adults; and (ii)
assess whether any symptoms varied by sex, race, ethnicity, age,
The design of the bleeding history phenotyping system we used
has been previously described [20]. The centerpiece is a
comprehensive bleeding history questionnaire that incorpo-
rated elements from a review of the literature, one of the
authorsÕ experience [1], and input from experts in hemostasis,
questionnaire development, epidemiology, and biomedical
informatics. It contains 278 questions covering 25 categories
of bleeding and related covariates, with the latter including
dermatologic lesions, connective tissue disorders, medications,
and family history. To reduce ambiguity in terminology, 168
terms in the questionnaire and ontology were cross-referenced
to the National Library of MedicineÕs Unified Medical
Language System by assigning them the corresponding code
The questionnaire was used to derive a bleeding history
ontology, which is an explicit representation of the relation-
ships among bleeding signs, symptoms, disorders, and treat-
ments. The ontology formalizes the concepts contained in the
questionnaire in an electronic format that facilitates data
analysis, organization, and representation. The ontology is
publicly available in the Bioportal ontology registry (http://
bioportal.bioontology.org/ontologies/40546) to facilitate its
critique by experts in the field and its future updating, as, for
Ó 2010 International Society on Thrombosis and Haemostasis
example, when new therapies for bleeding disorders are
235 individuals were approached and 135 (57%) agreed to
participate. In both settings, after written informed consent was
The questionnaire is administered by a medically trained
obtained, a physician or nurse trained in the use of the
individual using a Web-based program. Studies are assigned a
questionnaire conducted the interview and entered the partic-
site identification code as well as a code to identify the person
ipantÕs responses directly into the database with a personal
administering the questionnaire. To ensure confidentiality,
computer. Personnel conducting the interviews completed a
each respondent is identified by a randomly generated unique
credentialing process that included: (i) observing one of us
personal identification number. Skip patterns were introduced
(ACM) conduct two interviews; (ii) obtaining two histories
into the program to speed questionnaire completion. For
under ACMÕs direct supervision; and (iii) completing a
example, respondents who state that they have never had
checklist of skills. ACM conducted 129 interviews, trained
epistaxis are not asked questions about epistaxis frequency or
research nurses conducted 236 interviews, and CDN PBRN
duration. The program is time-stamped so that the time
staff (CK) conducted 135 interviews at CDN CHCs. All
required to complete the study is captured. Users can log off
questionnaires were administered in English. Participants
and log on as often as they wish, allowing the questionnaire to
received a $20 honorarium for their time. The mean time
be completed in more than one session. To help the person
needed to complete the questionnaire was 33 min (range: 12–
providing the bleeding history to better understand the
questions and give accurate responses, some of the questionsinclude visual aids, for example photographs of petechiae. Data
are stored in a secure, Web-accessible MySQL database. Investigators from other institutions can review all of the
All analyses were performed with PASW 18.0 (PASW,
components of the system, including the database, at http://
Chicago, IL, USA). The questionnaire includes both top-level
screening questions and detailed follow-up questions (e.g. pertaining to the frequency or duration of bleeding symptoms). For this study, 36 top-level questions were selected for detailed
analysis on the basis of their: (i) similarity to questions reported
The study protocol was approved by the institutional review
in the existing literature; (ii) reflecting the presence or absence
boards of both the Rockefeller University and the Clinical
of a bleeding symptom rather than attributes such as the
Directors Network (CDN; http://www.CDNetwork.org), a
frequency, duration or severity of a symptom; and (iii) eliciting
non-profit primary care practice-based research network
dichotomous responses that were suitable for binary logistic
(PBRN) and clinician training organization that conducts
clinical and translational research studies in community
Both intra-rater and inter-rater reliabilities were evaluated.
health centers (CHCs). Bleeding symptoms were obtained
To assess the consistency of responses to these questions by the
from 500 healthy individuals, of whom 365 were seen at
same subject over time (intra-rater reliability), 30 individuals
Rockefeller University and 135 were seen at two separate
were recalled 6–9 months after the questionnaire was initially
CDN-member CHCs (75 at Metropolitan Family Health
administered, and the questionnaire was administered again.
Network, Jersey City, NJ, and 60 at Newark Community
Of the 36 questions analyzed, 36% had complete concordance
Health Center, Newark, NJ). Potential participants were
between the first and second administration, 36% had 90–99%
eligible if they met the following criteria: age ‡ 18 years; self-
concordance, and 28% had concordances that ranged from
assessment as being generally healthy; and self-assessment as
56% to 89%. To assess whether the person administering the
being able to accurately read and answer questions in
questionnaire had any influence on the response, one of us
English. Exclusion criteria included a diagnosis of any
(ACM) reviewed 31 randomly selected audio recordings
bleeding disorder; hepatic or renal disease; malignancy
conducted by other interviewers, and completed a second
requiring treatment within 1 year prior to enrollment; use
questionnaire for each participant based on the recording
of any medications with known anticoagulant or antiplatelet
(inter-rater reliability). The recorded responses were completely
properties other than aspirin or non-steroidal anti-inflamma-
concordant for 30 of the 36 questions, four questions had
tory drugs within 30 days of enrollment; or any other
> 90% concordance, and two questions had 82% concor-
medical or psychological condition that would impair the
dance. An analysis of responses by site of administration
participantÕs ability to accurately respond to questions about
revealed minor differences in a few symptoms, but the analysis
was confounded by the different demographics at the sites and
Participants recruited at Rockefeller were identified through
the relatively small number of individuals reporting the
online and print advertisements seeking healthy volunteers.
symptoms. Thus, no adjustments were made for the site of
Participants recruited through CHCs were patients identified in
the waiting room during routine primary care visits who were
To test whether the prevalence of the 36 bleeding symptoms
willing to complete the interview. At Rockefeller, 372 individ-
differed according to one or more demographic characteris-
uals responded to advertisements and passed telephone
tics, a binary multiple logistic regression model was con-
screening, of which 365 (98%) were enrolled. At the CHCs,
structed for each symptom. For each model, the question
Ó 2010 International Society on Thrombosis and Haemostasis
Bleeding symptoms in healthy individuals 103
response was the dependent variable, and sex, race, ethnicity,
86 years), and 63% of subjects were female. The racial
age and the frequency of aspirin use were the independent
distribution was as follows: 37% African-American, 43%
variables. For each question, individuals who answered ÔdonÕt
Caucasian, 8% Asian, < 1% Pacific Islander, and 4% more
rememberÕ were excluded from analysis. For the aspirin
than one race; 8% preferred not to report race. The ethnic
analysis, ÔfrequentÕ aspirin users were defined as those who
distribution was 19% Hispanic and 80% non-Hispanic; 1%
used aspirin once a week or more often (10%), ÔinfrequentÕ
aspirin users were defined as those who used aspirin less than
The frequencies of the 36 bleeding symptoms analyzed are
once a week (49%), and ÔneverÕ users were defined as those
displayed in Table 3. Symptom frequencies ranged from 0%
who denied using aspirin (39%); 1% of respondents did not
(teething bleeding, hemorrhagic stroke, circumcision bleeding,
remember their frequency of aspirin use. Prior to regression
and umbilical cord bleeding) to 47% (heavy menses). It is of
analysis, multicollinearity among the independent variables
note that 18 of the 36 symptoms were reported by fewer than
was tested with the Spearman rank correlation coefficient for
5% of subjects who responded to the question.
ratio and ordinal variables and CramerÕs V for nominalvariables. From this analysis, Hispanic ethnicity was found to
be correlated with African-American and Caucasian race. Therefore, ethnicity was excluded when race was evaluated as
The total number of symptoms was not normally distributed
an independent variable, and race was excluded when
(Fig. 1). When all symptoms were considered, women
ethnicity was evaluated as an independent variable. Model
reported more bleeding symptoms than men (P < 0.01 by
fit was tested using the chi-squared goodness-of-fit and
Mann–Whitney U-test; Fig. 1A). Men reported a median of
Hosmer–Lemeshow tests [22]. For models with adequate fit,
one symptom (interquartile range [IQR] 0–3) and women
adjusted odds ratios (ORs) were calculated for independent
reported a median of two symptoms (IQR 1–4). However,
variables. For each symptom, the proportion of variance
after removal of sex-specific bleeding symptoms (heavy
explained by the regression model was estimated using the
menses, treatment for heavy menses, bleeding during preg-
Nagelkerke R2 [22]. Differences with P-values < 0.05 were
nancy, bleeding at delivery, postpartum bleeding, and, for
defined as statistically significant. No adjustments for multiple
men, circumcision bleeding), men and women both reported
comparisons were made in these exploratory analyses.
a median of one symptom (IQR 0–3 for both men andwomen, P = 0.50 by Mann–Whitney U-test; Fig. 1B). When individual symptoms were analyzed together by
logistic regression, however, differences by sex were noted
Demographic characteristics are displayed in Table 2. The
(Table 4). Thus, easy bruising was more common among
mean age was 43 years (standard deviation ± 13.8; range 19–
women than among men (24% vs. 7%, OR 4.78, 95%
Table 2 Demographic characteristics by site of enrollment
*For Rockefeller University vs. Community Health Centers. FisherÕs exact test. àT-test. §Chi-square.
Ó 2010 International Society on Thrombosis and Haemostasis
Table 3 Frequencies of selected bleeding symptoms
There was a trend towards more bleeding symptoms in
Caucasians (median 2, IQR 1–3) vs. either African-Americans
(median 1, IQR 0–3) or Asians (median 1, IQR 0–3, P = 0.07
by Kruskal–Wallis test). Epistaxis was less common among
African-Americans than among Caucasians (18% vs. 29%,
OR 0.55, 95% CI 0.34–0.90, P = 0.02), as was bleeding in oraround the eye, which included conjunctival hemorrhage,
retinal hemorrhage, and bleeding behind the eye (3% vs. 10%,
OR 0.29, 95% CI 0.11–0.75, P = 0.01).
Hispanics reported a similar median number of symptoms
(median 2, IQR 0–3) as non-Hispanics (median 2, IQR 0–3,
P = 0.54). When ethnicity was substituted for race as an
independent variable, no symptoms were associated with
Age was not associated with the total number of symptoms
(Spearman r = 0.05, P = 0.24), but the odds of reporting
epistaxis decreased with age (OR 0.97 per year, 95% CI 0.96–
0.99, P < 0.01). Increasing age was also associated with a
higher reported frequency of dark stools (OR 1.02 per year,
95% CI 1.00–1.04, P = 0.02); however, among the 72 indi-
viduals who reported a history of dark stools, 68% had been
told that the change in color was attributable to iron therapy,
and only 6% had been told that the change in color was caused
There was a trend towards an increased median number of
symptoms in infrequent aspirin users (median 2, IQR 1–3) vs.
those who never used aspirin (median 1, IQR 0–3) or who used
it frequently (median 1, IQR 1–2, P = 0.08 by Kruskal–
Wallis test). Easy bruising was more common among infre-
quent than among frequent aspirin users (21% vs. 8%,
OR 4.18, 95% CI 1.39–12.58, P = 0.01), with those who
reported not taking aspirin having an intermediate frequency
(15%). A history of heavy menses was also more common
among infrequent aspirin users than among frequent aspirin
users (56% vs. 38%, OR 3.03, 95% CI 1.25–7.32, P = 0.01),
with those who reported not taking aspirin again having an
*Exact question wording is available at http://ds9.rockefeller.edu/RUBHPSR/Documentation.html. Some questions were contingent
Contribution of sex, race, age and aspirin use to variability
upon previous answers; therefore, not all questions were asked of allrespondents.
For 30 symptoms, no significant associations with sex, race, age
confidence interval [CI] 2.50–9.16, P < 0.01), as was veni-
or aspirin use were identified. The contribution of sex, race, age
puncture bruising (10% vs. 3%, OR 3.04, 95% CI 1.22–7.59,
and aspirin use to the remaining six symptoms, as defined by
Nagelkerke R2, are summarized in Table 4. For instance, the
Ó 2010 International Society on Thrombosis and Haemostasis
Bleeding symptoms in healthy individuals 105
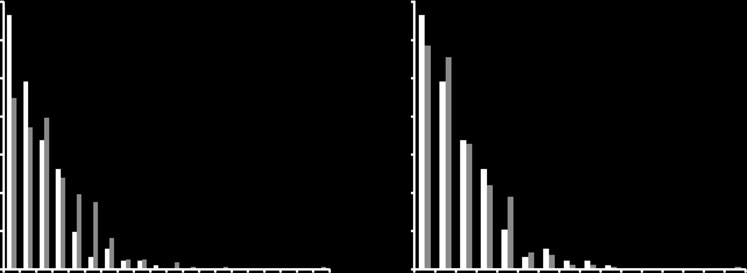
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Number of symptoms, excluding sex-specific symptoms
Fig. 1. Number of bleeding symptoms in men and women. (A) Men reported fewer bleeding symptoms than women (P < 0.01 by Mann–Whitney U-test). (B) When heavy menses, treatment for heavy menses, bleeding during pregnancy, bleeding at delivery, postpartum bleeding and circumcision bleedingwere excluded, men and women reported similar frequencies of bleeding symptoms (P = 0.50 by Mann–Whitney U-test).
Table 4 Results of logistic regression analyses of questions with statistically significant differences in responses by one or more demographic characteristics
*Odds ratio per additional year of age. Odds ratio vs. Caucasian race. àOdds ratio vs. male sex. §Defined as aspirin use less than once per week;odds ratio vs. aspirin use more than once per week.
combined R2 for age and race with regard to epistaxis was 0.08;
established whether applying adjustments for these character-
that is, the two variables accounted for 8% of the observed
istics can improve the diagnostic value of the bleeding history.
variability in epistaxis. Sex, race, age and aspirin use accounted
The frequencies of most bleeding symptoms in our popula-
for only 6–13% of the variability in reported symptoms.
tion were within the ranges previously reported by otherinvestigators (Table 1). For instance, 25% of our respondentsreported epistaxis, as compared with a weighted average of
23% in previous studies, and 18% of our respondents reported
We used a novel questionnaire and Web-based system to
easy bruising, as compared with a weighted average of 20% in
collect comprehensive bleeding histories from 500 healthy
previous studies. Of the 13 symptoms reported in Table 1, nine
individuals. We found that 26% of subjects reported no
symptoms were within 5% of the reported weighted average.
symptoms, and that 18 of the 36 symptoms were reported by
Greater differences were observed for menorrhagia (47% in
fewer than 5% of the subjects. The frequencies of epistaxis,
our study vs. 35% in the literature), tooth extraction bleeding
easy bruising, bruising after venipuncture, heavy menses, dark
(18% vs. 6%), gum bleeding (4% vs. 28%), and hematochezia
stools and ophthalmic bleeding exhibited variations according
(19% vs. 7%). It is likely that some of the variation is
to sex, racial background, age, and frequency of aspirin use,
attributable to differences in question wording. For instance,
but these characteristics accounted for only an estimated 6–
the lower frequency of gum bleeding that we found probably
13% of the total variability in the reported frequencies of these
reflects the requirement in our questionnaire, but not in those
six symptoms. Our findings suggest that the definition of
of other authors, that the gum bleeding last at least 5 min.
ÔnormalÕ bleeding that is not sex-specific varies relatively little
Differences in the populations studied may also contribute to
by sex, race, age, or aspirin use; thus, it remains to be
Ó 2010 International Society on Thrombosis and Haemostasis
Although women reported a higher median number of
easy bruising and heavy menses were more common among
symptoms than men when viewed from the standpoint of all
infrequent aspirin users than among frequent aspirin users,
bleeding symptoms, this difference did not persist after
with non-users having intermediate values. We have no simple
exclusion of sex-specific questions (e.g. menstrual bleeding
explanation for this finding, but frequent aspirin use was
and postpartum bleeding). Thus, bleeding scores that are based
reported by only 10% of responders, and it is possible that
on the number of bleeding symptoms need to be adjusted for
individuals with heavy menses or easy bruising who were
sex, as is done, for example, with the Vicenza bleeding score for
frequent aspirin users had been counseled to reduce their
VWD [4]. Easy bruising and bruising after venipuncture were,
aspirin intake. Unfortunately, the aspirin primary prevention
however, more common in women than in men, a finding that
studies noted above did not report the frequency of heavy
is consistent with the study by Wahlberg et al. [13], in which
women reported a higher frequency of spontaneous bruising
There is an apparent contradiction between the finding that
than men. It is also consistent with studies of primary aspirin
men and women reported similar total numbers of non-sex-
prophylaxis, where the reported frequencies of excessive
specific symptoms and the finding that women reported higher
bruising among the control groups not taking aspirin were
frequencies of easy bruising and venipuncture bruising. The
43% among women [23] and 9–13% among men [24,25].
reason why the increased frequency of bruising in women did
The literature on differences in bleeding symptoms as a
not affect the median value for all symptoms was that it was
function of race and ethnicity is sparse. In the only study
counterbalanced by statistically insignificant increases in
identified that addressed these issues, the authors found a lower
symptom frequencies among men in several categories (gum
frequency of epistaxis among Asians than among Caucasians
bleeding, lip bleeding, tooth extraction bleeding, hemoptysis,
[18], a finding that we did not observe. We found that epistaxis
minor cut bleeding, hematochezia, melena, eye bleeding,
and ophthalmic bleeding were reported with lower frequency
surgical bleeding, and trauma bleeding). Similarly, although
by African-Americans than by Caucasians. It is possible that
we observed differences in several symptoms by race or
this difference can be explained by the higher von Willebrand
frequency of aspirin use, the total number of symptoms did not
factor levels reported in African-Americans than in Caucasians
vary by race, age, or frequency of aspirin use, despite
[26–28], as epistaxis is a cardinal symptom of VWD [1,4].
statistically insignificant variations within individual categories.
However, the African-American women in our population did
The Vicenza group has demonstrated the diagnostic and
not report a lower frequency of heavy menses, another
prognostic utility of their questionnaire for VWD [4–6]. Based
common manifestation of VWD [4,29], than Caucasian
on their experience and expertise, they excluded from consid-
eration all bleeding symptoms that they defined as Ôtrivial,Õ and
As our bleeding history questionnaire is based on the
devised their bleeding score on the basis of the severity of
cumulative prevalence of a list of symptoms, we considered the
individual symptoms. Our questionnaire, in contrast, includes
possibility that older individuals would report more symptoms
questions on both major and minor bleeding symptoms. This
because they had more time in which to experience symptoms.
explains why we found a lower percentage of healthy individ-
Although a correlation between increasing age and higher
uals who did not report any bleeding symptoms (26%) than did
bleeding scores has been reported in individuals with bleeding
the Vicenza group (77%) [4]. We are currently employing our
disorders, previous reports have not found this correlation in
questionnaire to identify the symptoms of patients with mild
healthy individuals [4,5]. We also found few associations
bleeding disorders, and will compare these data with the data
between older age and more bleeding symptoms in our healthy
that we have obtained in the healthy adult cohort described in
adult population. Paradoxically, we found a modest decrease in
this study, using several different statistical methods.
the reported frequency of epistaxis with age, suggesting either
Because the reliability of medical histories depends on the
that epistaxis is becoming more common or that older
ability of subjects to recall symptoms over their entire lifetimes
individuals are less likely to remember episodes of epistaxis
and to report the data consistently, these studies will also
from their youth. We also found an increase in the reported
evaluate measures of questionnaire validation such as test–
frequency of dark stools with age. However, among the
retest and inter-rater reliability. In the current study, we chose
individuals who reported dark stools, the symptom could be
to use a comprehensive questionnaire, despite its length,
classified with reasonable certainty as melena in only 6% of
because we did not want to prejudge which questions would
cases. This highlights the limited utility of just inquiring about
have the best diagnostic and prognostic value. Going forward,
dark stools, and thus the importance of following up screening
we will compare the responses of the healthy adults in this
questions with questions that provide more details.
study with those of patients with bleeding disorders, so as to
Although aspirin use has been reported to increase the
identify those questions that are most reliable and/or of the
frequency of a number of bleeding symptoms, including easy
greatest diagnostic value. We will then create a shorter
bruising (which ranged from 9% to 43% in controls and from
questionnaire that focuses on obtaining the most valuable
14% to 53% in studies on aspirin in primary prevention studies
data. The potential advantages and drawbacks of our approach
[23–25]), we did not exclude individuals taking aspirin, because
we wanted a sample that represented as closely as possible the
The long-term goal of our research is to standardize the
demographics of our community. Unexpectedly, we found that
collection of bleeding histories by developing Web-based
Ó 2010 International Society on Thrombosis and Haemostasis
Bleeding symptoms in healthy individuals 107
instruments that can be used by investigators across different
boom J, Schneppenheim R, Budde U, Ingerslev J, Vorlova Z, Habart
sites and studies. This has the potential to aggregate large
D, Holmberg L, Lethagen S, Pasi J, Hill F, et al. A quantitativeanalysis of bleeding symptoms in type 1 von Willebrand disease:
amounts of de-identified phenotypic data, so as to increase the
results from a multicenter European study (MCMDM-1 VWD).
power to detect scientifically and medically important correla-
tions with genetic and environmental data. As a first step in this
6 Tosetto A, Castaman G, Rodeghiero F. Evidence-based diagnosis of
process, an electronic version of our questionnaire is available
type 1 von Willebrand disease: a Bayes theorem approach. Blood 2008;
to investigators at https://ds9.rockefeller.edu/RUBHPSR/.
7 Federici AB, Mannucci PM, Castaman G, Baronciani L, Bucciarelli P,
Canciani MT, Pecci A, Lenting PJ, De Groot PG. Clinical and
molecular predictors of thrombocytopenia and risk of bleeding inpatients with von Willebrand disease type 2B: a cohort study of 67
We would like to thank D. Rubin and M. Musen of Stanford
patients. Blood 2009; 113: 526–34.
University and S. Mollah of Rockefeller University for their
8 Bowman M, Mundell G, Grabell J, Hopman WM, Rapson D,
Lillicrap D, James P. Generation and validation of the Condensed
valuable conceptual and practical contributions to the design of
MCMDM-1VWD Bleeding Questionnaire for von Willebrand disease.
the Bleeding History Phenotyping System, D. Brassil and D.
Bernal-Messinger for their assistance in administering the
9 Bowman M, Riddel J, Rand ML, Tosetto A, Silva M, James PD.
Bleeding History Questionnaire, and the staff and patients of
Evaluation of the diagnostic utility for von Willebrand disease of a
the Metropolitan Family Health Center Network (P. Beaty,
pediatric bleeding questionnaire. J Thromb Haemost 2009; 7:1418–21.
10 Biss TT, Blanchette VS, Clark DS, Bowman M, Wakefield CD, Silva M,
Chief Medical Officer) and the Newark Community Health
Lillicrap D, James PD, Rand ML. Quantitation of bleeding symptoms
Centers, Inc. (N. Tham, Chief Medical Officer) for their
in children with von Willebrand disease: use of a standardized pediatric
bleeding questionnaire. J Thromb Haemost 2010; 8: 950–6.
11 Plug I, Mauser-Bunschoten EP, Brocker-Vriends AH, van Amstel
HK, van der Bom JG, van Diemen-Homan JE, Willemse J, Rosendaal
FR. Bleeding in carriers of hemophilia. Blood 2006; 108: 52–6.
12 Dilley A, Drews C, Miller C, Lally C, Austin H, Ramaswamy D,
In accord with federal law and the policies of the Research
Lurye D, Evatt B. von Willebrand disease and other inherited bleeding
Foundation of the State University of New York, B. S. Coller
disorders in women with diagnosed menorrhagia. Obstet Gynecol 2001;
has a royalty interest in abciximab (Centocor), and in accord
with federal law and the policies of the Mount Sinai School of
13 Wahlberg T, Blomback M, Hall P, Axelsson G. Application of indi-
Medicine, B. S. Coller has a royalty interest in the VerifyNow
cators, predictors and diagnostic indices in coagulation disorders. I. Evaluation of a self-administered questionnaire with binary questions.
assay system (Accumetrics). In addition, he is a consultant to
Methods Inf Med 1980; 19: 194–200.
Accumetrics and is an inventor of an aIIbb3 antagonist
14 Sramek A, Eikenboom JC, Briet E, Vandenbroucke JP, Rosendaal
compound identified by high-throughput screening. This study
FR. Usefulness of patient interview in bleeding disorders. Arch Intern
was supported by grants KL2RR024142 and UL1RR024143
from the National Center for Research Resources (NCRR), a
15 Nosek-Cenkowska B, Cheang MS, Pizzi NJ, Israels ED, Gerrard JM.
Bleeding/bruising symptomatology in children with and without
component of the National Institutes of Health (NIH), and the
bleeding disorders. Thromb Haemost 1991; 65: 237–41.
NIH Roadmap for Medical Research, as well as funds from
16 Quiroga T, Goycoolea M, Panes O, Aranda E, Martinez C, Belmont S,
Stony Brook University. The contents are solely the respon-
Munoz B, Zuniga P, Pereira J, Mezzano D. High prevalence of
sibility of the authors and do not necessarily represent the
bleeders of unknown cause among patients with inherited mucocuta-
neous bleeding. a prospective study of 280 patients and 299 controls. Haematologica 2007; 92: 357–65.
17 McKay H, Derome F, Haq MA, Whittaker S, Arnold E, Adam F,
Heddle NM, Rivard GE, Hayward CP. Bleeding risks associatedwith inheritance of the Quebec platelet disorder. Blood 2004; 104: 159–
1 Coller BS, Schneiderman PI. Clinical evaluation of hemorrhagic dis-
orders: the bleeding history and differential diagnosis of purpura. In:
18 Daniel M, Jaberoo MC, Stead RE, Reddy VM, Moir AA. Is admis-
Hoffman R, Benz EJ, Shattil SJ, Furie B, Silberstein LE, McGlave P,
sion for epistaxis more common in Caucasian than in Asian people? A
eds. Hematology: Basic Principles and Practice, 5th edn. New York:
preliminary study. Clin Otolaryngol 2006; 31: 386–9.
Churchill Livingstone, 2004: 1851–76.
19 National Institutes of Health. NIH policy on reporting race and
2 Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the
ethnicity data: subjects in clinical research. http://grants.nih.gov/
assessment of bleeding risk prior to surgery or invasive procedures.
grants/guide/notice-files/not-od-01-053.html. Accessed 13 September
British Committee for Standards in Haematology. Br J Haematol
20 Mauer AC, Barbour EM, Khazanov NA, Levenkova N, Mollah SA,
3 Eckman MH, Erban JK, Singh SK, Kao GS. Screening for the risk for
Coller BS. Creating an ontology-based human phenotyping system:
bleeding or thrombosis. Ann Intern Med 2003; 138: W15–24.
the Rockefeller University bleeding history experience. Clin Transl Sci
4 Rodeghiero F, Castaman G, Tosetto A, Batlle J, Baudo F, Cappelletti
A, Casana P, De BN, Eikenboom JC, Federici AB, Lethagen S, Linari
21 Bodenreider O. The Unified Medical Language System (UMLS):
S, Srivastava A. The discriminant power of bleeding history for the
integrating biomedical terminology. Nucleic Acids Res 2004; 32: D267–
diagnosis of type 1 von Willebrand disease: an international,
multicenter study. J Thromb Haemost 2005; 3: 2619–26.
22 Tabachnick BG, Fidell LS. Logistic regression. In: Tabachnick BG,
5 Tosetto A, Rodeghiero F, Castaman G, Goodeve A, Federici AB,
Fidell LS, eds. Using Multivariate Statistics, 5th edn. New York: Allyn
Batlle J, Meyer D, Fressinaud E, Mazurier C, Goudemand J, Eiken-
Ó 2010 International Society on Thrombosis and Haemostasis
23 Ridker PM, Cook NR, Lee IM, Gordon D, Gaziano JM, Manson JE,
age, race, sex, and risk factors for atherosclerosis. The Atherosclerosis
Hennekens CH, Buring JE. A randomized trial of low-dose aspirin in
Risk in Communities (ARIC) Study. Thromb Haemost 1993; 70: 380–
the primary prevention of cardiovascular disease in women. N Engl J
29 Kadir RA, Economides DL, Sabin CA, Owens D, Lee CA. Frequency
24 Steering Committee of the PhysiciansÕ Health Study Research Group.
of inherited bleeding disorders in women with menorrhagia. Lancet
Final report on the aspirin component of the ongoing PhysiciansÕ
Health Study. N Engl J Med 1989; 321: 129–35.
30 Wahlberg TB. A method for the evaluation of clinical information,
25 The Medical Research Council’s General Practice Research Frame-
exemplified for bleeding symptoms in non-severe von WillebrandÕs
work. Thrombosis prevention trial: randomised trial of low-intensity
disease type I. Methods Inf Med 1984; 23: 143–6.
oral anticoagulation with warfarin and low-dose aspirin in the primary
31 Mauser Bunschoten EP, van Houwelingen JC, Sjamsoedin Visser EJ,
prevention of ischaemic heart disease in men at increased risk. Lancet
van Dijken PJ, Kok AJ, Sixma JJ. Bleeding symptoms in carriers of
hemophilia A and B. Thromb Haemost 1988; 59: 349–52.
26 Miller CH, Haff E, Platt SJ, Rawlins P, Drews CD, Dilley AB, Evatt B.
32 Drews CD, Dilley AB, Lally C, Beckman MG, Evatt B. Screening
Measurement of von Willebrand factor activity: relative effects of ABO
questions to identify women with von Willebrand disease. J Am Med
blood type and race. J Thromb Haemost 2003; 1: 2191–7.
27 Green D, Ruth KJ, Folsom AR, Liu K. Hemostatic factors in the
33 Friberg B, Orno AK, Lindgren A, Lethagen S. Bleeding disorders
Coronary Artery Risk Development in Young Adults (CARDIA)
among young women: a population-based prevalence study. Acta
Study. Arterioscler Thromb 1994; 14: 686–93.
Obstet Gynecol Scand 2006; 85: 200–6.
28 Conlan MG, Folsom AR, Finch A, Davis CE, Sorlie P, Marcucci G,
Wu KK. Associations of factor VIII and von Willebrand factor with
Ó 2010 International Society on Thrombosis and Haemostasis
Any alteration in adverse factors can take 10-12 weeks to show an normal fertilisation after intercourse, but cannot be guaranteed to do so. A poor swim up has less than 4 million/ml rapidly motile sperm and would be unlikely to achieve fertilisation after normal intercourse or standard in-vitro Parameters measured in sperm function tests fertilisation (IVF). Persistently poor sperm swim u
Tanzanian Travel Information Th outlines is intended to be a brief outline of things you'll need to consider when traveling to Tanzania including approximate costs. Quoted here in Canadian dollars but in Tanzania the currency is Tanzanian shilling or USD. Flights: Between $1800.-2200.00/person- Vancouver/ Amsterdam/ Kilimanjaro,Tanzania. May go through Seattle. Try to avoid Amst
 Bleeding symptoms in healthy individuals 105
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Number of symptoms, excluding sex-specific symptoms
Fig. 1. Number of bleeding symptoms in men and women. (A) Men reported fewer bleeding symptoms than women (P < 0.01 by Mann–Whitney U-test). (B) When heavy menses, treatment for heavy menses, bleeding during pregnancy, bleeding at delivery, postpartum bleeding and circumcision bleedingwere excluded, men and women reported similar frequencies of bleeding symptoms (P = 0.50 by Mann–Whitney U-test).
Bleeding symptoms in healthy individuals 105
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
Number of symptoms, excluding sex-specific symptoms
Fig. 1. Number of bleeding symptoms in men and women. (A) Men reported fewer bleeding symptoms than women (P < 0.01 by Mann–Whitney U-test). (B) When heavy menses, treatment for heavy menses, bleeding during pregnancy, bleeding at delivery, postpartum bleeding and circumcision bleedingwere excluded, men and women reported similar frequencies of bleeding symptoms (P = 0.50 by Mann–Whitney U-test).