Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
Annals of Hepatology 2007; 6(3): July-September: 190-193
Case Report Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
Nikolaos S. Salemis;1,2 Epameinondas Georgoulis;1 Stavros Gourgiotis;2 Efstathios Tsohataridis1
Abstract
10:1 ratio, with an age range 50-60 years.2-4 The vast ma-jority are asymptomatic being detected incidentally during
Spontaneous rupture of a non parasitic hepatic cyst is
abdominal imaging3 and are not associated with hepatic
an extremely rare occurrence. A 50 -year- old male,
function abnormalities.5 Clinical symptoms occur in about
was admitted with typical clinical manifestations of
5% of the patients due to a progressive increase of cyst’s
acute surgical abdomen. At exploratory laparotomy, a
size, or the development of a complication.6 Complications
giant ruptured non parasitic cyst occupying the entire
of NPHC are unusual and may include intracystic hemor-
left liver lobe was found, along with a large amount of
rhage, torsion, infection, malignant transformation or com-
free intraperitoneal fluid. The cyst was widely un-
pression of adjacent structures resulting most commonly
roofed very close to the liver parenchyma. The patient
in obstructive jaundice.7,8 More rarely, spontaneous rup-
had an uneventful postoperative course and was dis-
ture,9,10 inferior vena cava thrombosis11 and acute pulmo-
charged six days later. The clinical presentation, diag-
nary embolism,12 have all been reported. We herein de-
nostic evaluation and surgical management of this ex-
scribe the case of a spontaneous rupture of a giant non-
tremely rare clinical entity are discussed, along with a
parasitic hepatic cyst in a 50 year old male, who presented
review of the literature. This case, which according to
with acute surgical abdomen and was successfully treat-
our best knowledge is the fourth reported in the litera-
ed with open wide unroofing. To our knowledge, this case
ture, highlights the considerable risk of serious com-
appears to be the fourth reported in the literature. plications associated with the presence of a large symp- tomatic nonparasitic hepatic cyst. Prophylactic treat- Case presentation ment should be considered in all these cases.
A 50- year- old male was admitted with a 4 hour history
Key words: Non parasitic hepatic cyst, spontaneous
of a sudden onset of severe abdominal pain, associated
rupture, acute abdomen.
with nausea and vomiting. Although the pain was initiallyepigastric, it progressively became generalized. He also
Introduction
complained of a dull epigastric pain and right upperguardant discomfort, which began to experience two
Non parasitic hepatic cysts (NPHC) are detected in
months prior to the current admission. His past medical
4.65% of the population, as a result of the increasing use
history included chronic obstructive pulmonary disease,
and refinement of abdominal imaging and ultrasonogra-
phy.1 They are encountered more often in women by a 4-
On clinical examination he was distressed, his abdo-
men was distended with marked diffuse tenderness,
1 Army Veterans General Hospital NIMTS.
guarding and rebound tenderness. Bowel sounds were ab-
sent. His blood pressure was 160/100 mmHg, pulse rate 90beats/minute and body temperature 37.6ºC. The haemo-
2nd Department of Surgery. Athens, Greece.
gram revealed a white cell count of 15,100 x103/ML with
91.3% neutrophils, a haemoglobin level of 14.2 g/dL and a
platelet count of 231 x 103/mL. Liver function tests were
normal. Abdominal ultrasonography demonstrated echo-
patterns consistent with a large cystic lesion occupying
almost the entire left liver lobe as well as fluid in the peri-
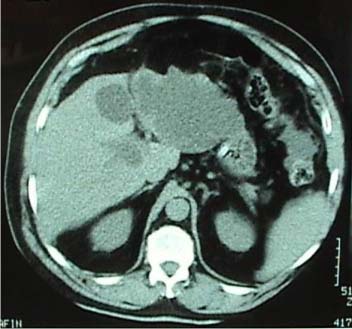
toneal cavity. Abdominal computerized tomographic (CT)
scans confirmed the presence of a huge homogeneous
cyst with irregular borders in the left live lobe measuring
17 x 12 cm (Figure 1) and free intraperitoneal fluid espe-
Manuscript received and accepted: 25 June and 12 July 2007
cially in the lower abdomen (Figures 2 and 3). NS Salemis et al. Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
At emergency exploratory laparotomy, a giant rup-
the possibility of spontaneous regression.16 The most
tured cyst that occupied the left liver lobe was found and
common presenting features in symptomatic patients are
approximately 1,000 mL of intraperitoneal fluid were as-
epigastric pain, nausea, vomiting, a feeling of fullness or
pirated. A wide excision of the cyst was undertaken very
close to the liver parenchyma. A running locking suture
To our knowledge, only 14 cases of spontaneous rup-
was used along the edge of the resected cyst wall, in order
ture of NPHC have been reported in the English litera-
to prevent bleeding and bile leakage. Intraoperative fro-
ture.9,15 Sudden abdominal pain was the most frequent
zen section of multiple specimens from the cystic wall
symptom in 13 cases, while one patient was asymptomat-
showed no evidence of malignancy, while cytology and
ic. We were able to find only three cases of patients who
cultures of the cystic fluid were negative. Serological
developed acute abdomen following spontaneous rupture
tests for echinococcus as well as tumor markers includ-
of a NPHC.18-20 Our case appears to be the fourth reported.
ing CEA and CA 19/9 were negative. Histological exam-
Several therapeutic approaches have been described
ination of the entire resected specimen measuring 27 x
for the management of NPHC, including guided aspiration
12 cm confirmed the diagnosis of a benign non hydatid,
with or without injection of a sclerosant, open unroofing,
non neoplastic simple liver cyst. The patient had an un-eventful postoperative course and was discharged sixdays later. Follow-up examinations performed six andtwelve months after surgery showed no findings of recur-rence. Discussion
Benign nonparasitic hepatic cysts are rare congenital
lesions that arise from the development of aberrant intra-hepatic bile ducts in utero and are lined with cuboidalepithelium.13 They can be classified as congenital or ac-quired. Congenital cysts can be further divided into soli-tary benign nonparasitic cysts, polycystic liver disease,or Caroli’s disease. The acquired type includes neoplas-tic, traumatic and infectious cysts.14 The majority of he-patic cysts remain asymptomatic and managed conserva-tively,2,15 due to the risk of complications in therapy and
Figures 2 and 3. Computerized tomographic scan demonstrates Figure 1. Computerized tomographic scan demonstrates a huge
the presence of free intraperitoneal fluid, especially in the lower
cyst with irregular borders, occupying the left liver lobe. Annals of Hepatology 6(3) 2007: 190-193
laparoscopic unroofing, radical excision, cyst enterosto-
In cases where the cystic fluid is bile stained and a
my, hepatic resection and liver transplantation.4,13,21 Prior
communication with the biliary tree is suspected, a cys-
to any kind of intervention, a thorough diagnostic evalu-
toenteric anastomosis using a Roux-en-Y jejunal loop is
ation is mandatory. Ecchinococcal serology should be
indicated.2,14,17 Intraperitoneal drainage in the above men-
obtained in all patients with cystic liver lesions and rare
tioned cases is unadvisable and usually results in the for-
cases of cystic tumors need to be excluded.6,14
mation of a postoperative biloma.14,21 However the con-
Ultrasonography or CT-guided cyst aspiration can be
struction of a Roux-en-Y cystoenterostomy carries a con-
easily performed in cysts larger than 5 cm in diameter,17
siderable risk of infectious complications and additional
but is associated with recurrence in 100% of the cases21-23
demanding surgery. Tocchi et al,21 reported that all three
and additionally carries a considerable risk of complica-
patients who underwent a cystojejunostomy, developed
tions. The only indications of the procedure are either pa-
relapsing cholangitis requiring repeated antibiotic treat-
tients with high operative risk or the need to perform a
ment, while in one patient hepatic resection due to septic
cytologic diagnosis.17 Additionally, it is a good thera-
complications was performed one year later. More radical
peutic test to ascertain whether abdominal symptoms are
procedures like hepatic resection and cystectomy have
related to the liver cyst14 in order to avoid an unnecessary
also been advocated in the management of NPHC. Al-
intervention.3 In order to destroy the secretory epithelial
though these procedures obtain the best results in terms
layer of the cyst, aspiration can be combined with the in-
of recurrence rate,4,17,21 they are however associated with
jection of a sclerosing agent such as ethanol, minocy-
increased morbidity, which may not be acceptable for a
cline chloride, or tetracycline chloride. This procedure
benign disease. Martin et al,4 reported a morbidity rate of
results to a much lower recurrence rate which may still be
50% among 16 patients who underwent hepatic resection
as high as 20%13 but should be considered only after a
for NPHC. Hepatic resections may be better reserved for
malignant or infectious etiology and a biliary communi-
patients with multiple recurrences or when a possibility of
cation have all been ruled out.2,21 However, series of this
a cystic tumor can not be ruled out.2,25 Radical cystectomy
technique involve small number of patients and insuffi-
is indicated in symptomatic cysts that can not be ade-
cient follow-up do not allow adequate evaluation of its
quately unroofed due to a small superficial component,14
while liver transplantation may be indicated in polycystic
Laparoscopic unroofing has been increasingly used in
liver patients with symptoms refractory to other therapeu-
the management of NPHC. Various studies have shown
tic approaches or with combined renal failure.2
that it is associated with reduced morbidity, shorter hospi-
In conclusion, we describe an extremely rare case of a
tal stay and more rapid return to normal activity, when
spontaneous rupture of a huge nonparasitic hepatic cyst
compared with open unroofing.24 Laparoscopic treatment
in a male patient who presented with clinical manifesta-
has been also been reported in the emergency setting,
tions of acute surgical abdomen. Prophylactic treatment
with good results.15 The two methods appear to have al-
should be considered in symptomatic large non parasitic
most similar recurrence rates.2,4,17,21,22 These findings are
hepatic, cysts as they carry a considerable risk of serious
however influenced by case selection and should be treat-
complications. Adequate patient selection is of great im-
ed with some caution.2,4 Additionally larger periods of fol-
portance for achieving acceptable long term results.
low-up are also necessary.4 Gigot et al,3 in a series of 26patients found that laparoscopic fenestration was techni-
References
cally feasible in 94% of the cases. Various factors that
Caremani M, Vincenti A, Benci A, Sassoli S, Tacconi D.
may affect recurrence have been identified, including in-
Echographic epidemiology of non-parasitic hepatic cysts. J Clin
adequate extent of deroofing, deep cysts and cysts in
Ultrasound 1993; 21: 115-118.
posteriors segments of the liver, the use of an argon beam
Garcea G, Pattenden CJ, Stephenson J, Dennison AR, Berry DP. Nine-year single-center experience with nonparasitc liver cysts:
coagulator for the remaining cystic wall epithelium, omen-
diagnosis and management. Dig Dis Sci 2007; 52: 185-191.
toplasty for the residual cavity and previous laparoscopic
Gigot JF, Legrand M, Hubens G, de Canniere L, Wibin E, Deweer
treatment or open fenestration which has resulted in
F, Druart ML, Bertrand C, Devriendt H, Droissart R, Tugilimana
dense adhesions formation.3 Consequently, adequate pa-
M, Hauters P, Vereecken L. Laparoscopic treatment of nonpara-sitic liver cysts: adequate selection of patients and surgical tech-
tient selection and type of cystic disease are crucial be-
nique. World J Surg 1996; 20: 556-561.
Martin IJ, McKinley AJ, Currie EJ, Holmes P, Garden J. Tailoring
In order to improve the recurrence rate, Emmerman et
the management of nonparasitic liver cysts. Ann Surg 1998;
al6 combined laparoscopic radical deroofing with an
Katkhouda N, Mavor E. Laparoscopic management of benign
omental transposition flap. Omentum placement keeps the
liver disease. Surg Clin N Am 2000; 80: 1203-1211.
cavity open and has the ability to absorb fluid produced
Emmermann A, Zornig C, Lloyd DM, Peiper M, Bloechle C,
by the cystic epithelium. This operative technique was ap-
Broelsch CE. Laparoscopic treatment of nonparasitic cysts of
plied in 13 out of 18 patients of the study and resulted in
the liver with omental transposition flap. Surg Endosc 1997; 11:734-736.
0% recurrence rate, whereas in the group of patients
Ishikawa H, Uchida S, Yokokura Y, Iwasaki Y, Horiuchi H, Hiraki
where no omental flap was used the relative rate was 11%.
M, Kinoshita H, Shirouzou K. Nonparasitic solitary huge liver
NS Salemis et al. Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
cysts causing intracystic hemorrhage or obstructive jaundice. J
17. Koperna T, Vogl S, Satzinger U, Schulz F. Nonparasitic cysts of
Hepatobiliary Pancreat Surg 2002; 9: 764-768.
the liver: results and options of surgical treatment. World J Surg
Terada T, Notsumata K, Nakanuma Y. Biliary carcinosarcoma
arising in nonparasitic simple cyst of the liver. Virchows Archiv
18. Carels RA, van Bommel EFH. Ruptured giant liver cyst: a rare
cause of acute abdomen in a haemodialysis patient with autoso-
Poggi G, Gatti C, Delmonte A, Teragni C, Bernardo G. Spontane-
mal dominant polycystic kidney disease. Neth J Med 2002; 60:
ous rupture of non-parasitic hepatic cyst. Int J Clin Pract 2006;
19. Chung TK, Chen KS, Yen CL, Chen HY, Cherng WJ, Fang KM.
10. Yamaguchi M, Kuzume M, Matsumoto T, Matsumiya A, Nakano
Acute abdomen in a haemodialyzed patient with polycystic kid-
H, Kumada K. Spontaneous rupture of a nonparasitic liver cyst
ney disease-rupture of a massive liver cyst. Nephrol Dial Trans-
complicated by intracystic hemorrhage. J Gastroenterol 1999;
20. Morano C, Fornari L, Persico SL. Acute abdomen caused by the
11. Torzilli G, Santambrogio R, Vellini S, Palmisano A, Donadon M,
rupture of a solitary non-parasitic cyst of the liver. Minerva Chir
Cornalba G. Montorsi. Inferior vena cava thrombosis: an un-
usual complication of a large simple non-parasitic liver cyst re-
21. Tocchi A, Mazzoni G, Costa G, Cassini D, Bettelli E, Agostini N,
quiring an intergrated approach. Hepatogastroenterology 2003;
Miccini M. Symptomatic nonparasitic hepatic cysts. Arch Surg
12. Buyse S, Asselah T, Vilgrain V, Paradis V, Sauvanet A, Consigny
22. Regev A, Reddy KR, Berho M, Sleeman D, Levi JU, Livingstone
Y, Dufour V, Fantin B, Valla D, Marcellin P. Acute pulmonary
AS, Levi D, Ali U, Molina E, Schiff ER Large cystic lesions of the
embolism: a rare complication of a large non-parasitic hepatic
liver in adults: a 15-year experience in a tertiary center. J Am Col
cyst. Eur J Gastroenterol Hepatol 2004; 16: 1241-1244.
13. Knauer EM, Sweeney JF. Cystic disease of the liver. In: Cameron,
23. Saini S, Mueller PR, Ferrucci JT Jr, Simeone JF, Wittenberg J,
JL (ed) Current surgical therapy. Eighth Edition. Philadelphia,
Butch RJ. Percutaneous aspiration of hepatic cysts does not pro-
vide definitive therapy. Am J Roentgenol 1983; 141: 559-560.
14. Cowles RA, Mulholland MW. Solitary hepatic cysts. J Am Col
24. Tan YM, Chung A, Mack P, Chow P, Klin LW, Ooi LL. Role of
fenestration and resection for symptomatic solitary liver cysts.
15. Cheung FKY, Lee KF, Wong J, Lai PBS. Emergency laparoscopic
unroofing of a ruptured hepatic cyst. JSLS 2005; 9: 497-499.
25. Kitajima Y, Okayama Y, Hirai M, Hayashi K, Imai H, Okamoto T,
16. Arai H, Nagamine T, Suzuki H, Shimoda R, Abe T, Yamada T,
Aoki S, Akita S, Gotoh K, Ohara H, Nomura T, Joh T, Yokoyama
Takagi H, Mori M. Simple liver cyst with spontaneous regression.
Y, Itoh M. Intracystic hemorrhage of a simple liver cyst mimicking
J Gastroenterol 2002; 37: 755-757.
a biliary cystadenocacinoma. J Gastroenterol 2003; 38: 190-193.
A physician should be consulted if Lyme disease is suspected. Only the rash is distinctive enough for a clinical diagnosis without laboratory confirmation. In the absence of an EM rash, Lyme disease may be difficult to diagnose because its symptoms and signs vary among individuals and can be similar to those of many other diseases. Conversely, other arthritic or neurologic diseases may be mis
When using batteries for energy storage, whether an off-grid or grid-tie with back-up power, therenewable energy system used to charge the batteries and the metering systems to monitorperformance must be properly configured for optimal performance. While there is a relativelylarge amount of information for programming the correct values in the battery charging systems,whether a charge controller o

 NS Salemis et al. Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
At emergency exploratory laparotomy, a giant rup-
the possibility of spontaneous regression.16 The most
tured cyst that occupied the left liver lobe was found and
common presenting features in symptomatic patients are
approximately 1,000 mL of intraperitoneal fluid were as-
epigastric pain, nausea, vomiting, a feeling of fullness or
pirated. A wide excision of the cyst was undertaken very
close to the liver parenchyma. A running locking suture
To our knowledge, only 14 cases of spontaneous rup-
was used along the edge of the resected cyst wall, in order
ture of NPHC have been reported in the English litera-
to prevent bleeding and bile leakage. Intraoperative fro-
ture.9,15 Sudden abdominal pain was the most frequent
zen section of multiple specimens from the cystic wall
symptom in 13 cases, while one patient was asymptomat-
showed no evidence of malignancy, while cytology and
ic. We were able to find only three cases of patients who
cultures of the cystic fluid were negative. Serological
developed acute abdomen following spontaneous rupture
tests for echinococcus as well as tumor markers includ-
of a NPHC.18-20 Our case appears to be the fourth reported.
NS Salemis et al. Spontaneous rupture of a giant non parasitic hepatic cyst presenting as an acute surgical abdomen
At emergency exploratory laparotomy, a giant rup-
the possibility of spontaneous regression.16 The most
tured cyst that occupied the left liver lobe was found and
common presenting features in symptomatic patients are
approximately 1,000 mL of intraperitoneal fluid were as-
epigastric pain, nausea, vomiting, a feeling of fullness or
pirated. A wide excision of the cyst was undertaken very
close to the liver parenchyma. A running locking suture
To our knowledge, only 14 cases of spontaneous rup-
was used along the edge of the resected cyst wall, in order
ture of NPHC have been reported in the English litera-
to prevent bleeding and bile leakage. Intraoperative fro-
ture.9,15 Sudden abdominal pain was the most frequent
zen section of multiple specimens from the cystic wall
symptom in 13 cases, while one patient was asymptomat-
showed no evidence of malignancy, while cytology and
ic. We were able to find only three cases of patients who
cultures of the cystic fluid were negative. Serological
developed acute abdomen following spontaneous rupture
tests for echinococcus as well as tumor markers includ-
of a NPHC.18-20 Our case appears to be the fourth reported.