Do you want to buy antibiotics online without prescription? https://buyantibiotics24h.net/ - This is pharmacy online for you!
3000health.com
Ankylosing Spondylitis Testing found more than six times the expected amount of Lead in the patient’s body along with other harmful toxic metals that carry a long list of side effects and slow the healing process! In just 3 months-
Off All Prescriptions Including
Grew 2 inches and gained 10 lbsInitial Symptoms-
Increasing Joint Pain/Stiffness“When diagnosed with a long-term possibly debilitating condition like this, it’s important to note that pharmaceutical drugs are not the only option. By pinpointing exactly what essential elements were missing and locating stores of toxins, we were able to correct the problem and allow this 14-year old patient to live pain free!” -Dr. Van D. Merkle Patient Profile: 10-14-05 -The 14-year old patient presented with swollen ankles, an
inflamed right knee, some weight loss, noticeable fatigue and a
problem with loose stools (2-3 times per day). At the time of
the initial visit, he weighed 118 lbs at 5’4” and his blood pressure was 99/64. About five months before, the patient
started having gastro/intestinal problems followed by a gradual increase in joint swelling specifically around the knees and
ankles. He bounced between several experts who did extensive
testing for arthritis and bacterial infections along with x-rays. They began prescribing medication to inhibit the swelling and
loose stool movements in September, but none helped and the patient was forced to quit playing JV basketball due to the daily
By the time he arrived in our office a month later, he had
already tried Valtrax, Prednisone, Voltaren, Cipro, and z-pak,and was still taking Relafen and Flagyl on a daily basis. When
we first saw him, the patient also suffered from frequent canker sores and fever blisters, inflamed gums around his braces,
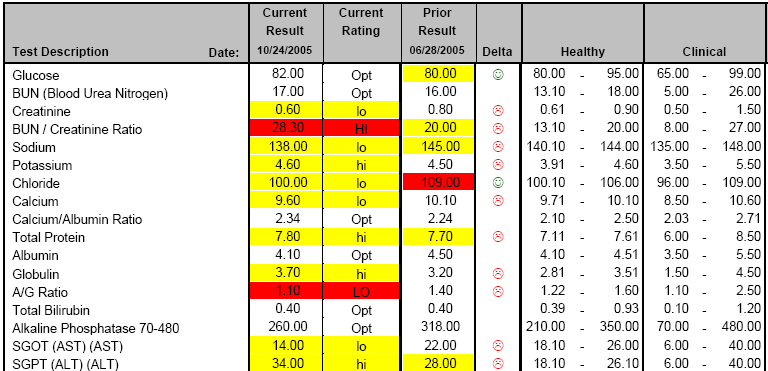
Patient’s tests results: 10-24-05 – A few days before his initial visit, the patient had a series of
blood tests done at a local hospital so I used these as a base for our analysis and did a comparison to earlier blood work he had
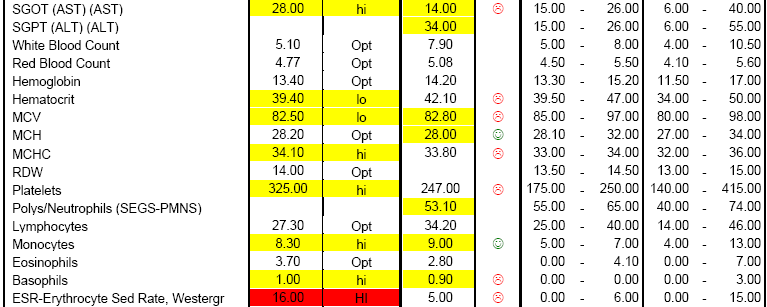
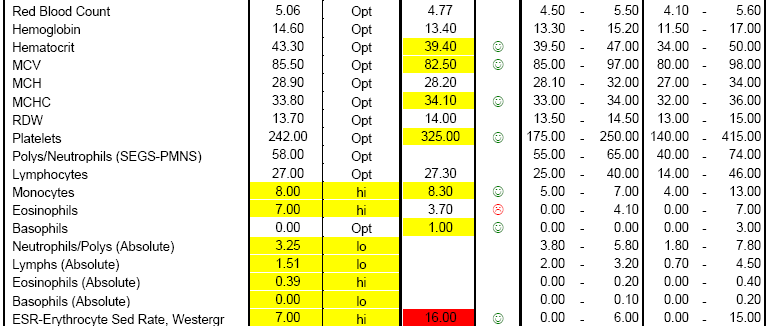
done at the same hospital in June. Looking at the chart below, 11 blood values became worse in a little less than 4 months
indicating that whatever the problem was, it was getting worse
despite or perhaps due to the medications his doctors recommended. The most significant findings were the low AST
and Polys/Neutrophils and the high Monocytes and ALT.
Results of Initial Blood Test:
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal.
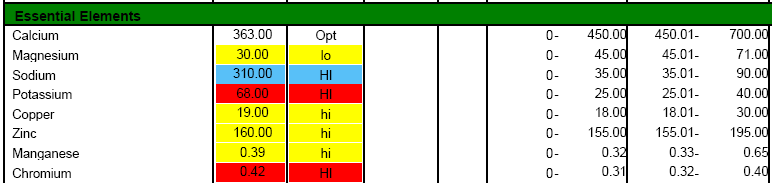
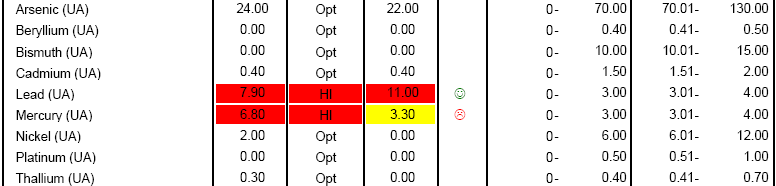
Several deficiencies/imbalances showed up in the patient’s hair
test results suggesting a difficulty for the body to heal and repair. High amounts of several toxic elements were also
present, most notably arsenic and lead, which may have
partially caused the depletion of several essential elements
including Lithium, Phosphorus, Selenium and Strontium. Lead’s
biggest outlet is actually the urine so we’ll conduct a UA mineral test to see how efficiently this toxin is being eliminated. The
high levels of Sodium may be due to the patient bathing in soft water. Results of Initial Hair Test:
Blue = clinically very high or clinically very low
Red = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal.
High levels of toxic elements can be further seen in the results
of the UA Mineral test. The column labeled ‘Prior Result’
represents the body’s ability to flush out toxic elements. The column labeled ‘Current Result’ is the amount of toxins leaving
the body with the help of the chelating agent DMSA. These tests show that the patient is unable to efficiently eliminate
heavy toxic metals like lead and mercury on his own. The
chelating agent was able to pull out more than six times the expected limit of lead and since most lead is excreted in the
urine, this shows a very large burden on the body. Results of Initial UA Mineral Test:
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal.
In addition to the above tests, we also conducted a urinalysis,
saliva test and metabolic urinalysis. These tests showed a slight infection, mild toxicity associated with the liver, gastrointestinal
involvement, a low pH, and vitamin C and calcium deficiency. Ablood test for the HLA-B27 gene also came back positive
leading to the diagnosis of Ankylosing Spondylitis. Doctor analysis: 10-26-05 – This teenager was suffering from two main problems: His body
was clogged with an array of toxic elements which slowed his
body’s ability to heal and deprived it of several essential elements; and he suffered from an arthritic disorder and
systemic rheumatic disease known as Ankylosing Spondylitis. This condition often appears between a person’s early teens up
to their 30’s, typically after some kind of bacterial infection. The
body activates its immune system to clear out the infection, but is then unable to turn back off leading to chronic tissue
inflammation, pain and stiffness in the joints.
The slightly high Globulin and low A/G ratio in the blood
illustrate signs of that inflammation and the low levels of Chloride and Calcium along with the high Monocytes partially
account for the patient’s Gastro/Intestinal Dysfunction. Tie that in with a load of toxic chemicals which are know to cause
weight loss, fatigue, joint pain, liver and kidney degeneration
and it’s no wonder he didn’t feel well!
A high SGPT and a low SGOT in the patient’s blood work
indicate possible liver inflammation or dysfunction, but these
also could be caused by his medications or high levels of toxins.
As the patient improves and his need for medication decreases, we’ll be able to better asses these two values. I recommended
alternating cycles of the chelating agent DMSA along with a
series of minerals and supplements which showed as deficient in the patient’s test results. As the toxic element burden is
eliminated from the body, the patient should notice a reduction in swelling and joint pain and a boost in energy. Patient assessment: 11-04-05 – The patient had two more partial blood tests done in 2005, the
first of which on 11-04 again shows how quickly his condition
was progressing. The ESR, which is an indicator of inflammation
jumped from 5 to 16 in less than two weeks. This was before the patient started taking vitamins and following the chelation
Results of 2nd Blood Test:
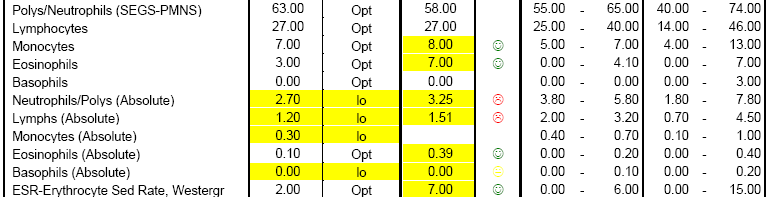
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal. 12-29-05 –A third blood test was done about two months later as the
patient neared the end of his chelation cycle. Many values
improved including the ESR rate which came down nine points
and the Monocytes and basophils neared their optimal healthy ranges. The SGOT and SGPT both became worse and eosinophils
also increased but these were all likely due to the high amounts of toxins being flushed out of the body. Results of 3rd Blood Test: Results of 3rd Blood Test Cont:
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal.
Around the time he completed the third blood test, the patient
also retested the UA minerals. The chelating agent DMSA pulled out smaller amounts of Lead and Mercury meaning there are
less of these toxic elements in the body, but there is still work
to be done. As the levels of the heaviest toxic elements are further reduced, the other lighter toxic metals will begin to
Results of 2nd UA Mineral Test:
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal. 01-23-06 – The patient is now off all medications and doing well but did
start probiotics to help an inflamed colon. He has grown 2
inches since November which surprised his rheumatologist, who
is still urging the patient to take medication. There has been a
reduction in swelling around the ankles and the patient
continues to see improvements with joint pain and stiffness. I recommended he give his body a little rest, and then do
another chelation cycle to pull out additional levels of toxic elements and retest the UA minerals in about 10 weeks. 04-15-06 – I reduced the DMSA dosage for this chelation cycle after the
patient noticed an increase in swelling and joint pain during the
first three days. There are still high levels of lead coming out but now other heavy metals are following, showing that the
toxic element reserves are being eliminated from the body. I
recommended the patient wait six weeks, then do another round of chelation and continue taking all other recommended
Results of 3rd UA Mineral Test:
Blue = clinically very high or clinically very lowRed = clinically high or clinically lowYellow = a little high or a little low; this can be considered a warning sign that the value is not optimal. 06-23-06 – A Rheumatologist called the patient to discuss the results of an
MRI done on June 8th saying the patient had marked arthritis and tendonitis in his ankles, increased in the right. He
recommended Enbrel to curtail the inflammation process even though the patient has not had any pain of stiffness since mid-
February. His right knee has completely healed, his colon is
99% better and he started playing basketball again in school. I recommended the patient have some blood work done, as this
is a better indicator of current amounts of inflammation. Effects of previous inflammation and damage from arthritis can be
seen in an MRI, but blood tests are better indicators of current
inflammation. I ordered a comprehensive panel and asked them to hold off until those results were known before starting
07-17-06 – Creatine Kinase is a measure of muscle breakdown or
inflammation in the body and this high number was most likely caused by the Ankylosing Spondylitis. We have not tested this
before but because the patient was feeling better, I believe the CK has most likely come down. I would estimate it was well
over 1,000 back in September. The liver enzymes (SGOT &
SGPT) are still elevated but both have improved since December. The GGT which has not been tested before and is
associated with pancreas dysfunction is very low so I modified his nutrient list to help the liver enzymes come down and the
GGT go up. The Monocytes also normalized showing G/I
improvements. Overall, this patient showed great progress over the past year and as long as he maintains his healthy diet and
keeps up with the recommended vitamins, he should continue to see great improvements. Results of 4th Blood Test:
Blue = clinically very high or clinically very lowRed = clinically high or clinically low
Yellow = a little high or a little low; this can be considered a warning sign that the value is not optimal. From The Patient’s Parents:
I am so sorry for not getting back to you after your thoughtful phone
call a couple months ago. As far as we can tell C is doing GREAT!!!!! He went to his family doctor for a sports physical a couple weeks ago and he
said C looked great! We have not done any blood work for a long time, so we
should probably follow through with that to see if any thing shows up, but he is back to doing all he has done before. Right now he is participating in the
SNAPP program to help him prepare and get stronger for basketball. He played last year for the Junior Varsity team (actually was a starter) and had
a great season for not having played the year before. He has gotten quite a
bit taller, has gained weight but is still very thin which I contribute to hisactivities. He has not seen his rheumatologist for over a year, but he really
had nothing else to offer him but Enbrel and we chose not to do that. Cwould like to go see him just to show him how good his ankles look.
Needless to say, we are all very thankful for what has happened to C in
the last two years and how far he has come!! He is very good about taking his supplements, and actually gets concerned about what may happen if he
We would like to thank you for starting us down the right road to help C
recover. We will never know for sure what triggered all of his problems, but we greatly appreciate the caring people who helped in his recovery. You and
your staff have been great. Thank you again, and we look forward to
-Thanks again and God’s Blessings. Dr. Merkle’s Final Thoughts:
Ankylosing Spondylitis is often misdiagnosed in young teens because
the symptoms are very similar to athletic injuries and because each
individual tends to present with their own unique pattern and activity of the illness. The best tools for early diagnosis include a physical exam to locate
any inflammation or decreased range of motion and a blood test for the ESR,
CK and HLA-B27 gene. This hereditary gene appears in almost 95% of Ankylosing Spondolitis cases but is only a piece of the puzzle. While about
7% of the U.S. population carries the HLA-B27 gene, only 1% of the population develops Ankylosing Spondylitis. There is emerging evidence that
other factors (perhaps environmental) may add to a person’s risk for the
disease to become expressed. For example, a study done in Northern Scandinavia found 24% of the population carries the HLA-B27 gene yet only
This patient’s ability to eliminate toxic metals from his body is very low.
On the first UA mineral test, we actually saw no lead being eliminated from his system, then with the help of a chelating agent that number spiked to
more than six times the expected limit. Those toxins actually bind processes in the body, slowing its ability to heal. Exposure to these kinds of toxins may
be one of the triggers that sparked the Ankylosing Spondylitis.
Medical treatment for this condition traditionally starts with a series of
non-steroidal anti-inflammatory drugs (NSAIDs) followed by medications like sulfasalazine which suppress the body’s immune system. Newer treatments
considered to be “more effective” include drugs that actually attack a messenger protein of inflammation called TNF but patients are required to
take these drugs for life or face relapse. Image telling a 14-year old boy he
has to choose between a crippling arthritic condition or taking a prescription with unknown long-term side effects. Furthermore, neither of those options
would help remove the vast levels of toxic elements in his system. Instead of treating just the inflammation, we worked on the whole system, filling the
nutritional gaps with essential elements and minerals and working to
eliminate toxins from the patient’s body. Now he has virtually no pain and can do all the athletic things he enjoys. Dr. Van D. Merkle is a Certified Clinical Nutritionist and a Doctor of Chiropractic who has practiced in the Dayton, Ohio area for 25 years. A Diplomate on the American Chiropractic Board of Nutrition and a Diplomate on the Chiropractic Board of Internists, he is also a member of The International and American Association of Clinical Nutritionists. Dr. Merkle is available to speak with you about your health concerns. To set up your consultation and get started on the road to better health, please call the Back To Health Center at (937) 433-3241 or email mail@Bk2Health.com.
SERVIÇO AUTÔNOMO MUNICIPAL DE ÁGUA E ESGOTO – SAMAE - TIMBÓ – SC CONCURSO PÚBLICO - EDITAL No 001/2008 ANEXO III ¾ NÍVEL MÉDIO CONTEÚDOS PROGRAMÁTICOS E REFERÊNCIAS PARA AS PROVAS COM NÚCLEO COMUM Português para todos os cargos de Nível Médio 1. O texto : compreensão e interpretação. 2. Semântica : sentido e emprego dos vocábulos nos texto
Plak de hartjes in je agenda!MEER? MAIL mail@jeugdtheaterschoolzuidoost.nlCHECK www.jtszo.nl BEL 020 – 4000 771 SEE YOU!Eindpresentaties DanS- & muSical gRoepen 10+ tHeateR klaSSen baSiSklaSSen Sky HigHligHtS Stop je HoofD nooit Stop je HoofD nooit in een Spinnenweb in een Spinnenweb Aaliyah Abbygail Abigail Abraham Adanna Adeel Adja Aisha Akesha Akua Alaya Al
 By the time he arrived in our office a month later, he had
already tried Valtrax, Prednisone, Voltaren, Cipro, and z-pak,and was still taking Relafen and Flagyl on a daily basis. When
we first saw him, the patient also suffered from frequent canker sores and fever blisters, inflamed gums around his braces,
Patient’s tests results:
By the time he arrived in our office a month later, he had
already tried Valtrax, Prednisone, Voltaren, Cipro, and z-pak,and was still taking Relafen and Flagyl on a daily basis. When
we first saw him, the patient also suffered from frequent canker sores and fever blisters, inflamed gums around his braces,
Patient’s tests results: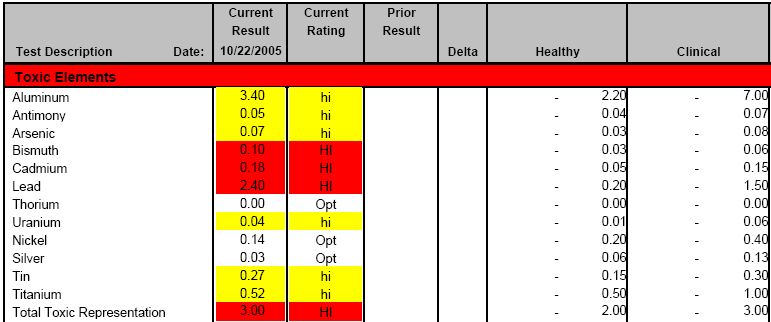
 including Lithium, Phosphorus, Selenium and Strontium. Lead’s
biggest outlet is actually the urine so we’ll conduct a UA mineral test to see how efficiently this toxin is being eliminated. The
high levels of Sodium may be due to the patient bathing in soft water.
including Lithium, Phosphorus, Selenium and Strontium. Lead’s
biggest outlet is actually the urine so we’ll conduct a UA mineral test to see how efficiently this toxin is being eliminated. The
high levels of Sodium may be due to the patient bathing in soft water.
 Results of Initial UA Mineral Test:
Results of Initial UA Mineral Test:

 alternating cycles of the chelating agent DMSA along with a
series of minerals and supplements which showed as deficient in the patient’s test results. As the toxic element burden is
eliminated from the body, the patient should notice a reduction in swelling and joint pain and a boost in energy.
alternating cycles of the chelating agent DMSA along with a
series of minerals and supplements which showed as deficient in the patient’s test results. As the toxic element burden is
eliminated from the body, the patient should notice a reduction in swelling and joint pain and a boost in energy.

 Results of 3rd Blood Test Cont:
Results of 3rd Blood Test Cont:
 reduction in swelling around the ankles and the patient
continues to see improvements with joint pain and stiffness. I recommended he give his body a little rest, and then do
another chelation cycle to pull out additional levels of toxic elements and retest the UA minerals in about 10 weeks.
reduction in swelling around the ankles and the patient
continues to see improvements with joint pain and stiffness. I recommended he give his body a little rest, and then do
another chelation cycle to pull out additional levels of toxic elements and retest the UA minerals in about 10 weeks.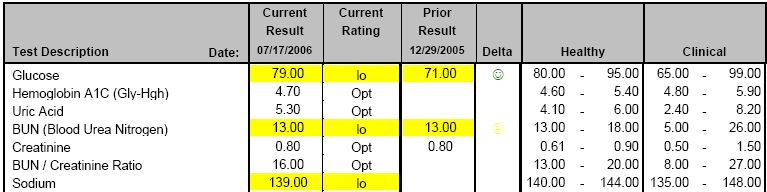


 07-17-06 – Creatine Kinase is a measure of muscle breakdown or
07-17-06 – Creatine Kinase is a measure of muscle breakdown or